The concept of “neuroinfection” includes all kinds of infectious diseases of the nervous system. This is a fairly common group of pathologies, with a severe course and a serious prognosis, characterized by damage to the anatomical structures of the nervous system with a high risk of death. It is possible to minimize negative consequences by contacting specialists as quickly as possible and carrying out the necessary diagnostic procedures.
Neuroinfections are divided into several types depending on the pathogen that caused the disease. Conventionally, five groups can be distinguished:
- bacterial;
- parasitic;
- fungal;
- viral;
- prion (obtained through prions - protein structures with an abnormal three-dimensional configuration, capable of transforming ordinary proteins of their own kind).
There are also several ways for infection to enter the body. As a rule, the following mechanisms are distinguished:
- airborne - most typical in the occurrence of viral and bacterial meningitis, herpes, encephalitis and polio;
- contact-household - occurs through direct contact with a sick person or contaminated household items. This is how infection occurs with polio, syphilis, and herpes;
- traumatic – from animal bites;
- hematogenous - usually found in the bacterial form. The disease is transmitted through the lymphatic tract and blood vessels to the central nervous system, most often in the presence of sinusitis, frontal sinusitis, otitis media, abscesses;
- fecal-oral – the infection enters the body with food, water and feces. This type of transmission is characterized by damage by ECHO, herpes, and botulism viruses;
- genital - through the mucous membranes of the genital tract. This mechanism transmits diseases such as HIV, encephalitis, and meningitis.
Neuroinfections are also classified according to the time criterion - the period of penetration of the pathogen into the brain:
- rapid – in the case when symptoms appear within a few hours after infection;
- acute - signs manifest themselves by the end of the next day;
- smooth or subacute - the clinical picture is visible on the second to seventh day;
- chronic - the appearance of symptoms occurs against the background of the development of other diseases, such as HIV, tuberculosis.
In addition, neuroinfections are divided into primary and secondary. In the primary case, the infection enters human cells from the outside. In secondary cases, the process develops as a complication of an existing pathology. Neuroinfectious diseases include meningitis of various forms, encephalitis, myelitis, arachnoiditis, tetanus, rabies, neurosyphilis, neurobrucellosis, neuroAIDS.
The danger lies precisely in the fact that initially these ailments have symptoms of a common cold, which, in the absence of careful attention and proper examination, can lead to irreparable results.
Causes
The etiological factor in the appearance of the disease is the pathogenic effect of pathogens on the human body, which is largely facilitated by:
- hypothermia;
- suffered from acute respiratory viral infections;
- traumatic brain injuries;
- introduction of infection from outside.
As a rule, neuroinfections appear due to existing foci of any purulent infections, lack of control after a severe viral illness, as well as a reduced level of immunity.
Symptoms
Symptoms often depend on the pathogen, the form of introduction and the severity of the pathology. However, there are basic signs, including:
- intoxication of the body (low-grade fever, sometimes the temperature reaches high values, severe weakness, pain in the head);
- liquor hypertension syndrome, manifested by morning headaches when lying down;
- cerebrospinal fluid syndrome (a sharp increase in protein in the cells of the cerebrospinal fluid);
- dizziness;
- low systolic blood pressure;
- irritability and aversion to loud noises and excessive light.
In the case of the development of processes with localization on the membranes of the brain, meningeal syndrome appears. It is characterized by muscle rigidity and Kerning and Brudzinski signs. If the central nervous system is affected, extrapyramidal syndrome, paresis, and all kinds of psycho-emotional disorders are possible. Damage to the peripheral nervous system is characterized by temporary immobility. There may be significant pain in the calf muscles, which may cause a change in gait. In the future, this can lead to paralysis.
Diagnosis
A comprehensive assessment of the patient’s condition is necessary, as well as careful collection of anamnestic data, especially related to the epidemiological component (cases of similar diseases in the patient’s environment, tick bites, presence of pets, previous infections, membership in risk groups, etc.). Indications for examination are signs of general infectious intoxication, accompanied by syndromes: increased intracranial pressure, cerebral edema, damage to the meninges or cephalic syndrome. Considering the similarity of symptoms when the central nervous system is infected with different pathogens, identification of the etiology of the disease should occur only using laboratory diagnostic methods. To do this, first of all, the cerebrospinal fluid and blood of patients are examined using direct (visual detection of the pathogen using microscopy, isolation in cell culture, detection of its antigens or fragments of genetic material) and indirect laboratory methods.
Given the severity of the disease, special attention is paid to diagnostic and laboratory tests to determine the type of pathological agent.
- MRI – to recognize the location of inflammatory foci and their characteristics;
- electroneuromyography – to analyze the functioning of the brain and nerve cells;
- electroencephalography – for differential diagnosis with other lesions of the central nervous system and assessment of the degree of damage to this body system;
- lumbar puncture - to study the cerebrospinal fluid spaces.
Return of neuroinfections to the clinic
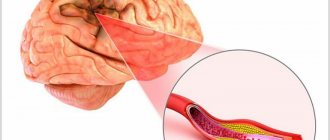
Among the infections that have returned to the clinic, syphilis, classified as a socially significant disease, should be mentioned. Syphilis is a serious problem and requires special attention from doctors of all specialties. In the mid-90s. last century, there was an extremely rapid increase in the incidence of syphilis; currently it is decreasing, but this figure exceeds 60 per 100 thousand population, which is significantly higher than in the European Union countries. At the same time, there is an increase in the incidence of neurosyphilis, especially its late forms. It is damage to the nervous system that leads to life-threatening conditions: meningovascular syphilis is one of the leading causes of stroke in young and middle-aged people. Syphilitic meningoencephalitis and meningomyelitis are life-threatening and lead to catastrophic disability [1, 2].
A number of neuropsychiatric disorders, such as mild cognitive impairment, dementia, bipolar psychoses, and delirium caused by neurosyphilis, are also quite well known. These disorders significantly worsen the condition of patients and can pose a threat to their life. We should not forget about the catastrophic complications in the treatment of neurosyphilis – the Jarisch-Herxheimer reaction [3, 4].
Another group of socially significant infectious diseases is hepatitis B and C. There are a large number of reports of severe life-threatening complications of these diseases, such as coma, hepatic encephalopathy, and parainfectious inflammatory demyelinating polyneuropathy [5–7].
Although herpes infection does not directly relate to socially significant infections, in terms of the rate of spread and severity of damage to the nervous system, diseases caused by various types of herpes viruses are close to them. Currently, there are a large number of observations of damage to the nervous system; It has also been noted that the addition of a herpes infection leads to aggravation of the course of many neurological diseases [8, 9].
Despite the large number of cases of neurological disorders caused by infectious pathogens, the study of the clinical picture and pathogenetic mechanisms continues, the influence of such pathogenetic factors as microcirculatory disorders, impaired permeability of the blood-brain barrier, neurodegenerative process, cognitive deficit, inflammatory and autoimmune disorders, etc. is being clarified. Knowledge of pathogenetic mechanisms development of the infectious process can optimize the management of patients, reduce disability and mortality. Let's look at some of the infectious lesions of the nervous system.
Bacterial meningitis
Despite the advances of modern medicine, bacterial meningitis of various natures remains a common and most severe infectious disease. Every year, more than 1.2 million cases of bacterial meningitis are recorded worldwide, with more than 135 thousand cases of the disease ending in death, despite the emergence of highly effective new generations of antibiotics. Thus, bacterial meningitis is one of the ten main infectious causes of mortality. Mortality in adults reaches 25%, and among survivors, about 20% have severe neurological disorders [10].
Among the causative agents of bacterial meningitis, the first place in frequency is occupied by pneumococcus (71%), which is explained by the high frequency of pneumococcal infection in the population. Meningococcal infection caused by Neisseria meningitides is detected in 12%, group B streptococci (colonizing the gastrointestinal tract and vagina) - in 7%, Haemophilus influenzae (Pfeiffer bacillus) - in 6%, gram-positive Listeria monocytogenes - in 4% of cases. In elderly people, it is the second most frequently detected causative agent of bacterial meningitis, found in 20% of cases. The causative agents of nosocomial (nosocomial) bacterial meningitis are often staphylococci and aerobic gram-negative bacteria, which cause disease in persons with ventricular drainage after neurosurgical interventions, as well as in patients after traumatic brain injury [11]. The clinical picture of bacterial meningitis is well known and has been described many times, so we will refer to the most informative publications [12, 13]. The most well-known clinical triad of symptoms: fever, stiff neck muscles and mental disorders (from mild stupor to infectious delirium), detected in the vast majority of patients. Severe diffuse headache, photophobia, and hypersensitivity are also associated with this diagnosis.
In elderly patients, especially those suffering from diabetes mellitus and cardiopulmonary diseases, the course of the infection may be atypical, fever may be absent, symptoms of meningeal irritation are mild and transient, and lethargy and drowsiness come first.
Additional (but optional) manifestations of bacterial meningitis may include epileptic seizures, cranial nerve palsies (Listeria), papilledema, hearing loss up to deafness, as well as signs of damage to other organs and systems - skin rash (meningococcus), arthritis, sinusitis and etc.
The most conclusive way to diagnose bacterial meningitis is a spinal puncture. Relative contraindications to it are increased intracranial pressure, suspicion of a mass formation in the brain, the presence of focal symptoms, thrombocytopenia, hemorrhagic diathesis, purulent processes in the lumbosacral region. Often, X-ray computed tomography (XCT) is used as a screening test if there are signs of increased intracranial pressure before a spinal puncture, but performing an X-ray CT scan should not delay its implementation and the initiation of antibacterial therapy. Most patients with suspected meningitis do not need a brain scan before undergoing a lumbar puncture.
It is imperative to perform an RCT of the brain before performing a spinal puncture [14] in patients who have:
- history of a brain mass, stroke, or CNS infection;
- repeated seizures;
- swelling of the optic discs;
- impaired consciousness, especially if the Glasgow Coma Scale score is below 11 points;
- focal neurological signs, including impaired pupillary reactions, instability, etc.;
- breathing rhythm disturbances;
- combination of arterial hypertension and bradycardia.
If lumbar puncture is delayed or delayed, empirical antibiotic therapy is prescribed. Glucocorticoids (dexamethasone) should be administered immediately before or simultaneously with the initiation of antibiotic therapy, and if antimicrobial therapy is not administered, steroids should not be prescribed [15].
Bacterial meningitis is a life-threatening disease; therefore, a delay in prescribing antimicrobial therapy worsens the prognosis of the disease. If bacterial meningitis is suspected, antibiotic therapy should not be delayed until the results of a cerebrospinal fluid test are available. Although the antibiotic should be selected based on the type of pathogen and determination of its sensitivity, while awaiting the results of the study, which can be obtained in 2 or even more days, empirical therapy is prescribed that is effective against the most common pathogens. The basic drugs are cephalosporins, such as ceftriaxone or cefotaxime, and additionally vancomycin for a more effective effect on gram-positive microorganisms resistant to cephalosporins. The effectiveness of the combination of chloramphenicol with ampicillin has also been shown [10, 11]. For patients over 50 years of age, as well as for those with weakened immune systems, ampicillin is added to protect against listeria infection. The effectiveness of antibiotic therapy for bacterial meningitis is mainly due to the ability of the drug to penetrate the blood-brain barrier.
Additional administration of corticosteroids (usually dexamethasone) is indicated, especially for pneumococcal meningitis. Studies have shown that when glucocorticoids are prescribed as part of complex therapy, mortality and neurological disability are reduced. It is recommended to prescribe steroids before the first dose of antibiotic, duration – 4 days.
Encephalitis
The difference in the clinical manifestations of meningitis and encephalitis is mainly associated with the anatomical substrate: with meningitis, the infection affects the meninges, with encephalitis - the brain parenchyma. With encephalitis, various disorders of brain functions are detected, for example, changes in mental state, behavior and personality, motor or sensory deficits, disturbances of speech and other higher cortical functions, epileptic seizures, etc. The importance of identifying the differences between meningitis and encephalitis is due to the fact that the most common pathogens of these diseases are different [16].
The first place in frequency among the causative agents of encephalitis is occupied by herpes viruses. The most commonly detected herpes virus type 1 in many cases causes bilateral damage to the temporal lobes, which often becomes necrotic (Fig. 1).
Among the viruses that cause encephalitis in humans, LH Taylor et al. [17] approximately 80% were classified as zoonotic. Therefore, increased contact between people and animals, especially wild ones, is an important risk factor for increasing the incidence of encephalitis. Considering the vector-borne route of transmission of up to 40% of viral zoonotic encephalitis, it can be assumed that contact with mosquitoes and arthropods is an important factor in increasing the prevalence of diseases.
Factors that have led to an increase in the incidence of zoonotic encephalitis are, in particular, climate change and climatic anomalies, including global warming, which has probably become key in the expansion of transmission of the pathogen to humans, an example being the emergence of cases of West Nile fever in the Moscow region area (Fig. 2). An important factor is the increase in the population of people with immunodeficiency, which increases susceptibility to infections due to the widespread use of drugs for the treatment of autoimmune diseases, as a result of chemotherapy for malignant diseases and the growing incidence of AIDS [18].
Signs in favor of encephalitis on cerebrospinal fluid examination include moderate pleocytosis (usually <250 in mm3) with a predominance of lymphocytes (but at the onset of the disease neutrophils may predominate), a slight increase in protein concentration (usually <1500 mg/l), normal glucose levels (more than 50% on blood glucose levels). The presence of red blood cells in the cerebrospinal fluid may indicate necrotizing encephalitis (herpes simplex virus type 1).
The treatment strategy for encephalitis is different; in the case of a specific vaccine, it is based on its use. Acyclovir and more active analogues are used for infections from the herpes group. Considering the role of autoimmune processes, glucocorticoid therapy occupies an important place, the effectiveness of which is higher after a preliminary course of plasmapheresis.
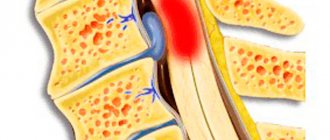
Intracranial abscesses
Purulent intracranial processes occur in the form of an abscess or empyema. An abscess is characterized by a local accumulation of pus, surrounded by a capsule, located in the brain parenchyma or in the epidural space. With empyema, purulent masses are not localized; the most common accumulation of pus is between the dura and arachnoid maters (for example, in the subdural space). Although intracranial purulent processes are rare, their development is life-threatening, and diagnosis is delayed.
There are several mechanisms for the occurrence of intracranial purulent processes. The hematogenous path of development, emanating from distant areas, often leads to multiple formation of purulent foci in the substance of the brain, more often in the blood supply of the middle cerebral artery. Currently, when people with immunodeficiency constitute an increasingly large stratum in the population, these diseases have begun to be observed more often (Fig. 3).
The spread of infection from a purulent focus in the neighborhood is observed with sinusitis, otitis media, and diseases of the oral cavity (Fig. 4).
Direct exposure to an infectious agent is possible during penetrating brain injuries and surgical interventions. Often this mechanism of infection leads to the development of massive intractable purulent lesions of both the membranes and the substance of the brain (Fig. 5).
Clinical manifestations of intracranial purulent process are variable and depend on the location and volume of brain damage. As a rule, all the symptoms of the infectious process are present, including fever. Hypertensive headache is the most common symptom. Neurological manifestations depend on the localization of the process. Diagnosis is carried out using neuroimaging, and round formations and cavities with liquid contents are identified; It should be noted that MRI is more informative than RCT, however, RCT with contrast can significantly speed up the diagnostic process.
In the treatment of purulent processes in the cranial cavity, neurosurgical assistance comes first, but antibiotic therapy is prescribed immediately, taking into account the sensitivity of the pathogen.
This article presents fairly brief descriptions of only a few forms of neuroinfections, which have become increasingly common in recent years in neurological clinics, especially in emergency hospitals. One can also mention botulism, spondylitis and their neurological manifestations, spinal epidural abscesses, postherpetic neuralgia, which have become a serious problem in patients with immunodeficiency. Spirochetoses - syphilis and Lyme borreliosis - are becoming increasingly common in neurological clinics. We should not forget about tuberculosis of the nervous system, the clinical manifestations of which are quite varied. The purpose of this article is to attract the attention of specialists to neuroinfections at the current stage of development of neurology.
Consequences
These infections can sometimes lead to extremely severe results, which are largely related to the part of the brain where the lesion is located.
Almost all those who have recovered from neuroinfectious diseases still have headaches and back pain, aggravated by weather changes, and their memory is weakened. In some cases, the acquisition of epileptic syndrome and hydrocephalus, speech disorder, and disruption of motor functions. Sometimes complete disability occurs, with loss of memory, vision and hearing.
The most serious damage to the nervous system occurs to those who suffered it in the prenatal state. In this case, we can talk about irreparable disorders in the central nervous system and anomalies in the development of internal organs.
The consequences of neuroinfections affect, as a rule, throughout subsequent life. Therefore, immediate medical attention and a timely set of examinations will help prevent deterioration in health after illness.
Material and methods
Clinical material includes data from a non-selective examination of 46 patients aged 18 to 83 years, admitted in 2010-2016. to the department of acute neuroinfections or the intensive care unit of the Infectious Clinical Hospital No. 1 of the Moscow Department of Health. Among them were 13 patients with non-traumatic subarachnoid hemorrhage (SAH), 15 with consequences of TBI, 7 with abscesses, 7 with brain tumors, 4 with CNS lymphomas. The results obtained in this group of patients were compared with data from a retrospective analysis of 128 case histories of patients with bacterial infections with purulent meningitis for 2005-2007. and 5 patients (with meningitis, pneumococcal, hemophilus influenzae infection, listeriosis, enteroviral disease) with meningitis in 2013-2014.
All patients underwent standard clinical-neurological, laboratory and instrumental examination (general blood test, urine test, chest x-ray, paranasal sinuses, ECG, biochemical blood test). Cell counting and determination of protein and glucose levels in the CSF were performed using routine methods in the clinical laboratory of the hospital. As differential signs of the activity of the systemic inflammatory response, the content of C-reactive protein (CRP) in the blood serum and lactate in the CSF were determined [10, 20]. The immunophenotypic characteristics of CSF cells of patients with neuroleukemia were also established.
Bacteriological testing was carried out in the microbiological laboratory of the hospital. It included generally accepted techniques: 1) microscopy of Gram-stained CSF smears; 2) setting up a latex agglutination reaction (immunochemical analysis) as a rapid method for detecting specific antigens of the main pathogens of bacterial infections in the CSF [21]; 3) the classical bacteriological method of inoculating CSF and blood on nutrient media1 [22]; 4) PCR.
Along with laboratory tests, modern radiation diagnostic methods were used: MSCT, MRI of the brain.
Treatment principles
Treatment should be differentiated, i.e. depend on the type of neuroinfection because There is no effective etiotropic therapy:
- for bacterial purulent meningitis and viral encephalitis during the acute period of the disease, antibacterial and antiviral drugs are prescribed;
- pathogenetic therapeutic measures include the use of decongestants, anticonvulsants, detoxification agents, no less important are: maintaining adequate oxygenation, correction of water-electrolyte and acid-base disorders;
- symptomatic treatment (antipyretic, restorative vitamin therapy).
Varieties
Neuroinfections in children and adults can occur in acute and chronic forms. The following diseases are classified as acute:
- myelitis;
- tetanus;
- encephalitis;
- rabies;
- meningitis;
- arachnoiditis.
Chronic types of neuroinfection of the brain:
- brucellosis;
- neurosyphilis;
- neurobrucellosis;
- neuroAIDS.
Neuroinfection according to the ICD does not have its own code, but the pathologies that are included in this group have a code. For example, the rabies code according to ICD-10 is A82.