PsyAndNeuro.ru
We present to your attention a review translation of clinical guidelines for the treatment of Alzheimer's disease and other dementias of the American Psychiatric Association. The material was prepared with the support of the Clinic of Psychiatry and Narcology Doctor SAN.
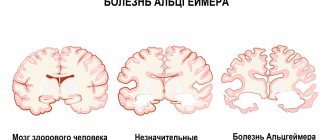
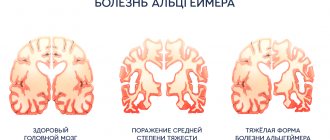
Alzheimer's disease is the most common form of dementia, a neurodegenerative disease first described in 1907 by German psychiatrist Alois Alzheimer. Typically, it is found in people over 65, but there is also early-onset Alzheimer's disease, a rare form of the disease. The global incidence in 2006 was estimated at 26.6 million people, and by 2050 the number of patients could quadruple.
Establishing a therapeutic alliance with the patient and family members
- The therapeutic alliance is fundamental to treatment.
- Since the patient is often unable to provide information about his condition, family members become a reliable source of such information.
- The behavior of caregivers affects the patient's condition, so the physician should treat them with care.
- It is necessary to determine in what situations it is necessary to talk with caregivers in the absence of the patient and how to behave during disputes between family members.
Patient and family education
- It is necessary to cover the following topics: diagnosis, symptoms, basic principles of care.
- Keep in mind that the willingness and ability to understand your diagnosis varies from patient to patient.
- Patients and their families need to be made aware that behavioral and neuropsychiatric features are part of the disease and are caused by brain damage.
- Caregivers may show signs of distress, such as increased irritability, social withdrawal, anxiety, depression, fatigue, insomnia, difficulty concentrating, and poor health.
Assessing the patient's physical health
- The patient's health assessment is coordinated with his or her physician.
- Physical health assessment helps identify the etiology of dementia and determine appropriate treatment.
ASSESSMENT PARAMETERS:
- Onset of the disease and development of symptoms.
- The patient's medical conditions and medications (including over-the-counter drugs and herbs).
- Functional abilities.
- Complete examination and detailed neurological examination.
- Psychiatric examination, including assessment of attention, memory, speech, visual functions.
- Psychiatric diagnoses in the past.
- Laboratory tests: complete blood count, biochemical blood test (glucose, electrolytes, calcium, kidney and liver function), vitamin B12 level, thyroid function. In some cases: toxicology studies, syphilis diagnosis, ESR, HIV test, homocysteine, lumbar puncture, EEG.
- For initial diagnosis, CT or MRI is recommended, especially for patients with subacute onset (less than a year), younger than 65 years, vascular risk factors, and the likelihood of focal lesions. The value of neuroimaging in late-stage disease has not been proven. Functional PET neuroimaging helps to clarify the diagnosis (eg differentiate Alzheimer's disease from frontotemporal dementia).
- Neuropsychological tests are useful for differentiated diagnosis of dementia, assessing the condition of a patient with mild or atypical symptoms, determining the severity of cognitive impairment and selecting treatment.
- Except in rare cases (CSF-14-3-3 protein in cases where Creutzfeldt-Jakob disease is suspected and stroke or viral encephalitis has been ruled out), biomarker studies have not been proven to be effective.
- Genes associated with certain types of dementia have been identified. Genetic testing is available but is generally not used for diagnosis.
Mental status assessment and monitoring
- During the course of their illness, 90% of patients with dementia develop behavioral and neuropsychiatric symptoms. Regular monitoring helps detect the appearance of new symptoms. It is especially important to monitor the patient's condition after changing the dose of medications.
- Symptoms to watch for: depression, suicidal ideation, hallucinations, delusions, agitation, aggression, loss of self-control, sexually inappropriate behavior, anxiety, apathy, appetite and sleep disturbances. You also need to monitor cognitive functions: memory, executive functions, speech, logic of reasoning, spatial orientation.
- Acute deterioration in mood, behavior, or cognitive function may be associated with delirium, an underlying medical condition (eg urinary tract infection, dehydration), pain, or physical or emotional discomfort. Before initiating treatment with psychotropic drugs or using physical control measures, a detailed assessment of the patient's condition should be carried out, unless it is an emergency.
Monitoring and improving security
- Patients living alone should be closely monitored. Signs that a patient can no longer live alone include repeated falls, hospitalizations, dehydration, poor nutrition, deteriorating living conditions and other signs of untidiness.
- All patients and their caregivers should be asked about suicidal ideation, plans, and attempts. In patients with dementia, suicidal ideation is more likely to appear early in the disease, when the ability to understand is preserved. Measures to prevent suicide are the same as for patients without dementia: psychotherapy, pharmacotherapy, removal of potential suicide weapons, enhanced supervision, hospitalization.
- Agitation (eg aggressiveness, conflict, threatening behavior, hyperactivity, loss of self-control) usually appears in the late stages of dementia and often has multiple causes. The first thing to do is to find out the reasons, which may include physical health problems, depression, psychosis, pain, hunger, sleep deprivation, changes in living conditions, frustration, boredom, loneliness or overstimulation.
- Decisions regarding patient care must be made taking into account the patient's cognitive impairment, living environment, and risk of risky behavior.
- Falls are a problem common to all older people and especially to those with dementia. If possible, medications that induce falls by causing sedation or orthostatic hypotension should be discontinued; change the environment in your place of residence (eg remove slippery rugs, make the bed lower); teach exercises to maintain muscle strength.
- It is important not to lose sight of the risk of becoming a victim of crimes against the elderly and the risk of losing the support of loved ones. Such threats should be taken seriously, especially if reported by the patient.
- Wandering (more common in men) is associated with severe dementia, long-term dementia, depression, delusions, hallucinations, sleep disturbances, and use of antipsychotic medications. To prevent wandering, care must be taken to increase surveillance, change living conditions, and make it more difficult to leave the house. Pharmacotherapy is rarely effective unless wandering is associated with mania. It makes sense to take care of patient identification - a patch on clothing, a bracelet.
Discussing with the patient and family the risks associated with certain activities
- The risks associated with driving should be discussed with people with dementia and their families. The fact of such a discussion should be documented. With patients who continue to drive, this issue should be discussed repeatedly and regularly. This is especially true for patients with Alzheimer's disease and other progressive dementias.
- There is currently no consensus on at what stage of dementia one should stop driving.
- Patients with mild impairments should be advised to limit driving to familiar and safe areas.
- Persons with moderate impairments should stop driving. In severe forms of dementia, a person loses the ability to drive.
- The same approach should be applied to other activities related to the management of complex equipment.
Discussing financial and legal issues with family members
- Discussing certain issues in advance will free the patient's relatives from the difficulties associated with caring for a sick person. The following questions need to be discussed:
- Use of medications, feeding tube, life support system
- Patient participation in research
- Will
- Power of attorney to conduct business
- Treatment cost planning
Patient and family understanding and acceptance of the disease and its associated limitations
- The patient should be offered pragmatic behavioral strategies such as making to-do lists and scheduling.
- In addition to identifying impaired functions, it is necessary to determine what capabilities remain available to the patient.
- Patients who are worried about their diagnosis should be offered psychotherapy.
Treatment of early Alzheimer's disease with donepezil, galantamine or rivastigmine
- These three cholinesterase inhibitors are widely used for cognitive symptoms of early and mid-stage Alzheimer's disease.
- Given the risks of long-term use of vitamin E and selegiline, and the lack of evidence of their effectiveness, their use is not recommended. The effectiveness and safety of non-steroidal anti-inflammatory drugs, statins, and estrogen supplements in the treatment of Alzheimer's disease have not been proven.
- Cholinesterase inhibitors are also recommended for the treatment of mild to moderate dementia due to Parkinson's disease.
- Cholinesterase inhibitors may be used for dementia with Lewy bodies
- Mild cognitive impairment and vascular dementia have vague boundaries with Alzheimer's disease. The safety and effectiveness of cholinesterase inhibitors for these disorders is unclear, so specific recommendations cannot be made at this time, although some patients may benefit from these drugs.
- There is evidence of the effectiveness of memantine in the treatment of mild Alzheimer's disease and very little evidence of its effectiveness in the treatment of vascular dementia.
Diagnosis of depression and treatment
- The best way to identify depression comorbid with dementia has not yet been determined. Irritability and social withdrawal can be added to the DSM-IV-TR criteria.
- Other psychiatric disorders (eg dependence on alcohol or sedative-hypnotics), neurological problems (eg stroke, Parkinson's disease), other diseases (thyroid disease, heart disease, cancer), use of certain drugs (eg corticosteroids, benzodiazepines) can contribute to the development of depression. .
- Depression may exacerbate cognitive impairment in dementia. The goal of treating depression in dementia is to improve cognitive function. Treatment for depression also helps reduce symptoms such as aggression, anxiety, apathy and psychosis.
- It is preferable to use SSRIs, which are best tolerated by patients. Alternatives to SSRIs include venlafaxine, mirtazapine, and bupropion.
- For depression that is life-threatening and unresponsive to other types of treatment, ECT is used.
Diagnosis and treatment of sleep disorders
- Sleep problems occur in 25-30% of people with dementia. The main causes include physiological changes associated with aging, pathological activity of the suprachiasmatic nucleus, the effect of concomitant diseases, the effects of medications, pain, and poor sleep hygiene. Cholinesterase inhibitors may cause insomnia.
- Some drugs (eg diphenhydramine) can promote delirium and paradoxically impair sleep. It is necessary to find out whether the patient is taking such medications or any herbal infusions, and recommend stopping them.
- If sleep disturbance is not associated with other problems, you need to start with non-pharmacological measures, such as training in sleep hygiene, establishing a sleep schedule and bedtime routine, limiting daytime sleep, and adequate physical and mental activity during the day.
- It is necessary to find out what medical problems may underlie sleep disorders. If possible, medications that may interfere with sleep should be adjusted.
- Pharmacological intervention should be initiated only after all other options have failed. It is necessary to identify sleep apnea, which occurs in 33-70% of patients with dementia. This condition is a relative contraindication to the use of benzodiazepines and other respiratory suppressants.
- If drugs with sedative properties are used to treat other behavioral or neuropsychiatric disorders, it is better to take them before bedtime (eg antidepressants with sedative properties, second-generation antipsychotics).
- Pharmacological agents: trazodone or non-benzodiazepine hypnotics (zolpidem or zaleplon). Benzodiazepines can be used, but are recommended only for short-term use due to the development of tolerance, daytime sleepiness, insomnia after discontinuation, cognitive decline, falls, loss of self-control, and delirium. Insomnia and daytime sleepiness can be caused by any drugs in this group. Triazolam is not recommended for dementia due to the risk of amnesia.
Determining the need for patient supervision
- During all patient examinations, attention should be paid to safety issues.
- Family members should be informed of the risks of incidents (eg fire during cooking) and wanderings.
- Family members should be encouraged to take charge of the patient's finances.
- At this stage of the disease, almost all patients should not drive a car.
Discuss options for caregivers and family members (eg discuss transfer of patient to nursing home)
Treatment of cognitive impairment with a combination of a cholinesterase inhibitor and memantine
- This combination has been shown to improve cognitive function and slow the progression of symptoms more effectively than a single cholinesterase inhibitor.
Treatment of psychosis and agitation occurring in patients with moderate disorders
- The pros and cons of treatment should be discussed with the patient and caregivers, and the results of the discussion documented.
- If psychotic symptoms cause minimal discomfort to the patient and are not accompanied by agitation and conflict, it is best to use non-pharmacological methods.
- If symptoms cause significant discomfort and compromise the safety of the patient and others, the use of low-dose antipsychotics in addition to nonpharmacological methods is indicated. For agitation and conflict without psychosis, antipsychotics are also indicated. However, the benefits of antipsychotic treatment must be weighed against the potential increased risk of death in patients with dementia taking antipsychotics.
- When antipsychotics do not work, carbamazepine, valproic acid, or SSRIs may be used with caution. If behavioral abnormalities occur only at certain times or in certain circumstances (eg during diagnostic testing), or when other methods have not worked, low-dose benzodiazepines can be used, although side effects may be a problem in the elderly. Mood stabilizers and SSRIs are used for agitation, delirium, and aggressiveness, but their effectiveness and safety for these symptoms have not been proven. Therefore, when choosing a medication, you should not consider mood stabilizers and SSRIs to be safer or as effective as antipsychotics.
- As dementia progresses, psychosis and agitation may lessen or change. Therefore, long-term treatment of behavioral disorders or psychoses must be adjusted during treatment.
Identifying and treating depression and sleep disorders using the strategies described
Memantine or cholinesterase inhibitor for the treatment of cognitive impairment
- Memantine is FDA approved for the treatment of moderate to severe Alzheimer's disease. It helps achieve some success with few side effects.
- Donepezil is FDA approved for the treatment of severe Alzheimer's disease. The use of galantamine and rivastigmine in advanced disease is not approved but may be beneficial.
- To understand whether medications are working, you can stop them for a while and evaluate the patient's condition.
Assessment and treatment of other psychiatric symptoms
- Depression is less common and more difficult to diagnose, but if it exists, it must be actively treated.
- Psychotic symptoms and agitation are often present and if they cause discomfort to the patient or pose a threat to the safety of caregivers or other residents of the nursing home, pharmacological treatment is necessary.
- Sleep disorders should be treated as described above.
Providing adequate care, including prevention of pressure ulcers and contractures
Helping the family prepare for the patient's death
- Ideally, discussions about feeding tubes, infection management, cardiopulmonary resuscitation, and intubation should occur when the patient can participate. If it was not possible to discuss these issues in advance, you need to discuss them with family members before an urgent need arises.
Psychosocial activities to correct behavior and improve mood
- Behavior-focused interventions are needed to identify the causes and consequences of problem behavior and to change the external conditions affecting the patient.
- Activities aimed at stimulation, such as active leisure, art therapy, music therapy, pet therapy, etc. are aimed at maximizing the feeling of satisfaction in patients, resulting in improved behavior, mood and, to a lesser extent, functional possibilities.
- Among the interventions that target emotions, supportive psychotherapy is recommended that targets the feelings of loss that arise in the early stages of dementia.
- Cognitive-oriented activities, such as reality orientation, retraining, and skills training aimed at replenishing cognitive deficits, are unlikely to produce a lasting positive effect and, moreover, cause a state of frustration in some patients.
Organizing these events simultaneously, daily or weekly
- Since the effect of psychosocial interventions usually does not last long, they are recommended to be carried out regularly.
Unless absolutely necessary, start with non-pharmacological methods, avoiding polypharmacy if possible
Initial doses should be low, dose increases should be slow, and intervals between medications should be long.
- In the elderly, renal clearance is reduced and hepatic metabolism is slowed, which alters the pharmacokinetics of many drugs. In addition, older adults may be taking many medications for different illnesses, so it is important to consider how illnesses and medications may affect drug absorption, plasma protein binding, metabolism, and elimination.
- Some patients may require higher doses given to younger patients.
CHOLINESTERASE INHIBITORS AND MEMANTINE
| Medicine | Initial dose (mg/day) | Target dose (mg/day) | Side effects |
| Donepezil | 5 | 10 | Cholinergic effects including nausea, vomiting, decreased appetite and weight, bradycardia, muscle cramps, increased acidity. May cause or worsen urinary tract obstruction, worsen asthma and COPD, cause seizures, cause or worsen sleep disturbances, and enhance the effects of certain relaxants during anesthesia. |
| Galantamine | 8 | 16-24 | |
| Rivastigmine | 3 | 6-12 | |
| Memantine | 5 | 20 | Rare: mild confusion, dizziness, headache, sedation, agitation, falls, constipation. |
SECOND GENERATION ANTIPSYCHOTICS
| Medicine | Initial dose (mg/day) | Maximum dose (mg/day) | Side effects |
| Aripiprazole | Unknowna | 15 | Mild to moderate side effects include akathisia, parkinsonism, sedation, peripheral and central anticholinergic effects, delirium, postural hypotension, cardiac conduction disturbances, urinary tract infections, urinary tract obstruction, and falls. Serious side effects include tardive dyskinesia, neuroleptic malignant syndrome, hyperlipidemia, weight gain, diabetes, stroke, and death. |
| Olanzapine | 1,25-5 | 10 | |
| Quetiapine | 12,5-50 | 200-300 | |
| Risperidone | 0,25-1 | 1,5-2 | |
| Ziprasidone | Unknown | Unknown |
a The data collected suggest that 5 mg/day is a safe dose for most patients.
ANTIDEPRESSANTS
| Medicine | Initial dose (mg/day) | Maximum dose (mg/day) | Side effects |
| Citalopram | 5-10 | 40 | Nausea and vomiting, agitation and akathisia, sexual dysfunction, weight loss, hyponatremia, increased risk of falls. |
| Bupropion | 45 | 135 | |
| Duloxetine | 20-40 | 60-80 | |
| Escitalopram | 5 | 20 | |
| Mirtazapine | 7,5 | 45-60 | |
| Paroxetine | 5-10 | 40 | |
| Sertraline | 12,5-25 | 150-200 | |
| Venlafaxine | 25 | 375 | |
| Venlafaxine extended release | 37,5 | 225 |
MEDICINES FOR TREATING SLEEP DISORDERS
| Medicine | Usual dose (mg) | Side effects |
| Trazodone | 25-100 | Postural hypotension, which may lead to falls |
| Non-benzodiazepine hypnotics | ||
| Zolpidem | 5-10 | Daytime sleepiness |
| Zaleplon | 5-10 | Daytime sleepiness |
Side effects of medications may cause problems in older patients with dementia
- Anticholinergic effects (eg antipsychotics, antidepressants, diphenhydramine) are problematic in people with dementia and may aggravate existing cardiovascular, prostate, bladder, or other conditions. Anticholinergic drugs can also worsen cognitive impairment, confusion, and even delirium.
- Elderly patients, especially those with dementia, are prone to falls and fall-related injuries.
- Drugs that cause sedation (eg benzodiazepines) may impair cognitive function and increase the risk of falls and respiratory depression in patients with sleep apnea.
- Antipsychotic use is associated with cognitive decline, excessive sedation, falls, tardive dyskinesia, neuroleptic malignant syndrome, as well as hyperlipidemia, weight gain, diabetes, stroke, and death. The elderly, particularly those with Parkinson's disease or Lewy body dementia, are particularly sensitive to extrapyramidal side effects.
Care must meet the needs of patients, including those with behavioral problems
- Staff should have knowledge and experience of working with people with dementia whose behavior is challenging.
Adequate use of medications alleviates psychiatric symptoms, reduces discomfort, and enhances the safety of patients and medical staff.
- It is important to consider the risk of side effects, periodically evaluate the need for antipsychotics and the possibility of using alternatives, and document decisions made.
- Provider education helps manage patient behavior and reduce the use of antipsychotics.
Physical restraint is rarely indicated and should only be used if the patient threatens his or her own safety or the safety of others.
- The reasons for using physical restraint should be documented.
- The need for physical restraint may be reduced by changing living conditions, reducing the risk of falls and wandering, and identifying and eliminating the causes of agitation.
Author of the translation: Filippov D.S.
Editor: Kasyanov E.D.
Source
The art of substitution
— How justified are the advances that the FDA gave to the manufacturer of this drug?
“Many scientists have expressed doubts that a slight reduction in such plaques improves the condition of patients. And the adukunamab trials actually confirmed this. Even earlier, several drugs in development also slightly reduced the amount of amyloid plaques, but did not improve the cognitive (mental) abilities of patients. Researchers led by Maria Glymour of the University of California, San Francisco, conducted an analysis that found no link between cognitive performance and the small reduction in amyloid in these studies: "The idea that we would approve drugs based on a change in a biomarker of amyloid reduction when we know “That reducing the amount of amyloid does not mean a definite benefit for improving people’s quality of life, that is, improving memory and well-being in general, sets a bad precedent.”
Jörg Schulz, head of the department of neurology at the Medical School of the RWTH University in Aachen (Germany) , asked whether a number of those drugs (which were not previously approved, and there were many) that also reduce amyloid will now be re-evaluated. under the same expedited procedure. Acting FDA Commissioner Janet Woodcock said affirmatively: “The door is open for expedited approval of other beta-amyloid-lowering drugs based on biomarker data alone.”
No more sentence. How to cope with Parkinson's and Alzheimer's diseases Read more