Hemorrhagic stroke - what is it? Symptoms, treatment and prognosis
Hemorrhagic stroke, acute cerebrovascular accident (ACVA) of the hemorrhagic type is an acute clinical syndrome that is a consequence of damage to cerebral vessels and hemorrhage in the brain. The root cause may be damage to either an artery or a vein. The larger the damaged vessel, the more profuse the bleeding; in severe cases, up to 100 ml of blood is poured into the tissue. The resulting hematoma mechanically compresses and displaces the nervous tissue, and swelling quickly develops in the affected area.
If the victim is not provided with medical assistance within three hours, the chances of survival rapidly decrease and tend to zero. According to statistics, hemorrhagic strokes account for just over 20% of stroke cases.
What it is?
Hemorrhagic stroke is an acute hemorrhage in the brain due to rupture or increased permeability of blood vessels. This cerebrovascular accident differs from classic (ischemic) stroke, which is more common (70% of patients).
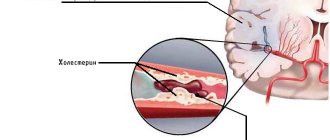
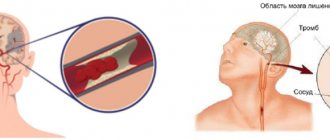
The nature of changes in blood vessels during an ischemic stroke is the blockage of their lumen by blood clots, resulting in gradual necrosis of brain cells, and in a hemorrhagic stroke there is a violation of the integrity of the vascular wall, as a result of which the brain tissue is saturated and compressed by the gushing blood.
Hemorrhagic cerebral stroke is a dangerous and insidious disease. It is characterized by:
- High mortality (60–70% of patients die within the first week after the onset of the disease).
- Suddenness (in 60–65% of patients, hemorrhage occurs without any previous symptoms).
- Profound disability of surviving patients - 70–80% of people are bedridden and cannot care for themselves, the remaining 20–30% have a less pronounced neurological deficit (the function of the limbs, walking, speech, vision, intelligence, etc. is impaired)
More than 80% of brain hemorrhages are associated with increased blood pressure (hypertension). By taking antihypertensive drugs (blood-lowering drugs), you can reduce the risk of stroke, the amount of hemorrhage and the severity of brain damage. If patients are admitted to a medical facility within the first 3 hours, this increases the chances of survival. Specialized rehabilitation centers help restore lost brain functions as much as possible after a stroke. Complete cure is rare, but possible.
Prevention
The disease is extremely serious and dangerous. It is much easier to avoid it than to treat it later. Prevention measures include:
Blood pressure control
- proper nutrition;
- monitoring weight changes (especially when you are overweight);
- control of blood pressure, preventing its increase;
- fight against atherosclerotic phenomena;
- getting rid of bad habits - smoking, alcohol;
- If possible, avoid stress and overexertion.
To prevent relapse, restorative and vitamin preparations are prescribed. Constant supervision by a specialist is required.
Classification
It should be noted that a brainstem stroke results in almost instantaneous death. Only in rare cases is it possible to save the patient’s life with such a diagnosis. At the same time, there is no likelihood of returning to a full life.
The brain stem is the center of all body systems and is directly connected to the spinal cord. It serves as a link between the commands of the brain centers and the nerves of the body: it is thanks to it that we are able to move, breathe, swallow, see, hear, and so on. The brain stem also regulates the circulatory system, thermoregulation, and heartbeat. That is why damage to it during a stroke most often leads to death.
Based on their origin, primary and secondary hemorrhagic stroke are distinguished:
| Primary | provoked by a hypertensive crisis or thinning of the walls of arteries and veins due to prolonged stress on them (for example, due to high blood pressure, physical and nervous overload, etc.) |
| Secondary | provoked by the rupture of an aneurysm, hemangioma and other vascular deformations and anomalies (malformations), congenital or formed in the process of life. |
Depending on the localization zone, I distinguish the following types of hemorrhagic stroke:
- Subarachnoid - hemorrhage into the space between the hard, soft and arachnoid membranes of the brain;
- Hemorrhage on the periphery of the brain or in the thickness of its tissue;
- Venticular hemorrhage - localized in the lateral ventricles;
- Combined type: occurs with extensive hemorrhage affecting several areas of the brain.
Peripheral hemorrhage is much less dangerous than intracerebral hemorrhage, which inevitably provokes the formation of hematomas, edema and subsequent death of brain tissue. Hematomas are also distinguished by location:
- Lobar - the hematoma is localized within one lobe of the brain, without going beyond the cerebral cortex.
- Medial - hemorrhage damages the thalamus.
- Lateral – damage to the subcortical nuclei localized in the white matter of the hemispheres (fence, amygdala, caudate, lenticular nuclei).
- Mixed - hematomas affecting several areas of the brain at once are most common.
Meningeal symptoms
Signs of irritation of the meninges can occur with parenchymal hemorrhage due to cerebral edema, but they are more characteristic of subarachnoid hemorrhage.
The most typical sign is a stiff neck, when the patient is unable to press the chin to the chest when lying down.
If the patient bends his knees while checking for rigidity, this is another sign of irritation of the meninges, which is called Brudzinski's sign.
Clinical manifestations
Symptoms of hemorrhagic stroke are varied and are divided into two large groups: general cerebral and focal. Also, the symptoms strongly depend on the location of the hemorrhage, its size, the somatic condition of the patient and many other factors.
General cerebral symptoms of hemorrhagic stroke include the following:
- Impaired consciousness (stunning, stupor, coma). The larger the focus, the lower the level of consciousness. However, with damage to the brain stem, even a small focus of hemorrhage leads to severe depression of consciousness.
- Dizziness.
- Nausea, vomiting.
- Headache.
- General weakness.
- Breathing disorders.
- Hemodynamic disorders.
Predominantly focal symptoms include the following:
- Paresis or plegia in the limbs, hemiparesis is more common.
- Paresis of facial muscles.
- Speech disorders develop mainly with damage to the left temporal lobe.
- Visual impairment (including the development of anisocoria).
- Hearing impairment.
A stroke should be suspected if the patient has any type of speech impairment, weakness in the arm and leg on one side, the development of epileptic seizures without provoking factors (for example, such factors include alcohol consumption), impaired consciousness up to coma. In any suspicious cases, it is better to play it safe and call an ambulance. Behavior and assessment of the situation when a stroke is suspected should be considered in a separate article.
Coma due to hemorrhagic stroke
Approximately 90% of patients with GI in a state of stupor or coma die in the first five days, despite intensive therapy. Disorders of consciousness are characteristic of many pathologies, manifested by inhibition of the functions of the reticular formation of the brain.
Brain dysfunctions develop under the influence of:
- Endo- and exotoxins – derivatives of the end products of metabolism;
- Oxygen and energy starvation of the brain;
- Metabolic disorders in brain structures;
- Expansion of the volume of brain matter.
The most important factors in the development of coma are acidosis, cerebral edema, increased intracranial pressure, and impaired microcirculation of brain fluids and blood.
The state of coma affects the functioning of the respiratory system, excretion (kidneys) and digestion (liver, intestines). It is impossible to recover from a coma at home, and it is very difficult even in intensive care conditions.
The clinical definition of coma is carried out using the GCS (Glasgow Coma Scale), and some other methods that are important for clinicians are used. There are precoma and four stages of coma. The easiest is the first, and the hopeless state of the patient corresponds to the fourth stage of coma.
Treatment
Stroke therapy in the acute period may include:
- Pain relief, correction of body temperature (paracetamol, efferalgan, naproxen, diclofenac, often opiates, propafol). Aspizol, dantrolene are given intravenously, and magnesium sulfate is given by drip.
- Reducing blood pressure, which helps stop bleeding in the brain. For this purpose, drugs are administered intravenously: labetalol, nicardipine, esmolol, hydralazine. However, a sharp decrease in pressure in the first days is not allowed. Next, tablet drugs are prescribed - captopril, enalapril, capoten (as basic therapy orally or through a tube).
- Diuretics for persistent high blood pressure (chlorothiazide, andapamide, Lasix), calcium antagonists (nimotop, nifedipine).
- In case of severe hypotension, vasopressors are prescribed by drip (norepinephrine, mesaton, dopamine).
- Often, a continuous intravenous infusion is used to administer the above drugs, monitoring the pressure level every 15 minutes.
- To reduce cerebral edema, dexamethasone is recommended for 3 days (intravenously). If the swelling progresses, glycerin, mannitol, albumin, and refortan are injected dripwise.
- Often, a continuous intravenous infusion is used to administer the above drugs, monitoring the pressure level every 15 minutes.
- Drugs for the correction of neurological symptoms (sedatives - diazepam, muscle relaxants - vecuronium).
- Local therapy is aimed at eliminating bedsores and includes treating the skin with camphor alcohol and sprinkling with talcum powder.
- Symptomatic therapy - anticonvulsants (lorazepam, thiopental or anesthesia for 1-2 hours), medications for vomiting and nausea (metoclopramide, torecan), against psychomotor agitation (haloperidol). For pneumonia and urological infections, a course of antibacterial treatment is carried out.
In the presence of large hematomas (more than 50 ml), surgical intervention is performed. Excision of the hemorrhage site can be carried out if it is localized in an accessible part of the brain, and also if the patient is not in a comatose state. Most often, clipping of the aneurysm neck, puncture-aspiration elimination of the hematoma, its direct removal, as well as ventricular drainage are used.
Medical care in hospital
All patients receive intensive therapeutic care at an early stage in a neuro intensive care hospital. Initial treatment measures are aimed at:
- normalization of microcirculation, hemorheological disorders;
- relief of cerebral edema, treatment of obstructive hydrocephalus;
- correction of blood pressure, body temperature;
- functional regulation of the cardiovascular system;
- maintaining water and electrolyte balance;
- prevention of possible seizures;
- prevention of extracranial consequences of inflammatory and trophic nature (pneumonia, embolism, pulmonary edema, pyelonephritis, cachexia, DIC syndrome, endocarditis, bedsores, muscle atrophy, etc.);
- providing respiratory support (if the patient needs it);
- elimination of intracranial hypertension in HI with dislocation.
Consequences
If patients can be saved, they experience neurological deficits—symptoms caused by damage to the area of the brain where the hemorrhage occurred.
These may be consequences of a hemorrhagic stroke:
- paresis and paralysis - impaired movement of the limbs on one half of the body, since they are constantly in a half-bent position and it is impossible to straighten them;
- speech impairment and its complete absence;
- mental disorders and irritability;
- constant headaches;
- movement coordination disorders;
- inability to walk or even sit independently;
- visual impairment up to complete blindness;
- facial distortion;
- vegetative state - the absence of any signs of brain activity (consciousness, memory, speech, movements) with preserved breathing and heartbeat.
Symptoms of the disease and their duration depend on the location of the hemorrhage and its volume. The first 3 days are the most dangerous, since during this time severe disorders occur in the brain. Most deaths (80–90%) occur during this period. The remaining 10–20% of patients die within one to two weeks. Patients who survive recover gradually from a few weeks to 9–10 months.
Rehabilitation objectives
The main objectives of the ongoing rehabilitation are:
- Work on restoring lost everyday and physiological functions of a person suffering from a stroke. Restoring full range of motion, the ability to independently care for oneself and perform simple household chores.
- Restoration of lost professional ability to work with a return to the previous place of activity or assistance in retraining.
- Maintaining the necessary social activity of a person, first of all, restoring his contact with loved ones and the ability to make new acquaintances;
It is very important to prevent a possible relapse and correct the patient’s current lifestyle.
Left-hand side
If the left side is affected, the consequences are characterized by disruption of the right side of the body. The patient experiences complete or partial paralysis, and not only the leg and arm are affected, but also half of the tongue and larynx. Such patients develop gait disturbances and a characteristic posture of the right hand (folded in a boat).
The victim experiences deterioration in memory and speech, and the ability to clearly express thoughts is impaired. Damage to the left hemisphere of the brain is characterized by problems with recognizing time sequences; it cannot decompose complex elements into components. Impairments in written and oral speech appear.
Right side
If the right side is affected, the most dangerous consequence is damage to the brain stem, in which a person's chances of survival are close to zero. This department is responsible for the functioning of the heart and respiratory system.
Diagnosing a hemorrhagic stroke on the right is quite difficult, since the centers of orientation in space and sensitivity are located in this part. This lesion is determined by speech impairment in right-handed people (in left-handed people the speech center is located in the left hemisphere). In addition, there is a clear relationship: if the functionality of the right half of the brain is impaired, the left side suffers and vice versa.
Lifestyle
Stroke is a disease in which a person must start life in new conditions. Most people find it difficult to accept their condition, so deep depression is as dangerous a complication as the physical manifestations. Already in the first stages of recovery, much attention is paid to this aspect.
The scientific, material and technical base of the Yusupov Hospital allows patients to undergo rehabilitation procedures using modern equipment that meets European standards.
How long do they live after a hemorrhagic stroke?
The prognosis of hemorrhagic stroke is unfavorable. It depends on the location and extent of the lesion. Hemorrhage into the brainstem is dangerous, which is accompanied by respiratory failure and a sharp, poorly corrected by drugs, decrease in blood pressure to critical levels. Hemorrhage into the ventricles with their breakthrough is severe and often ends in death.
How long do people live with hemorrhagic stroke? This pathology is fatal in 50-90% of cases. Death may occur on the very first day - against the background of generalized convulsions, when breathing is impaired. More often, death occurs later, by 2 weeks. This is due to a cascade of biochemical reactions triggered by the outpouring of blood into the cranial cavity and leading to the death of brain cells. If there is no displacement of the brain, no herniation (entry into a bone hole), no breakthrough of blood into the ventricles, and the compensatory capabilities of the brain are sufficiently large (this is more typical for children and young people), then the person has a great chance of survival.
At 1-2 weeks, in addition to neurological disorders, complications associated with the immobility of the patient, exacerbation of his chronic diseases or connecting him to an artificial respiration apparatus (pneumonia, bedsores, liver, kidney, cardiovascular failure) occur. And if they do not lead to death, then by the end of 2-3 weeks the cerebral edema will stop. By week 3, it becomes clear what the consequences of a hemorrhagic stroke are in this case.
Principles of disease diagnosis
The gold standard for making a diagnosis is computed tomography (CT). In the early period after an attack (1-3 days), this method of neuroimaging is more informative than MRI. Fresh hemorrhagic material, including 98% hemoglobin, appears on CT as a high-density, well-defined, bright inclusion against the background of darker brain tissue. Based on a computed tomogram, the epicenter zone, volume and shape of the formation, the level of damage to the internal capsule, the degree of dislocation of brain structures, and the state of the cerebrospinal fluid system are determined.
With the onset of the subacute phase (after 3 days), the red cells of the hematoma along the periphery are destroyed, in the center the iron-containing protein is oxidized, and the focus becomes lower in density. Therefore, along with CT scan, MRI is mandatory within 3 days and later. In subacute and chronic forms, the MR signal, in contrast to CT, better visualizes a hematoma with derivatives of hemoglobin oxidation (methemoglobin), which passes into the isodense stage. Angiographic examination methods are used in patients with an unknown cause of hemorrhagic stroke. Angiography is primarily performed on young people with normal blood pressure readings.
For adequate management of patients after an attack of intracerebral hemorrhage, an ECG and X-ray of the respiratory organs are required, and tests for electrolytes, PTT and APTT are taken.
Recovery after a stroke
The rehabilitation period after a hemorrhagic stroke is long, especially in old age. It depends on the lost functions and does not guarantee their complete rehabilitation. Lost abilities are restored most quickly in the first year after a stroke, then this process is slower. The neurological deficit that remains after three years will most likely remain for life.
Neurologists and rehabilitation specialists are ready to help restore lost functions as much as possible. For this:
- classes are held with a psychologist or psychotherapist;
- if reading/writing skills are lost, classes are held to restore them;
- hydrotherapy is carried out (massage in the pool, light exercises in the water);
- classes on special simulators;
- if speech reproduction is impaired, the person will have to work with a speech therapist; for paresis or paralysis, physiotherapy is carried out (for example, on the Myoton apparatus), massage and exercise therapy are performed with an instructor;
- drugs are prescribed that will help restore lost neural connections (“Cerakson”, “Somazina”), reduce high blood pressure (“Enalapril”, “Nifedipine”), antidepressants and sedatives;
- color therapy - treatment with visual images.
The prognosis for recovery depends on how large the area was covered by the hemorrhage, as well as on how qualified the actions of doctors and rehabilitation specialists were. Hemorrhagic stroke is a very complex pathology, the consequences of which are unlikely to be completely eliminated. Maintenance treatment and rehabilitation continue for a very long time.
Fighting bedsores
Bedsores are a dangerous enemy of bedridden patients who have to remain in bed for long periods of time. Bedsores appear in areas that are subject to the greatest pressure - the tailbone, shoulder blades, buttocks, legs, forearms.
Bedsores in advanced stages require surgical treatment. There are cases when a patient was saved in intensive care, but then, due to poor care, he died from sepsis that developed from banal bedsores. Nursing after a stroke is exactly the case when an experienced and conscientious nurse is just as important as a doctor. And sometimes it’s even more important.