Infectious disease specialist
Sinitsyn
Olga Valentinovna
33 years of experience
Highest qualification category of infectious disease doctor
Make an appointment
HIV (human immunodeficiency virus) is a virus that attacks the body's immune system. More precisely, it targets certain immune cells and kills them. The longer and more active this process lasts, the weaker the immune system becomes - over time, it is simply unable to cope even with infections that are relatively safe for an ordinary person.
HIV and AIDS - differences, duration of development, forecasts
AIDS is the final stage of HIV, which is characterized by severely reduced immunity. It is important not to confuse these two concepts. From the moment of HIV infection, the disease can develop to the AIDS stage without treatment within 9-11 years (on average). Once diagnosed with AIDS without treatment, life expectancy is short - on average up to 19 months.
If you start treatment on time, you can live a very long life at the HIV stage - the life expectancy of such patients thanks to modern treatment is 20-50 years. And although at the AIDS stage the situation is much more complicated, many patients, with proper treatment and a strong body, can live more than 10 years.
It is obvious that taking therapy is the most important factor for treating HIV and living a full, long life. Moreover, it is treatment that can significantly reduce the viral load and make the infected person harmless to the partner, as well as family members.
Diagnosis of human immunodeficiency virus
It is important for any person to know what HIV tests are available in clinics. To detect infection, an enzyme-linked immunosorbent assay is performed to detect antibodies to HIV in biological fluids. A positive result can only be after the end of the incubation period, when the body has already synthesized antibodies to the virus. The test is done no earlier than 4 weeks after contact, the results will be reliable after 3-4 months, control tests are taken after 6 and 12 months.
If the ELISA is positive, the blood sample is retested by immunoblotting. If this test gives a positive answer, the probability of HIV reaches 99.9%. If the immunoblot test is negative, there is no virus in the blood. An indeterminate test result is possible during the incubation period, when there are still few viral particles, or after treatment of the infection.
If HIV is detected, the patient is given tests to measure the amount of viruses in the blood plasma (the so-called viral load) and the patient's immune status is determined.
Routes of HIV transmission
Main routes of HIV infection:
- unprotected sex with an infected person (the most common route of HIV transmission). You can become infected either after a single contact or after several;
- using a needle to inject drugs after an infected person. Or other variants of situations in which the blood of a healthy person comes into contact with the blood of an infected person;
- transmission from mother to fetus during childbirth or from mother to child during breastfeeding. An important note: if a woman is treated and is under the supervision of doctors, she has every chance of giving birth to a healthy baby;
- transfusion of infected blood. In modern clinics and hospitals this is no longer possible, since all materials undergo very serious testing.
There are also so-called risk groups - these are people who are more susceptible to HIV infection than others:
- people who are promiscuous;
- homosexuals;
- drug addicts who inject drugs;
- people with a partner infected with the virus.
Such people should constantly get tested. In some cases, they are recommended to take preventive medications (only on the recommendation of a doctor).
When talking about how you can become infected with HIV, you should clarify in what cases this is impossible:
- during everyday contacts;
- when using infected utensils;
- with an insect bite;
- when kissing.
Contact with an HIV-infected person at the everyday level (in the family, at work, in other forms of communication) is absolutely safe and does not pose any threat to others.
Main stages of the disease
The stages of HIV are divided into the following:
- incubation This is the stage at which infection and subsequent multiplication of the virus in the blood occurs. It lasts up to six weeks, sometimes less. Even if infected, at this stage a person will not see obvious signs, and a blood test will not show that there are antibodies in the blood;
- primary. The first signs of infection may already appear here. The second stage lasts for 3 weeks - at this time antibodies appear, the virus is determined in the laboratory;
- subclinical. The first sign of the disease appears - enlarged lymph nodes. The patient feels completely healthy and does not complain about his health;
- the appearance of secondary diseases. The immune system begins to malfunction, causing a variety of diseases to appear: from frequent colds and candidiasis to pneumonia, tuberculosis;
- terminal. The stage involves exhaustion (rather rapid and progressive), as well as the subsequent death of the patient.
The stages do not have one correct time frame - they may differ from person to person. For example, HIV-infected people often feel well for years or do not pay attention to small signs. The disease is detected only at the stage of severe deterioration in health or through random tests.
Classification of the disease by stages
During the course of the disease, it is customary to distinguish five successive stages. Each of them has its own specific characteristics. Source: Structural biology of HIV. B. G. Turner, M. F. Summers. Howard Hughes Medical Institute and Department of Chemistry and Biochemistry University of Maryland Baltimore County. https://www.sciencedirect.com/science/article /abs/pii/S0022283698923543?via%3Dihub.
The incubation stage lasts from the period when the virus enters the body until a reaction to it appears (in the form of the symptoms described above) or the production of antibodies. The duration of this stage is from 3-4 weeks to 3 months, in rare cases longer. During this period, viral particles actively spread throughout the body and multiply, but there are no clinical manifestations, HIV is not detected by laboratory tests, but the person is contagious.
The stage of primary manifestations begins approximately 3-6 months from the moment of infection. The virus continues to actively multiply during this period, and the immune system actively reacts to its presence by producing antibodies and clinical symptoms. During this period, the infection can be detected by laboratory examination: a specific test for HIV is performed. During this period, there may be no complaints, or periods of low-grade fever, skin rashes, lymph node reactions, candidiasis, relapses of herpes infection, and pneumonia may occur. The duration of acute HIV infection is 12 months from the moment antibodies appear.
The subclinical stage of infection is characterized by a slowdown in the process of virus reproduction and active synthesis of antibodies to existing particles. Among the leading symptoms are enlarged lymph nodes. The duration of the stage is about 5-7 years, sometimes it can extend to 10-20 years.
The stage of secondary diseases is characterized by the constant multiplication of viral particles, the death of the population of CD4 lymphocytes with the gradual depletion of the immune system resource. This leads to the formation of opportunistic infections (candidiasis, tuberculosis, herpes zoster) and oncological processes (Kaposi's sarcoma). The duration of the stage depends on the activity of treatment of secondary pathologies and the characteristics of the immune system.
The AIDS stage completes the development of the infection. Typically, the development of lesions of the nervous system, secondary severe infections and tumors, which pose a threat to life and occur as generalized processes. Without treatment, AIDS occurs approximately 10-12 years after infection.
Symptoms of HIV
Once you know how HIV is transmitted, you need to understand the symptoms. The problem is that these symptoms appear at an early stage, then disappear and no longer bother the person for a long time - literally for years. They are also very similar to the manifestations of other diseases, which can be misleading.
So, at the first stage, when the virus manifests itself, a person may feel:
- sore throat, fever;
- soreness of the skin, joints, bones4
- chills, fever.
At the same time, the cervical lymph nodes enlarge and various rashes may appear. All this is often mistaken for signs of ARVI or other similar diseases.
New HIV symptoms return after several years of a calm and healthy life. These include:
- severe fatigue, fatigue;
- enlargement of lymph nodes - not only in the cervical, but in several groups;
- weight loss. Usually it looks causeless, the person does not understand what is going on;
- fever, chills, sweating (mostly at night);
- problems with the gastrointestinal tract - usually manifested by loose stools for no apparent reason.
At this stage, as a rule, the disease is detected - because the patient goes to the doctor, and the specialist prescribes an additional examination.
Are you experiencing symptoms of HIV?
Only a doctor can accurately diagnose the disease. Don't delay your consultation - call
Complications
Much attention is paid to the treatment and prevention of infection with the human immunodeficiency virus due to the fact that the infection leads to various severe complications associated with the development of an immunodeficiency state.
Candidiasis of the oropharynx, esophagus and respiratory tract occurs against the background of activation of yeast-like fungi of the genus Candida. Typical symptoms include discomfort when swallowing, sore throat, the appearance of white deposits on the mucous membranes of the mouth, and an increase in temperature to subfebrile levels.
Shingles is a reactivation of the varicella zoster virus, which is stored for life in the nerve ganglia after the initial infection. Itchy blistering rashes appear along the nerve trunks in the back and chest, which form painful and itchy crusts.
Tuberculosis infection is caused by mycobacteria entering the body. Characterized by sweating, cough, fever, shortness of breath. In HIV-positive people, tuberculosis is prone to a severe generalized course, affecting organs other than the lungs.
Kaposi's sarcoma often occurs - a malignant lesion with multiple foci, originating in the vascular area. The skin, mucous membranes, internal organs and lymphatic capillaries are mainly affected.
Pneumocystis pneumonia is a severe lesion of the lung tissue, typical of patients with immunodeficiencies. It is manifested by high fever, severe shortness of breath and severe general condition.
Cerebral toxoplasmosis is a parasitic pathology in which people with immunodeficiencies develop pathological lesions in the brain area, leading to neurological disorders (seizures, headaches, cognitive impairmentSource: Molecular epidemiology of HIV. AJ Kandathil, S Ramalingam, R Kannangai, Shoba David , G Sridharan. Indian J Med Res, 2005 Apr;121(4):333-44. https://pubmed.ncbi.nlm.nih.gov/15817947/.
How is HIV diagnosed in Moscow?
There are two tests to diagnose the virus: preliminary ELISA and the most accurate immunoblot. The accuracy of ELISA is about 90%. It is recommended to carry out it 3-6 months after contact with the virus, then it gives maximum accuracy. The usual ELISA test is based on a blood test, but there are also rapid tests that help obtain information based on urine or saliva. Such texts are purchased exclusively at the pharmacy (in no case on the Internet!), since it is necessary to use officially approved products.
If the rapid test gives a positive result, you need to go to an infectious disease specialist yourself. In such a situation, as well as when ELISA in a blood test gives a positive result, the patient is prescribed an immunoblot. Its reliability is already 99.9%. Depending on the diagnosis, the diagnosis is made either on the basis of two repeated tests or a combination of both. The analysis is rechecked and only after this a diagnosis can be made. This is necessary in order to exclude false positive results that may occur during the diagnostic process.
Important: the test does not show how HIV is transmitted in a particular situation - that is, you can determine the route of infection only by analyzing your own actions.
Publications in the media
HIV infection is an anthroponotic viral infection characterized by slowly progressive immunodeficiency and the associated development of secondary infectious and tumor processes, leading to the death of the patient. The last stage of the disease, manifested by complete decompensation of the immune system, is known as AIDS (acquired immunodeficiency syndrome) Frequency. Currently, the incidence of HIV infection has acquired the nature of a pandemic, which brings the problem to the level of a global catastrophe. It is believed that every hundredth adult inhabitant of the planet is already infected with HIV. According to the UN AIDS Programme, by the beginning of 2000, the infection had claimed the lives of 16.3 million people. By this time, another 33.6 million people were infected with HIV, and during 1999 alone, 5.6 million people became infected. In several countries in Central and Southern Africa, up to 15–20% of the adult population is infected with HIV. In Eastern European countries, including Russia, there has been an intensive increase in the infection rate of the population in recent years. In 2000, 56,471 new cases of HIV infection were registered among Russian citizens, which is 3 times more than registered during the same period in 1999. During the period from January 1, 1987 to April 1, 2001, 103,024 citizens of the Russian Federation were registered infected HIV. According to estimates from the Federal AIDS Center, at the end of 2000, more than 500,000 HIV-infected people lived in Russia.
Etiology. The causative agent is HIV of the genus Retrovirus of the Lentivirinae subfamily of the Retroviridae family. HIV is killed at a temperature of 56 °C for 30 minutes, but is resistant to low temperatures; quickly die under the influence of ethanol, ether, acetone and conventional disinfectants. In blood and other biological media under normal conditions they remain viable for several days. There are 2 types of virus known • HIV-1 (HIV-1; formerly known as HTLV-III or LAV) is common in North and South America, Europe, Asia, Central, Southern and Eastern Africa • HIV-2 (HIV-2) - less virulent virus; rarely causes typical manifestations of AIDS; the main causative agent of AIDS in West Africa.
Epidemiology. The source of infection is a person at any stage of the infectious process. The virus is isolated from blood, semen, vaginal secretions, mother's milk (these fluids determine the route of transmission of the virus), and saliva. Routes of transmission: sexual, parenteral, transplacental, through breast milk. Risk groups • Homosexual and bisexual men (43%) • IV drug addicts (31%) • Heterosexuals (10%) • Recipients of blood and its components, transplanted organs (2%) • Patients with hemophilia (1%).
Classification (Pokrovsky V.I., 1989) • Stage I - incubation • Stage II - primary manifestations •• Phase A - acute infection (mononucleosis-like syndrome) •• Phase B - asymptomatic (latent) •• Phase B - generalized lymphadenopathy • III stage - secondary diseases. Subdivision into phases based on the clinical symptom complex •• Phase A - body weight deficiency up to 10% of the original, superficial lesions of the skin and mucous membranes of fungal, bacterial and/or viral etiology •• Phase B - body weight deficiency more than 10%, recurrent or persistent lesions skin and mucous membranes or internal organs of fungal, bacterial and/or viral etiology, causeless diarrhea and/or fever lasting more than 1 month, recurrent herpes zoster, pulmonary tuberculosis, localized Kaposi's sarcoma •• Phase B - cachexia, generalized infections of various etiologies, disseminated Kaposi's sarcoma, extrapulmonary tuberculosis, atypical mycobacteriosis, Pneumocystis pneumonia, esophageal candidiasis, central nervous system lesions of various etiologies • Stage IV - terminal.
Pathogenesis
• Cell populations affected by HIV •• HIV infects CD4+ cells (monocytes, macrophages and related cells expressing CD4-like molecules), using the CD4 molecule as a receptor; these cells recognize Ag and perform the functions of T-helper/amplifiers •• Infection is possible through phagocytosis of immune complexes containing HIV and Antigen. Infection of monocytes and macrophages is not accompanied by a cytopathic effect, and the cells become a persistent system for the pathogen.
• Tissues in which HIV is able to reproduce in the body of an infected individual •• Lymphoid tissues are considered the main ones. The pathogen reproduces constantly, even in the early stages •• In the central nervous system - microglia •• Intestinal epithelium.
• Early viremic stage •• The virus replicates for various periods of time in small quantities •• Temporary decrease in the total number of CD4+ cells and an increase in the number of circulating HIV-infected CD4+ T-lymphocytes •• HIV circulation in the blood is detected at different times; viremia reaches its peak 10–20 days after infection and continues until the appearance of specific antibodies (until the period of seroconversion).
• Asymptomatic stage. For various periods of time (up to 10–15 years), HIV-infected people have no symptoms of the disease. During this period, the body's defense systems effectively restrain the reproduction of the pathogen •• Humoral reactions - the synthesis of antibodies of various types that are not capable of providing a protective effect and do not protect against further development of infection •• Cellular immune reactions - are capable of either blocking the reproduction of the pathogen or preventing the manifestations of infection. It is likely that cytotoxic reactions dominate in HIV-infected patients with a long absence of clinical manifestations.
• Immunosuppression •• Reduction in the number of circulating CD4+ cells ••• Reduction in the number of circulating CD4+ T cells, which is essential for the replication of integrated HIV. Replication of integrated HIV in vitro is activated by mitotic or antigenic stimulation of infected T cells or concomitant herpes infection ••• A possible reason for the decrease in the number of T cells is the manifestation of a cytopathic effect caused by viral replication. Infection of T cells in vitro is not always productive; the viral genome in an integrated state can remain unexpressed for a long period of time, while the number of T cells constantly decreases ••• The appearance of viral glycoproteins in the membrane of infected T cells is a trigger for the launch of immune mechanisms directed against such cells. Mechanisms of implementation - activation of cytotoxic T cells and the reaction of AT-dependent cytotoxicity ••• Accumulation of non-integrated viral DNA in the cytoplasm of infected cells causes rapid replication of HIV and cell death ••• HIV infects precursor cells in the thymus and bone marrow, which leads to the absence regeneration and reduction in the pool of CD4+ lymphocytes ••• A decrease in the number of CD4+ lymphocytes is accompanied by a decrease in the activity of the TH1 subpopulation of T cells (however, there is no evidence that the activity of TH2 cells increases). An imbalance between the TH1 and TH2 cell subpopulations precedes the development of AIDS. The activity of cytotoxic T cells and natural killer cells decreases, which is associated with a deficiency of CD4+ lymphocytes. The response of B cells also weakens as the numerical reduction of the TH2 subpopulation ••• Defects in humoral responses to various Ags are caused by a deficiency of T helper cells. B lymphocytes are in a state of constant polyclonal activation •• Due to polyclonal activation and a defect in regulatory mechanisms, B cells produce antibodies to HIV Ags with low specificity, cross-reacting with nuclear, platelet and lymphocyte autoantigens.
• Mechanisms that allow HIV to avoid the action of immunological surveillance factors •• Increased humoral anti-HIV response, even more pronounced against the background of AIDS •• Integration of the HIV genome into the host DNA with minimal expression of viral genes •• HIV mutations in the gp120 epitope. HIV mutates much more often than most other viruses because... HIV reverse transcriptase works with errors and lacks corrective activity •• Cellular immune responses.
CLINICAL PICTURE
The incubation period lasts from 2–6 weeks to several months (in most cases) and even several years. Characterized by an asymptomatic course.
Stage of primary manifestations (stage II) - wave-like development of clinical manifestations of the disease • Initial phase of acute infection (phase A) •• In 15% of cases, the so-called mononucleosis-like syndrome (acute retroviral syndrome) develops: an increase in body temperature to 38–39 ° C, widespread peripheral lymphadenopathy, symptoms of pharyngitis (sore throat, catarrhal changes in the oropharynx), exanthema (erythematous maculopapular rash on the face and torso, sometimes on the extremities in the palms and soles) and the appearance of atypical mononuclear cells in the blood •• At the same time, mucosal lesions may develop membranes - aphthous stomatitis, esophagitis, ulcers on the mucous membrane of the genital organs. The patient may be bothered by headache, myalgia and arthralgia, dyspeptic symptoms (nausea, vomiting, diarrhea) •• In some patients, thrush occurs and hepatosplenomegaly is determined. In rare cases, in phase A, a decrease in body weight is noted, neurological disorders occur: aseptic meningitis, meningoencephalitis, neuro- or radiculopathies, neuritis, paresis, etc. Severe acute or subacute encephalitis caused by HIV may develop and is usually fatal. The duration of phase A varies from several days to 3–4 weeks • With regression and disappearance of clinical manifestations, an asymptomatic (latent) phase begins (phase B), it can last several months or years. In this phase there is still no pronounced immunodeficiency, and the diagnosis can only be made in a laboratory based on the detection of specific viral Ags or Abs • Generalized lymphadenopathy (phase B) - lymphadenopathy persists in all subsequent periods of the disease. Suspicion of HIV infection arises in cases where the lymph nodes of at least three different areas located in the upper parts of the body (above the diaphragm) are affected. The diameter of the lymph nodes in adult patients is at least 1 cm, and the duration of manifestations of lymphadenopathy exceeds 2 months • In many patients, there are no primary clinical manifestations; HIV infection proceeds latently until the stage of secondary diseases. The total duration of stage II of the disease varies from 2–3 months to 8–10 years.
The stage of secondary diseases (stage III) is characterized by progressive immunodeficiency, against which opportunistic infections and some oncological processes develop • Phase A: weight loss (up to 10% of initial body weight), superficial lesions of the skin and mucous membranes of fungal, bacterial and/or viral etiology ( herpes simplex and herpes zoster, seborrheic dermatitis, pustular skin lesions, aphthous stomatitis, candidiasis, fungal nail infections, etc.) • In phase B, the loss of body weight exceeds 10% of the original, changes in the skin and mucous membranes become recurrent or persistent. Damage to internal organs of fungal, bacterial and/or viral etiology may develop. “Unreasonable” diarrhea with a stool frequency of 3 times a day or more and/or fever lasting more than 1 month is added. Diarrhea is often etiologically associated with cryptosporidium or other protozoa that are not very pathogenic for humans. In addition, pulmonary tuberculosis, recurrent herpes zoster, localized Kaposi's sarcoma can be detected in patients • Phase B: cachexia, development of oncological processes (disseminated Kaposi's sarcoma, malignant lymphoma), central nervous system lesions (dementia, encephalitis, peripheral polyneuropathy, etc.). Opportunistic infections are extremely diverse in etiology, take on a generalized nature and often occur as mixed infections. Patients in the Russian Federation most often experience herpes simplex and herpes zoster, CMV infection, esophageal candidiasis, cryptococcosis, cryptosporidiosis, toxoplasmosis, Pneumocystis pneumonia, extrapulmonary tuberculosis, atypical mycobacteriosis, etc.
The terminal stage (phase IV) continues until death.
Concomitant diseases • Syphilis (more severe in HIV-infected people) • Tuberculosis. Patients with tuberculosis are tested for HIV, or, if this is not possible, they are treated comprehensively, according to the regimen used to treat tuberculosis in HIV-infected people.
RESEARCH METHODS. Diagnostic algorithm: ELISA (primary isolation of antibodies to HIV), if the result is positive, immunoblotting to confirm the diagnosis. If the result of immunoblotting is negative, it is advisable to test the blood using the PCR method to identify the replicating virus • Solid-phase ELISA detects antibodies to HIV • • The antibodies detected by ELISA appear in the blood approximately 2 months after infection. In 95% of infected people, they appear only after 5–8 months •• Antigenemia is detected by a modified enzyme-linked immunosorbent test that detects p24 Ag in blood serum treated with acid (as a result of the procedure, immune complexes are destroyed and Ag is released) • Western blotting (immunoblotting) is used to confirm diagnosis of HIV infection. The method detects specific antibodies in blood serum and is only a confirmatory test. The results are considered positive after detection of antibodies to p24, p31, gp41, gp120 •• It is recommended to use reactions with two Ags from three groups: p24, gp41 and gp120/160. If the results are uncertain, the study is repeated after 3 and 6 months •• Antibodies to p24 Ags appear 6 weeks after infection (ABs to gp120 and gp41 are detected earlier). Since AT is usually absent during the initial manifestations of infection, a seronegative patient who belongs to a high-risk group should undergo a repeat test after 6 weeks. In rare cases, seroconversion may take a year or more to occur. The p24 Ag test is positive in 85–95% of infected children aged 4–6 months; Ag is detected much less frequently in children under 4 months of age •• In the later stages of HIV infection, the results of serological studies may be false negative, which is due to a decrease in antibody titers and the level of formation of daughter populations of the pathogen due to a general decrease in sensitive immunocompetent cells •• Methods that detect antibodies not suitable for diagnosing HIV infection in newborns, because maternal IgG can be present in the child's serum for up to a year or more • Alternative research methods •• Viremia is detected in cell culture in vitro and PCR with the patient's blood •• Isolation of the virus in vitro and identification of the genetic material of the causative agent by PCR. Results are positive in 35–55% of infected neonates less than 1 week of age and in 90–100% of children 3–6 months of age • Determine the progressive decline in the number of CD4+ lymphocytes •• Identify markers of leukocyte activation, such as molecules released during T activation -lymphocytes (b2-microglobulin, soluble IL-2 receptor, soluble CD8), and a molecule released during the activation of monocytes (neopterin) •• A constant increase in the content of b2-microglobulin and neopterin is characteristic of the weak development of symptomatic infection. The combination of a decrease in the number of CD4+ cells and an increase in the level of b2-microglobulin or neopterin, or a decrease in CD4+ cells and the detection of Ag p24 indicates a more reasonable prognosis for the development of AIDS than simply a low level of CD4+ lymphocytes • Serological tests for toxoplasmosis. In 80%, toxoplasmosis develops after a decrease in the number of CD4+ cells to 100/μl or below • Study of biopsy material from the skin of the perianal area in HIV-positive women, because they are more susceptible to HPV infection.
TREATMENT
Management tactics • Collecting the most complete information about past diseases and the results of their treatment • Thorough examination of the patient by organs and systems, pay attention to fever of unknown origin, prolonged diarrhea, weight loss, adenopathy, oral ulcers, dysphagia, cough, increased breathing , shortness of breath on exertion, skin rashes, sinusitis • The frequency of examinations is determined by the clinical picture, the mental status of the patient, the need to control the function of the immune system and the development of side effects of drugs • During subsequent visits to the doctor, a complete and thorough physical examination of all organ systems is performed • Determination of T-helper levels is carried out depending on the stage of the disease every 3-6 months • The reproductive activity of the pathogen is determined by qualitative PCR • HIV-infected women have an increased risk of developing cervical cancer. Pap smears should be performed every 6 months or more frequently.
Etiotropic treatment • At least 2 drugs are prescribed simultaneously to prevent the rapid development of resistance. The likelihood of developing many side effects of drugs should be taken into account: • HIV reverse transcriptase inhibitors • • Zidovudine 500–1,500 mg/day in 4–6 doses. Recommended for CD4+ cell counts >500/µl; pregnant HIV-seropositive women (between 14 and 34 weeks of pregnancy); persons infected with HIV (for example, through a needle stick); children under 6 weeks born from HIV-infected mothers. Contraindicated in cases of severe neutropenia or a significant decrease in Hb concentration. During treatment, it is recommended to conduct blood tests every 2 weeks during the first 3 months, then at least 1 time per month •• Zalcitabine 0.75 mg 3 times per day; recommended for late stage disease (monotherapy for intolerance or ineffectiveness of zidovudine or in combination with zidovudine). If side effects occur (most often anemia and neutropenia), the drug is discontinued or the treatment regimen is adjusted. It should be used with extreme caution in cases of peripheral neuropathy, pancreatitis and a history of congestive heart failure, cardiomyopathy. During treatment, a systematic study of general and biochemical blood tests is recommended • Didanosine 125–200 mg every 12 hours 30 minutes before meals; most effective in combination with azidothymidine. Side effects: pancreatitis, nausea, vomiting, abdominal pain, dyspepsia, peripheral neuropathy, etc. If signs of pancreatitis appear, treatment should be stopped. Prescribe with caution if there is a history of pancreatitis, alcohol abuse, or impaired renal function. Antacids containing magnesium or aluminum increase side effects. Concomitant use with tetracycline is not recommended • Protease inhibitors (most effective in combination with reverse transcriptase inhibitors) • Saquinovir 600 mg 3 times a day. Contraindicated in children under 13 years of age. Side effects: headaches, myalgia, rash, itching, ulceration of the oral mucosa, nausea, diarrhea, etc. Should be used with caution in cases of liver and kidney damage. Ketoconazole increases, and rifampicin reduces, the concentration of the drug in plasma •• Indinavir 800 mg 3 times a day (for liver failure, nephrolithiasis, in combination with ketoconazole - 600 mg 3 times a day). Contraindicated for children. When taking the drug, it is recommended to drink at least 1.5 liters of liquid per day. Monitoring for signs of nephrolithiasis is necessary. Compatible with co-trimoxazole, fluconazole, isoniazid, clarithromycin, and oral contraceptives. Combinations with rifampicin, cisapride are not recommended • Inhibitors of the assembly and maturation of daughter populations, for example a-IFN.
Prevention of opportunistic infections. • Pneumonia caused by Pneumocystis carinii - to all patients with a history of pneumocystis; with a CD4+ cell count <200/mm3 (in adults) or with fever of unknown origin and candidiasis •• The drug of choice is co-trimoxazole (18.75–25 mg/kg sulfamethoxazole, 3.75–5 mg/kg trimethoprim every 6 hours). When combined with zidovudine, regular blood tests are necessary •• In case of intolerance or resistance to co-trimoxazole - dapsone orally. • Pneumonia caused by Streptococcus pneumoniae - pneumococcal vaccine (Pneumo 23) every 5 years • Influenza infection caused by viruses type A and B - annual influenza vaccination • Cryptococcal meningitis - amphotericin B for active disease, fluconazole for primary prevention or preventing relapses • Cerebral toxoplasmosis - pyrimethamine and sodium sulfadiazine (or clindamycin); co-trimoxazole for primary prevention • For mycobacterial infection •• Infection caused by Mycobacterium tuberculosis - isoniazid daily for 1 year •• Infection caused by Mycobacterium avium-intracellulare - rifampicin (in patients with symptoms of AIDS or with a decrease in the count of CD4+ cells <200/mm3) • For CMV chorioretinitis - ganciclovir • Bacterial and viral superinfections in children - immunoglobulin 1 r/month IV (infected children not receiving etiotropic therapy).
Course and prognosis. After an asymptomatic period, 80–100% of patients develop symptomatic HIV infection, and about 50–100% will develop clinical AIDS. After the transition from HIV infection to AIDS, life expectancy does not exceed 2–3 years. Until the CD4+ lymphocyte count falls below 200/mm3, AIDS (including opportunistic infections) usually does not develop. During HIV infection, the number of T helper cells decreases at a rate of 50–80/μl/year, with a more rapid decline in their number once the level reaches 200/μl.
Prevention • Changing the attitude of society to the problems of extramarital sexual relations, prostitution, homosexuality • Educating young people about morality, responsibility and appropriate hygienic skills • Teaching the population correct sexual behavior: limiting the number of sexual partners and using condoms • In medical institutions it is necessary to follow the rules for the use and sterilization of syringes , needles and other instruments • Combating drug addiction. IV drug addicts make up the main group of newly diagnosed HIV-infected people in the Russian Federation.
ICD-10 • B20 Disease caused by HIV, manifested by infectious and parasitic diseases • B21 Disease caused by HIV, manifested by malignant neoplasms • B22 Disease caused by HIV, manifested by other specified diseases • B23 Disease caused by HIV, manifested by as other conditions • B24 Disease caused by HIV, unspecified
HIV treatment
Treatment boils down to prescribing antiretroviral therapy. The patient is given a medication regimen - and it must be followed as precisely as possible, without deviating from the program. Otherwise, the virus may develop resistance to treatment and cannot be further suppressed.
Indicators of quality treatment are a decrease in the viral load, as well as an increase in CD4+ cells in the blood, which indicates the activity of the immune system.
Medicines for treatment are issued in medical institutions, patients are registered and receive medications free of charge, in accordance with the established procedure. Information about the disease is confidential - it is not sent to work, place of study or other places. The patient has the right to keep it secret (if this is not provided for in separate work contracts).
If the rules for taking therapy are followed, the virus in the blood gradually decreases; over time, the patient becomes completely safe for his sexual partner and is not able to infect anyone.
How to treat HIV
If an infection is detected, the patient is registered with the AIDS Center and is constantly monitored by an infectious disease specialist. Today, a cure for HIV has not yet been developed that could completely suppress the infection. But clinical recommendations for the management of patients with HIV have been developed and put into practice, and antiretroviral drugs are used to prevent the development of AIDS and significantly prolong life. They are issued free of charge after a full examination and continuous monitoring by a doctor. Source: HIV infection: issues of therapy. Aronin Steve I. Kazan Medical Journal No. 6, 2005. p. 433-450.
Taking antiretroviral therapy suppresses the process of reproduction of viral particles, which prevents the infection from destroying the immune system. Patients who constantly take drugs do not transmit the infection even during sexual intercourse without condoms, and do not infect children during pregnancy and childbirth.
It is important to use the drugs selected by the doctor for life; the effectiveness of treatment is constantly monitored and patients are monitored to exclude side effects from the drugs.
Prevention of HIV infection
The first and most important rule is to be regularly tested for HIV, even if you have not had suspicious contacts. It is recommended to be examined once every six months - especially since there are convenient rapid tests for this.
You also need to be careful when choosing partners. You should not take the word of a person who says that he is definitely not sick - it is better to ask for the results of the study and see for yourself that you can trust him. But remember that within six months even contaminated blood may not give positive results.
HIV prevention consists of the following points:
- protected sex with non-regular sexual partners, as well as regular ones, if there is no confidence that the partner is not sick or is faithful;
- exclusion from life of drugs and promiscuity;
- maintaining general hygiene. Avoid sharing razors, toothbrushes, nail clippers, and other items that may come into contact with small wounds.
The main prevention is to be aware of the infection and always remember the danger of infection.
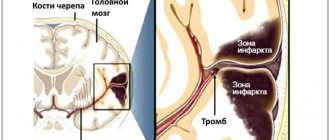
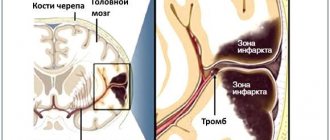
Basic mechanisms of development of HIV infection and AIDS
The main target of HIV is CD4 lymphocytes, which play an important role in the formation of human immunity. After initial infection, HIV remains in the person's body for the rest of his life. Constant multiplication of the virus (replication) occurs in the lymphoid organs throughout the entire period of HIV infection. As a result of the action of HIV, lymphoid tissue is destroyed, leading to immunity disorders and progressive depletion of the immune response to a variety of pathogens. Accordingly, the body, left without a protective immune barrier, becomes unable to resist even the most harmless diseases for a healthy person. AIDS develops - the final stage of HIV infection.
Popular questions and answers about HIV
How does HIV manifest in men and women?
The symptoms of HIV in women are exactly the same as the symptoms of HIV in men. Manifestations may differ only at the level of genitourinary diseases, when the body is already very weakened - for example, thrush appears more often in women. Otherwise, there are no specific signs by gender.
Is there a cure for HIV?
Technically, we can say that there is no cure for HIV - patients are constantly required to undergo special therapy. But the results that it allows to achieve make the patient a healthy person who can live calmly for decades without any problems - you just need to constantly take medications and monitor your health.
HIV has not been a fatal disease for a long time!
Is HIV a disease of drug addicts and people with disordered lifestyles?
In fact, this is a myth that HIV activists are constantly dispelling. Unfortunately, a person who leads a healthy lifestyle and is responsible for their relationships can also get this disease. It is enough that a sexual partner can cheat – and in this way “bring” illness to the couple. HIV is not always a sign of an irresponsible attitude towards one’s life.
Who are HIV dissidents?
These are people who, contrary to scientific data and common sense, deny the existence of the virus. They refuse treatment, which inevitably leads to early death. Such people are also dangerous because, due to lack of treatment, they spread the virus among their sexual partners without warning them of the possible danger (because they do not believe that it exists).
The success of HIV treatment and long life lies in seeking help and starting therapy as early as possible. In this case, a person will have a long life without fears and difficulties.