As part of a series of articles based on materials from the source “Psychoanalytic Diagnostics” by Nancy McWilliams, we will turn to the manic personality type. The article is addressed to all those who are interested in psychology, as well as those who visit or plan to see a psychologist for professional help.
In this article we will look at the main characteristics and features of the manic personality type; what contributes to its formation; and how manic individuals interact with other people.
Characteristics of manic personalities
In psychology, it is believed that mania is the other side of depression. If we talk about depression, it is neutralized by the defense mechanism of denial. In the external world for a person there are, or he perceives, circumstances that he does not want or cannot recognize as existing. We can say that mania is the polar opposite of the depressive personality type.
A manic personality is cheerful, active, feels guilty due to aggression towards others, and cannot be lonely. They often have grandiose plans. These people can be creative, bursting with many ideas and projects.
From the outside it seems that they are on top and cannot slow down. Some may use alcohol or any psychotropic drugs to relax. When communicating with them, people note their unabating wit, I can admire them.
Spectrum of disorders
Symptoms of mania can vary in intensity:
- hypomania – mild form; the disorder does not cause significant harm to a person's psychosocial functioning and is characterized by moderately elevated mood that persists for at least 4 consecutive days, increased energy, activity, and a feeling of increased productivity;
- classic mania – elevated mood and agitation lasting more than a week, increased self-esteem, loss of social inhibitions, risky behavior;
- manic disorder with psychotic symptoms often requires hospitalization, the disease is characterized by the presence of delusions and hallucinations; this form affects about 1/3 of patients (manias, usually expansive, religious, erotic, etc.).
Manic syndrome is divided into 3 types:
- euphoric syndrome - a feeling of bliss, contentment without significant hyperactivity;
- stuporous mania – complete absence of psychomotor symptoms;
- resonant mania - irritability, anxiety, sometimes aggression.
Drives, affects
Manic individuals have high arousal and sociability. We can say that they are, as a rule, the “life of the party.” With the help of humor they do not enter into close relationships with others. It looks like they are laughing it off and not talking seriously about something.
In manic individuals, there is a sudden manifestation of hatred. These may be similar to affective reactions.
If we consider the communicative process of manic personalities, then there is an oral non-stop process, they talk a lot, and can attract attention to themselves.
The constant mobility of individuals with manic character characteristics indicates high anxiety, while calm serenity is beyond their experience. This does not mean that they consciously drive themselves into stressful states; they are simply habitual for a manic personality type.
Diagnostic criteria
The diagnosis is made based on the medical history and interview with the patient. The exact type of mania is determined and appropriate treatment is decided. If necessary, tests are carried out to determine what type of mania the patient has developed.
Rorschach test
The Rorschach test (inkblot test) is one of the psychological methods used to analyze personality. This is a projective test that uses the projection of thinking processes and personal qualities onto undefined objects.
Altman scale
The Altman Scale is a self-report diagnostic scale that can be used to assess the presence and severity of manic and hypomanic symptoms, most commonly in patients suspected of having bipolar disorder.
This scale can assess differences in “normal” or baseline levels from mania in 5 subjective and behavioral areas:
- positive mood;
- self confidence;
- need for sleep;
- speech;
- activity.
Defense mechanisms and adaptation
The leading mechanisms of psychological defense in a manic personality type are denial and reaction.
Denial - ignoring, or turning into humor. This may be due to the fact that the situations in which these people find themselves can be emotionally difficult for them.
Ignoring – sexualization, intoxication, theft, etc. Prone to depreciation. This happens automatically. Bringing these processes to the level of awareness is one of the leading tasks of a psychologist when working with manic individuals.
Such clients prefer everything that distracts them from emotional suffering. It is also important to note omnipotent control. And, for the most part, authoritarian. Trying to control everything around them reduces their anxiety level.
Manic individuals are usually convinced of the success of their own plans.
You can often notice quite a lot of criticism towards other people.
The manic personality type is characterized by the presence of emotional violence and neglect towards other people.
Diagnostics
The clinical picture plays a major role in making a diagnosis. Symptoms can only be assessed by a psychiatrist after a comprehensive life history collection. Laboratory and instrumental studies are of little significance. The criteria for bipolar disorder must correspond to those specified in the International Classification of Diseases (ICD-10), which are used in the protocols for providing assistance to the Russian Federation.
Mental status is examined not only at the time of examination, but throughout the entire history of the disease. The patient’s complaints, symptoms observed from others (by others), and the age of first manifestations are taken into account. Relatives must honestly talk about the peculiarities of raising children, the presence of hereditary burden of (any) mental illnesses, including through generations.
An important diagnostic point is assessing the risk of suicide. The most commonly used is the Columbia scale. Self-harmful behavior and preparatory actions are also included in the criteria for severe MDP.
Manic self
The “I” of manic personalities is like a children’s toy top. Such a high speed makes it possible not to come into contact with painful experiences or conditions.
They are at risk of experiencing disintegration of their own “I”, that is, they are “afraid of falling apart.”
In a manic personality type, avoidance of pain occurs in exchange for the light of high spirits. As a rule, they are extraordinary and witty.
If we talk about extreme manifestations of character, bordering on borderline, then suicidal intentions are possible.
Application of the diagnosis "mania"
One of the leading tasks of a psychologist when working with a manic personality type is early and unjustified prevention of interruption of sessions. It can be quite difficult for these clients to hold on to their experiences that occur during the setting. They feel the impulse to run away.
You can say to such a client: “I noticed that many important life situations were interrupted on your initiative. This is also possible in a session. Pay attention to this!” If you do not follow the impulse, but try to explore it, especially in terms of when and how it arises, then you can control it.
During a psychological session, a confrontation occurs with the usual way of ending a relationship. This is done in the mode of experimentation and the client’s awareness of his reactions.
If there is an intolerance to something, it is important to explore this in a safe environment in a psychological session. Such clients often complain of frequent allergies.
During sessions, working through one's own unmourned losses often comes up. If you constantly avoid these experiences, they will “fade out”, appearing in other situations similar to the traumatic one.
It is important to teach the client to love. First of all, yourself. To get closer to another person, you must be aware of any reactions you have. In particular, note the negative. Emphasize the affects that lead to clarification. For example, you can return his message to the client by pointing out the feelings that arose here and now in the psychological session.
Demonstrating how to live in the world of feelings is very important for these clients. This is a development zone for them, and we can say that this is an unknown world. They tend to prefer to talk instead of feel.
How to recognize a maniac by his behavior?
Often in films, maniacs are shown as exemplary and law-abiding citizens who literally turn into werewolves when darkness falls. And this is not the directors’ imagination. Most people with these disorders do not show their aggression in everyday life. They are well-mannered, calm, reasonable and taciturn. They usually dress modestly so as not to stand out from the crowd. They may seem boring and pedantic. Many women consider such men to be ideal family men, so they easily meet them halfway.
By the way, have you noticed that among the maniacs there are practically no representatives of the fairer sex? Female aggression can be no less terrible, but usually women splash out their emotions immediately, and do not accumulate them, like men.
If you dare to go to the cinema with a stranger, watch the expression on his face while watching the film. If horror and violence are shown on the screen, and your friend calmly watches it, you should be wary. Of course, men will not cry or hide behind your shoulder so as not to show weakness. They may demonstrate feigned courage, but you can still read certain emotions on their faces. No one will enjoy watching people kill each other, even on screen. But the maniac will not only not be hurt by such a picture, he will watch it calmly and even with some admiration. Keep this in mind to recognize a maniac in the early stages of dating.
It is also worth paying attention to how the other person looks at you when you express strong emotions. Usually the maniac does not look away, but looks intently at the person, even if he is screaming or crying. Not a muscle moves on his face. It seems that this is a wax statue, and not a living person.
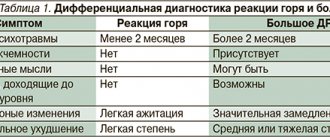
Differential diagnosis
Manic vs. Hysterical: Both tend to be charming and can attract attention. The hysterical personality feels insufficiently supported. Manic can lead to devaluation of the psychologist. There is no preoccupation with gender, unlike the hysterical one. A psychologist, especially in the Gestalt approach, focuses on working with feelings, which can be a rather painful process.
Manic versus Narcissistic Personality: Both types exhibit grandiosity. Narcissists do not have intense worries like manic individuals. Denial, as a psychological defense mechanism of the individual, is mainly present in the manic. Narcissists, in most cases, are not inclined to end relationships with other people.
Manic versus Compulsive Personality: Both types are ambitious and demanding of themselves and others. Compulsive individuals are capable of deep relationships, long-term intimacy, and are modest. And manic people are pompous and incapable of getting close to others. And compulsive people are more moral. Manic individuals ridicule authorities and can be immoral.
Next in the series of articles we will look at the schizoid personality type.
Therapy methods
In the treatment of manic syndrome, 2 main groups of medications are used: mood stabilizers and antipsychotics.
The patient may also be prescribed medications that have auxiliary effects, for example, for insomnia, anxiety and restlessness, etc.
The main drugs used in therapy:
- Mood stabilizers : a group of drugs intended for preventive treatment. Their long-term use reduces the risk of relapse of depression or mania. Drugs in this group are also used in acute cases of mania or depression.
- Antipsychotics (antipsychotics) : drugs used to treat mania or depression. Some of the newer antipsychotic drugs have also demonstrated effectiveness in long-term, prophylactic use, thus resembling the effects of mood stabilizers.
Additional (auxiliary) drugs:
- Antidepressants are used to treat depression. It is not recommended to use drugs in this group without a mood stabilizer - this can lead to a worsening of the disease.
- Sleeping pills and tranquilizers are intended only for short-term use in the treatment of insomnia, anxiety, in cases of tension or excitement.