Authors: Heron Werner, Taisa Davaus Gasparetto, Pedro Daltro, Emerson Leandro Gasparetto, Edward Araujo Júnior
What is pregnancy screening
Thanks to the study, the doctor can diagnose certain developmental defects with certain accuracy.
Such a study includes the following procedures:
- Blood test from a vein
- Ultrasound
In Russia, only routine ultrasound is inevitably prescribed. Full screening is not recommended in all cases. If your doctor insists on having it done, then you shouldn’t worry or get upset in advance. As a rule, it should be done in the following situations:
- if the pregnant woman is over 35 years old;
- if the child’s father is over 40 years old;
- one of the family members has genetic pathologies;
- the woman suffered an infection during pregnancy;
- the pregnant woman took medications that may adversely affect the development of the child;
- women's work in hazardous industries.
The importance of early detection of any pathologies can be noted. After all, this is what makes it possible to begin the necessary treatment as early as possible. If during screening the doctor sees certain deviations from the norm, then the pregnancy is monitored more carefully and seriously.
Screening during pregnancy is done three times. If necessary, there is the possibility of additional examination.
Brain and central nervous system defects
Anencephaly
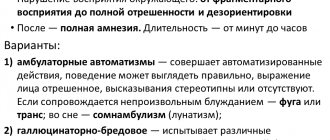
Anencephaly refers to defects in the fusion of the anterior neural tube, with an overall incidence of approximately 1 in 1000 births and a fatal prognosis. Anencephaly is characterized by the absence of the cranial vault, which leads to exposure of nervous tissue. Early diagnosis can be easily made using ultrasound in the first trimester (Figure 1).
Figure 1:
Fetus at 13 weeks with exencephaly. A . Sagittal ultrasound shows a flat head (arrow). B, C. Coronal (left) and sagittal (right) T2-weighted images (B) and 3-dimensional magnetic resonance imaging reconstruction images show dysmorphic brain tissue in the amniotic cavity (arrows).
Ventriculomegaly
Ventriculomegaly is one of the most common pathological changes in the brain. It is associated with an imbalance between the production and reabsorption of cerebrospinal fluid, which leads to an excess of the latter. As a result, the lateral ventricles may exhibit varying degrees of enlargement, which may or may not be related to dilatation of the third and fourth ventricles. The term ventriculomegaly is used only when the width of one or both ventricles, measured at the level of the glomus, is ≥10 mm at any stage of pregnancy.
In cases where ventriculomegaly is detected by ultrasound, MRI is useful in assessing the brain parenchyma as well as assessing associated malformations (Figure 2).
Associations with other anomalies occur in approximately 70-85% of cases, including myelomeningocele (30%) and brain injuries such as agenesis of the corpus callosum, cortical malformations, periventricular heterotopia, cerebellar malformations, periventricular white matter damage, etc. Additionally , there may be defects affecting the heart, chest, kidneys, abdominal wall, face and limbs. However, in some cases, ventriculomegaly is the only pathological finding, which is called isolated ventriculomegaly. In such cases, the risk of developing aneuploidy may be higher and more specific analysis is necessary (Fig. 3).
Figure 2:
Fetus with left ventricular dilatation at 35 weeks. A-C . Axial ultrasound (A), axial T2-weighted (B), and coronal T2-weighted (C) magnetic resonance imaging images show left ventricular dilatation (asterisks). In the left hemisphere, close to the left ventricle, a heterogeneous signal is present (C, arrow). E. _ Sagittal T2-weighted image shows narrowing of the brainstem (arrow). F. _ An axial diffusion-weighted image (left) and corresponding apparent diffusion coefficient map (right) show a hematoma close to the left ventricle (arrows).
Figure 3:
Fetus with ventriculomegaly at 34 weeks.
Sagittal T2-weighted (left) and 3-dimensional reconstructions (right) images demonstrate an enlarged posterior horn in the lateral ventricles (asterisks).
DO YOU CARE CORRECTLY FOR YOUR ULTRASOUND DEVICE?
Download your care guide now
Download PDF
Agenesis of the corpus callosum
The corpus callosum is an important commissure connecting the cerebral hemispheres. It is formed from the anterior to the posterior commissure, with the exception of the rostrum. Agenesis of the corpus callosum can be diagnosed using ultrasound. The diagnosis can be confirmed by indirect signs such as parallelism of the lateral ventricles, elevation of the third ventricle, dilatation of the occipital horn of the lateral ventricles, absence of gyri, and the presence of a Probst commissure that does not reach the contralateral hemisphere and subsequently bends, causing indentations on the anteromedial wall of the frontal horn (Fig. 4). Fetal MRI may also reveal other abnormalities of this system, including partial agenesis, dysgenesis, and hypoplasia. In addition, associated malformations involving supratentorial and infratentorial structures are common (80% of cases), and associated anomalies outside the central nervous system may occur, including congenital heart defects, skeletal defects, and genitourinary defects (60% of cases).
Figure 4:
Fetus with agenesis of the corpus callosum at 35 weeks. A. _ Axial ultrasound (left) and MRI (right) show an enlarged posterior horn of the lateral ventricle (asterisks). B. _ Coronal gray scale (left) and power Doppler (right) show absence of the cingulate gyrus and radial distribution of the gyrus (arrow). C. _ Sagittal T2-weighted magnetic resonance imaging also shows the same features as ultrasound. D. _ Axial tractography shows Probst's commissures (arrows).
Holoprosencephaly
Holoprosencephaly is a disease of early origin, observed even during brain organogenesis and resulting from a violation of the forebrain splitting. Based on severity, it is classified as alobar, semilobar, and dolobar, with specific imaging findings for each form. The incidence is approximately 1 in 10,000 births, and the prognosis of the alobar and semilobar forms is unfavorable.
Survival of mild forms is usually associated with mental retardation. Facial development is linked to brain development; consequently, facial defects ranging from mild hypotelorism to cyclopia may occur. Ultrasound is a very effective method for diagnosing alobar and semilobar holoprosencephaly.
Figure 5:
Fetus at 11 weeks with alobar holoprosencephaly. A. _ Axial ultrasound (left) demonstrates fusion of the thalamus and ventricles (asterisk), also shown in 3D rendering (right) with the proboscis (arrow). B. _ Anterior rendering (left) and HDLive (right) 3D ultrasound images of the face show the proboscis (arrow). C. _ A 3D ultrasound profile view in rendering (left) and HDLive (right) modes of a fetus shows the proboscis (arrow). D. _ Serial 3D ultrasound (tomographic ultrasound imaging) images show ventricular fusion (arrow). Axial (left), coronal (center), and sagittal (right) T2-weighted MR images show the monoventricle (asterisks) and fused cerebral hemispheres.
Hydroanencephaly
Hydranencephaly consists of complete or almost complete destruction of the cerebral cortex and basal ganglia. The etiology of this injury is controversial, and brain damage may be caused by vascular changes (complete and bilateral obstruction of the internal carotid arteries) or congenital infections (cytomegalovirus and toxoplasmosis). The vertebral artery system is relatively intact in hydranencephaly, resulting in significant sparing of the posterior fossa structures and the inferior and posterior portions of the temporal and occipital lobes. On MRI, despite the absence of the cerebral hemispheres, the brain stem, thalamus and cerebellum are present. The falx cerebri is also present, although sometimes reduced, with large amounts of fluid and necrotic debris over the immature thalamus and cerebellum (Fig. 6). When hydranencephaly is suspected, the differential diagnosis should include hydrocephalus and alobar and semilobar holoprosencephaly.
Figure 6:
Fetus with hydranencephaly at 22 weeks. A, B. Axial ultrasound (A) and 3-dimensional rendering ultrasound (B) demonstrate hydranencephaly (asterisks). C. _ Sagittal T2-weighted magnetic resonance imaging shows that the brain parenchyma forms a thin band with hydranencephaly (asterisks).
Microcephaly
Microcephaly is defined as a significant decrease in head circumference below the fifth percentile or two standard deviations below the mean. It is usually detected at 24 weeks because further diagnosis is easier at this stage due to the contrast between the size of the head and the body of the fetus. The main causes are autosomal recessive or dominant disorders, infections (cytomegalovirus, toxoplasmosis, rubella and Zika virus), radiation, drugs, alcohol and hypoxia.
Figure 7:
Microcephaly at 35 weeks after intrauterine Zika virus infection. A. _ Axial ultrasound shows parenchymal calcifications (arrow) and dilatation of the lateral ventricle (asterisk). Note that brain assessment is limited by shading artifact from the ossified skull. B. _ Axial T2-weighted magnetic resonance imaging shows a smooth and thin cortical band (arrow) and an enlarged ventricular system (asterisks). C. _ Sagittal T2-weighted magnetic resonance imaging shows ventricular enlargement (asterisk) and relative smoothness of the brain surface, brain atrophy, and heterogeneous cortex (arrow).
Chiari malformation
Chiari malformations are congenital anomalies of the hindbrain usually associated with hydrocephalus. Defect types I and II are the most common. Chiari I involves displacement of the cerebellar tonsils into the upper neck, while Chiari II involves herniation of the cerebellar vermis and fourth ventricle. Chiari II occurs in 65%-100% of cases of severe spina bifida. For this reason, when a Chiari II malformation is suspected, the possible presence of an associated meningomyelocele should be assessed. Chiari II findings on ultrasound include a small posterior fossa, hypoplastic cerebellar hemispheres, and ventricular dilatation.
Figure 8:
Fetus with Chiari II malformation at 26 weeks. A. _ Axial ultrasound shows evidence of cerebellar herniation (arrow). Axial ultrasound shows evidence of bilateral frontal skull depression and ventricular enlargement (asterisks). C, D. Sagittal (C) and axial (D) sonographic images demonstrate a meningocele (arrows). E. _ A meningocele (arrow) should be noted on 3-dimensional ultrasound rendering. F. Coronal T2-weighted magnetic resonance imaging shows a small posterior fossa, ventriculomegaly (asterisks), and obliteration of the cisterna magna (arrow). G. _ Axial T2-weighted magnetic resonance imaging shows ventricular enlargement (asterisks). H. Sagittal T2-weighted magnetic resonance imaging shows ventricular enlargement (asterisk) and cerebellar herniation (arrow). I. Axial (left) and sagittal (right) T2-weighted magnetic resonance imaging images show a meningocele (arrows). J. _
Three-dimensional reconstruction from magnetic resonance imaging shows a meningocele (arrow). There is another severe form of Chiari malformation known as type III. This form is rare and consists of an encephalocele with herniation of the contents of the posterior fossa (Fig. 9) and sometimes the occipital lobe. Tissue herniation is always abnormal, with areas of necrosis, gliosis, and fibrosis.
Figure 9.
Inencephaly
Inencephaly is a rare neural tube defect that occurs early in the embryonic development of the fetus (around the third week). It is characterized by severe retroflexion of the head due to a defect in the occipital region involving vertebral lesions. Vertebral changes are described in terms of the inability to visualize the posterior arches due to fusion with the anterior aspect of the vertebral body. The face is turned upward, the skin covers the areas of the lower jaw and chest. Associated anomalies are present in 84% of affected fetuses, including hydrocephalus, Dandy-Walker malformation, encephalocele, meningocele, diaphragmatic hernia, omphalocele, and cardiac and aortic arch anomalies. Findings obtained from ultrasound may indicate the diagnosis, but it is usually difficult to visualize the entire spine in the longitudinal plane using this technique, and details of the fetal brain and spinal cord may not be satisfactorily observed. MRI can delineate intracranial and intraspinal abnormalities in more detail (Figure 10).
Figure 10.
Fetus with inencephaly at 28 weeks. A, B. Sagittal ultrasound (left) and three-dimensional ultrasound rendering (right) (A) and sagittal T2-weighted magnetic resonance imaging (B) demonstrate a short cervical spine with marked retroflexion. Note hydrocephalus (asterisk) and dysraphism (arrow).
Dandy-Walker syndrome
Dandy-Walker malformation is a malformation of the posterior fossa with an incidence of 1 in 25,000 to 35,000 live births and a slight predominance in women. It is characterized by complete or partial agenesis of the cerebellar vermis, cystic dilatation of the fourth ventricle and enlargement of the posterior fossa, with superior displacement of the tentorium and fusion of the sinuses. Due to the late embryological development of the cerebellum, the diagnosis of agenesis or partial agenesis of the vermis cannot be suggested until the end of the 19th week, when the cerebellar vermis should be fully developed. Developmental defects are common, including agenesis of the corpus callosum (25%), lipoma of the corpus callosum, malformation of the gyrus, holoprosencephaly (25%), and cerebellar heterotopia (25%). In addition, the frequency of karyotypic disorders is high, mainly trisomies 18 and 13, as well as triploidy (up to 40% of cases).
Figure 11.
Fetus with Dandy-Walker malformation at 28 weeks. A. _ Axial ultrasound (left) and T2-weighted magnetic resonance imaging (right) demonstrate enlargement of the posterior fossa (asterisk). B. _ Sagittal T2-weighted magnetic resonance imaging shows a posterior fossa cyst (asterisk).
Ultrasound standards for first screening
The very first screening should be done from the 11th week of pregnancy to the 13th. It is during this period that the doctor prescribes an examination. Some expectant mothers can’t wait to go for an ultrasound before the 11th week. But there is no urgent need for this. After all, many indicators simply cannot be determined before this date. Therefore, the information content of the study will be small.
At the first screening, the doctor:
- reveals the exact duration of pregnancy;
- calculates the size of the fetus;
- looks at the uterus.
There are standards for each value. Let's look at them.
- The CTE or, more simply put, the length of the fetus is assessed. The norm is from 43 to 65 mm. When the deviation increases, it is believed that the baby will be born large. If it is to a lesser extent, then this indicates a slowdown in development, illness, or even the death of the fetus.
- The next indicator they look at is called BPR. The distance from one temple to another temple is measured. Normally it should be from 17 to 24 mm. Low scores may indicate developmental delays. High - about a large fetus (if other criteria also indicate this), or about hydrocephalus.
- Thickness of the collar space. The norm is 1.6-1.7 mm. If other numbers are revealed, then this is a bad sign, and we may be talking about Down syndrome.
- The length of the nasal bone should be from 2 to 4.2 mm.
- Heart rate. The norm is from 140 to 160 beats.
- Amnion. The norm of amniotic fluid is 50-100 ml.
- Cervical length. The norm is 35-40 mm.
Ultrasound diagnosis of hydrocephalus
The main symptom of the disease is an increase in the size of the head, caused by increased fluid pressure on the soft bones of the baby. The first and subsequent screenings show that the fetal head is too large.
When making a diagnosis, the doctor compares the size of the fetal head with normal ones. To do this, measure the dimensions of the head:
- Biparietal (BPR) - the distance between the temples along the line of the superciliary arches;
- Fronto-occipital (FOR) - the distance between the forehead and the back of the head.
An increase in both indicators indicates possible hydrocephalus. The more they deviate from the norm, the more severe the pathology. The data in the tables is considered approximate as it depends on the size of the fetus
| Duration in weeks | BPR, mm | LZR, mm |
| 10-11 | 13-17 | — |
| 12-13 | 21-24 | — |
| 14-15 | 27-31 | — |
| 16-17 | 34-38 | 45-50 |
| 18-19 | 42-45 | 54-58 |
| 20-21 | 48-51 | 62-66 |
| 22-23 | 54-58 | 70-74 |
| 24-25 | 61-64 | 78-81 |
| 26-27 | 67-70 | 85-88 |
| 28-29 | 73-76 | 91-94 |
| 30-31 | 78-80 | 97-101 |
| 32-33 | 82-84 | 104-107 |
| 34-35 | 86-88 | 110-112 |
| 36-37 | 90-92 | 114-116 |
| 38-40 | 94-96 | 118-120 |
Therefore, to identify hydrocephalus, the gynecologist simultaneously measures all other dimensions of the child. If they are also larger than normal, then the baby is simply large. With hydrocele of the brain, the development of the fetus often suffers, so its body and limbs are even smaller than necessary.
Measurements make it possible to differentiate hydrocephalus from a congenital increase in the size of the cerebral ventricles. Since these children do not have increased cerebral pressure, the head size may be normal. Sometimes it is even less than normal.
With hydrocephalus, the ventricles are filled with cerebrospinal fluid and are therefore deformed and enlarged. The size of their lateral walls, which is normally 7.5 mm, increases to 1 cm. The height of the ventricles increases by 0.2-0.3 mm. Incorrect development of other parts of the spinal cord and brain - the cisterna magna and the interhemispheric fissure - is often observed. At later stages, it is noticeable that the baby’s brain convolutions are flattened, the furrows are smoothed, and the vessels and membranes are incorrectly formed.
Ultrasound standards for second screening
At 16-20 weeks, a second screening is done. In addition to the size, the doctor looks at how the fetus is positioned and the condition of the fetal organs.
Ultrasound standards look like this:
- BPR - 26–56 mm.
- The length of the femur bone is 13–38 mm.
- The length of the humerus bone is 13–36 mm.
- Exhaust gas - 112–186 mm
- Water levels are 73–230 mm. If oligohydramnios is detected, this negatively affects the formation of the baby’s nervous system.
In addition to the above, the doctor looks at the location of the placenta. If it is located on the anterior wall of the uterus, then there is a risk of detachment.
Another important indicator that the doctor pays attention to is the location of the umbilical cord attachment.
Ultrasound screening in Moscow in a paid clinic
Screening is a very important examination that must be completed. Diseases that can be found using this diagnostic method can save your baby's life.
It is most convenient for this study to go to a private clinic. A pregnant woman is prone to frequent mood swings and fatigue. In a private clinic, you don’t have to sit in line for a long time, there is no need to swear for any reason. On the contrary, it is possible to make an appointment at a convenient time and day, friendly staff. The doctor will carry out the procedure more carefully and carefully, and if desired, take a photo of the fetus and a video of the procedure. In addition, there is always the opportunity to send screening results to your email.