Stiff person syndrome (SPS) is a rare neurological disorder characterized by progressive muscle stiffness and painful muscle spasms. The term HRF was first introduced in 1956 by American neurologists F. Moersch and H. Wbltman, who presented a description of patients with a previously unknown disease, which was characterized by “progressive fluctuating muscle rigidity and spasms in the axial muscles” [1, 2]. The etiology and pathogenesis of this disease remain not fully understood; an autoimmune mechanism of the disease is assumed. In HRF, the GABAergic descending system is relatively selectively affected, leading to an imbalance between the noradrenergic and GABAergic descending systems [1, 2]. The basis of the clinical manifestations of this syndrome are: pain and tension in the muscles of the back, abdomen, and neck; the predominance of high muscle tone in the extensors of the limbs, constant tension of the paravertebral muscles, abdominal muscles and muscle spasms (see table)
Diagnostic criteria for HRF with modifications [3-5] [1].
Along with the classical variants of HRF, the literature describes cases of its combination with other neurological symptoms, including cerebellar and oculomotor disorders, and severe autonomic dysfunction, which expands the understanding of the clinical manifestations of HRF [2, 6]. We present our own observation of SRF with features of the clinical course.
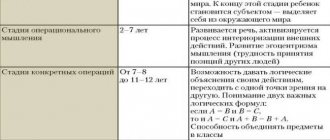
Cognitive rigidity
This is inertia of thinking, lack of flexibility in adjusting the order of actions in the face of changed external circumstances. It is very difficult for people of this type to use a familiar object for an unfamiliar action. For them, this thing is associated only with its traditional purpose.
In everyday life, the cognitive type of rigidity is expressed in the fact that a person has difficulty assimilating and using new information, learning material and practical skills. New technologies are difficult for him to master and use, even if they greatly facilitate his work or improve his living conditions.
Temperament types
Description of the characteristics of various temperaments
can help to understand the traits of a person’s temperament if they are clearly expressed, but people with clearly expressed traits of a certain temperament are not very common; most often people have mixed temperament in various combinations. But the predominance of traits of any type of temperament makes it possible to classify a person’s temperament as one or another type.
Melancholic
A person is easily vulnerable, prone to constantly experiencing various events, he reacts little to external factors. He cannot restrain his asthenic experiences by force of will; he is highly impressionable and easily emotionally vulnerable. These traits are emotional weakness.
Phlegmatic person
Slow, calm, has stable aspirations and mood, outwardly stingy in the manifestation of emotions and feelings. He shows perseverance and perseverance in his work, remaining calm and balanced. He is productive at work, compensating for his slowness with diligence.
Sanguine
A lively, hot-tempered, active person, with frequent changes of mood and impressions, with a quick reaction to all the events happening around him, quite easily coming to terms with his failures and troubles. He is very productive at work when he is interested, becoming very excited about it; if the work is not interesting, he is indifferent to it, he becomes bored.
Choleric
Fast, passionate, impetuous, but completely unbalanced, with sharply changing moods with emotional outbursts, quickly exhausted. He does not have a balance of nervous processes, this sharply distinguishes him from a sanguine person. A choleric person, getting carried away, carelessly wastes his strength and quickly becomes exhausted.
Affective rigidity
This is the inertia of thinking regarding the establishment of a connection between events and certain affective reactions. In other words, a person is not able to connect real events with fantasy. This hinders him from identifying and solving real problems.
A person with affective rigidity focuses excessively on some object or situation. At the same time, the overpowering feelings excessively influence a person’s behavior. In this case, the previous experience of experienced experiences is included. As a result, a person acts according to a previously proven algorithm.
Character traits
People belonging to this type of personality are distinguished by suspicion towards others and distrust. Afraid of being deceived, they always and everywhere try to be careful.
A person with a rigid type of higher nervous activity always has high self-esteem.
He does not acknowledge criticism addressed to him - it irritates him. He himself is also unable to evaluate himself objectively. At the same time, he can quite harshly express his opinion about others.
Jokes towards a person with a rigid type of nervous activity can cause in him a feeling of resentment, the confidence that he is unfairly underestimated. This often leads to conflict situations. Such people are not able to give up their beliefs, even if they are wrong. This is the most difficult personality type in terms of behavior in a conflict situation.
When faced with such a person, you should carefully select the topic for conversation and speak out, weighing every word. In a controversial situation, it is better to remain silent and leave without heating up the relationship.
Rigid individuals are staunch conservatives. But you can find some advantages in this. Such people make excellent mathematicians, accountants, economists and representatives of other exact sciences and professions. If this feature is expressed moderately, then from a disadvantage it turns into an advantage. Such a person adheres to his position in life, he is characterized by pedantry and accuracy, which is often valued in people.
Rigid personalities prefer specifics. They are more resistant to stressful situations and external stimuli. If a person is intellectually developed, he can “infect” others with his idea. This contributes to the rapid acquisition of leadership positions.
If rigidity is highly developed, it can give rise to paranoid tendencies. It is very difficult to restrain and direct such people in the right direction. Only a qualified psychologist can help.
Table
Melancholic temperament
, as can be seen from the table, is determined by the weakness of the processes of excitation and inhibition, while their mobility or inertia is uncharacteristic. Even with a slight overstrain, for example, in the case of solving a difficult task or life situation, a melancholic person has a breakdown.
A melancholic person has a weak type of nervous system and, therefore, is not resistant to circumstances that require overcoming or strong stimulation of the nervous system. The remaining three types of nervous system are considered strong.
Phlegmatic temperaments
, is called a type of temperament that, although a strong type, is still characterized by low mobility of nervous processes. Once arising in certain centers, they are distinguished by constancy and strength. An inert nervous system corresponds to this type.
Sanguine temperament
- another strong type of temperament - is characterized by the fact that the processes of excitation and inhibition are quite strong, balanced and easily mobile.
Choleric temperament
- the third strong type of temperament
is
unbalanced, unrestrained, in it the processes of excitation prevail over weak inhibition. This type of nervous system quickly depletes and is prone to breakdowns.
If on a diagram we place all the temperaments in a coordinate system, at the starting point of which is the sanguine person (strong, balanced, agile), then other temperaments deviate from it depending on the severity of the features of the three coordinates such as the nervous system, characteristic of these temperaments.
Diagram of the dependence of temperament on the coordinates of the type of nervous system
Why cannot the concepts of temperament and type of nervous system be identified?
Temperament is a psychological concept, and the type of nervous system is physiological.
Causes
A rigid personality type, as a rule, is formed in childhood or at the stage of growing up. Parents are often to blame for this. The reason is their increased demands on the child and distrust of his actions, especially if this is expressed in an aggressive form.
Constant fear for the correctness of the results of one’s actions necessitates constant recognition of one’s importance. The child begins to strive for absolute leadership; a desire arises to always be the first, the best, and irreplaceable.
Rigid individuals, talking about their childhood, often claim that their relationship with their parents was normal, even friendly to some extent. But it was superficial communication without mutual expression of feelings.
Experiencing injustice towards himself, such a child tries to get rid of his worries. For this purpose, he puts on a protective mask of composure - rigidity. A person of this type appears insensitive, convincing himself that nothing concerns him. In fact, these are very vulnerable people who hide their emotional experiences from others.
Already in childhood, such a child notices that he is valued more for his actions, and not for his essence. He is sure of this, even if it is a mistaken opinion. For this reason, he becomes diligent and hardworking. A rigid person always solves all his problems himself. He seeks help in the most extreme cases. Does not like to talk about his troubles to others.
A rigid person loves punctuality, but he himself is prone to being late, since his preparations are often delayed. Being confident that the boss is always right, he is afraid of authoritative people.
Since a rigid person is always confident that he is right and honest, he perceives any doubt about this as an insult. He is prone to exaggeration, is too demanding of himself and is afraid to make mistakes.
External signs
A rigid personality is distinguished by the habits characteristic of this type. These people often cross their arms over their chest, as they intuitively try to close the solar plexus area so as not to succumb to feelings. They have a preference for dark shades of clothing, their favorite color is black. They prefer styles that fit the waist, again trying to squeeze the solar plexus area.
A rigid person always maintains his posture. He has a proportionate physique, even if over time he becomes overweight, the acquisition of which he is more afraid of than all other people. His shoulders are always straight and his neck is proudly stretched out.
Rigid individuals have liveliness of character and mobility. However, they are not flexible enough. The look of such people is lively and open.
If you notice similar external signs in yourself, as well as behavior and communication, you cannot leave the problem unattended. In order to avoid worsening your condition, it is recommended to seek help from a psychologist.
Clinical case
Patient T.
, 23 years old, was sent to the regional clinical hospital of Krasnoyarsk with complaints of severe progressive stiffness and painful spasms of the muscles of the back, neck, chest, abdomen, shoulder girdle with significant limitation of spinal mobility, difficulty in performing movements, walking (slowing down and shortening the step) and self-care , limitation of free speech due to stiffness in the articulatory muscles, general weakness, difficulty swallowing food (especially solid), loss of body weight by 10 kg over 3 months. The patient also noted increased stiffness of the trunk muscles with excitement, sudden stimuli (loud sound, fear, etc.) and a decrease during sleep.
From the anamnesis it is known that in childhood he grew and developed without any special features. A vegetarian since childhood, over the last year he began to eat meat. At the age of 16, she was diagnosed with thoracic kyphoscoliosis and was bothered by moderate pain in the back. The development of the present disease occurred over the course of a year; moderate stiffness and soreness appeared in the muscles of the trunk, which was associated with stress. Next, muscle stiffness, slower walking, and difficulty performing physical work progressed. After 3 months, he began to notice choking on dry food and a decrease in body weight. The patient's above-mentioned complaints progressed steadily, muscle stiffness increased and other symptoms became much more pronounced.
Hereditary history is not burdened.
Neurological status upon examination: walking independently, oligobradykinesia noted. The patient is hypomimic and does not sit down during examination (he notes increased contraction in the back muscles when sitting). Oriented, adequate, mild dysarthria in speech, answers questions in short phrases, lacks speech initiative. Needs help in everyday life and with self-care (difficulty getting dressed, getting a mug from the shelf, washing, etc.). Memory within normal limits, decreased attention. Palpebral fissures D=S, pupils D=S, eyeball movements in full, no nystagmus, no diplopia. Trigeminal points are painless, sensitivity on the face is not impaired. The nasolabial folds are somewhat asymmetrical. The tongue is in the midline, the tone of the tongue is slightly increased. The soft palate is mobile, the uvula is in the midline, the pharyngeal reflex is preserved. Dysphagia when eating dry food. Tension of the neck and oromandibular muscles, limitation of rotation and tilt of the head. Severe kyphoscoliosis in the thoracolumbar region, limitation of movements in all parts of the spine. Severe tension in the muscles of the abdomen, back, and neck (Fig. 1).
Rice. 1. View of patient T. (a) from the front and (b) from the side. The paravertebral muscles in the area of scoliosis are moderately painful on palpation. Stiffness in the muscles of the arms and legs. Limitation of the range of active movements in the upper limbs to chest level. Muscle strength in the limbs is sufficient in all segments, tendon reflexes D=S. There are no pathological signs. No sensory disturbances were detected. Coordinator tests are performed satisfactorily. There are no meningeal signs. Pelvic functions are not impaired. Signs of autonomic dysfunction: bright diffuse dermographism, hyperhidrosis of the palms and feet.
The patient underwent further examination by a geneticist at the regional medical genetic center; there was no evidence of lysosomal storage diseases.
According to magnetic resonance imaging of the brain, there were signs of moderate external hydrocephalus, minimal ectopia of the right cerebellar tonsil; multislice computed tomography (MSCT) of the chest, abdominal organs, ultrasound examination (ultrasound) of the abdominal organs - without pathology; esophagogastroscopy - gastric erosion, ultrasound of the thyroid gland - without pathology.
A complete blood count, biochemical blood test, general urine test, rheumatological tests, creatine phosphokinase were within normal limits for the entire observation period. Blood test for thyroid hormones (total T3 - 1.17 nmol/l, total T4 - 100.53 nmol/l, TSH - 2.49 mU/l) - within normal limits. Analysis for tumor markers: alpha-fetoprotein - 3.55 IU/ml (normal), cancer embryonal antigen - 2.9 ng/ml (normal). Needle electromyography (EMG) was performed: spontaneous EMG recorded constant motor activity of muscle units and spontaneous activity in the form of fibrillations, fasciculations and single positive sharp waves. In the trapezius muscles, the motor unit potential is normal. Consulted with related specialists (nephrologist, orthopedist, neuropsychologist, psychiatrist, ophthalmologist, ENT doctor, urologist, gastroenterologist), data regarding ankylosing spondylitis, cancer, systemic connective tissue disease, psychiatric and other pathologies have not been established.
A blood test was performed for antibodies to GAD (glutamate decarboxylase), and an elevated level was recorded - 32.70 U/ml (normal value is less than 10 U/ml).
Considering the gradual onset of the disease with muscle tension, painful spasms, slow progression, difficulty walking, dysphagia, autonomic dysfunction, the absence of cognitive impairment and other somatic and neurological pathology, confirmed by electromyographic data, the presence of antibodies to antigens of GABAergic neurons, the diagnosis “G25” was made .8 Other specified extrapyramidal and movement disorders. SRF with severe rigidity, dysphagia, dysarthria, autonomic dysfunction, skeletal deformities in the form of severe kyphoscoliosis, moderately progressive course, stage of incomplete stabilization.” The patient was consulted in absentia at the Federal State Budgetary Institution "Scientific Center of Neurology". Taking into account the results of the comprehensive examination, the most likely pathogenesis of the disease was autoimmune.
The patient was hospitalized in the neurological department for immunosuppressive treatment and selection of further therapy. During hospitalization, gastroscopy revealed erosive lesions of the stomach, which was a contraindication for pulse therapy with methylprednisolone. A course of treatment with intravenous human immunoglobulin (Octagam 5%) was carried out at a dose of 0.4 g/kg/day for 5 days; baclofen was added as additional therapy at a dose of 10 mg 3 times a day, valproic acid 600 mg per day (for the purpose of stimulation of GABA transmission). During treatment, dynamics were noted in the form of a decrease in muscle stiffness, an increase in the range of movements in the cervical spine, a decrease in speech disorders and dysphagia. The patient was recommended to take cyclosporine at an initial dose of 50 mg/day, which the patient refused to increase further. After treatment for 3 months, the patient's condition stabilized, he became more active, rigidity decreased, speech activity improved, and he swallows freely. During a routine examination, therapy was adjusted: valproic acid was replaced with levetiracetam at a dose of 500 mg/day, diazepam was added at a dose of 10 mg/day, baclofen 30 mg/day, and further use of cyclosporine was stopped, and the patient refused. During a six-month follow-up, the patient's condition remained stable.
The disease further progressed in March 2021, when stiffness in the muscles of the shoulder girdle and neck began to increase, and swelling of the feet appeared, which were regarded as a side effect of taking levetiracetam. The drug was discontinued, but the swelling of the feet did not regress. In April 2021, paresis of the left arm was added to the clinical symptoms, which developed acutely during a meal when the arm was suspended (Fig. 2).
Rice. 2. Patient T. Peripheral monoparesis on the left. An emergency medical team was called, the patient with suspected acute cerebrovascular accident was taken to the hospital, examined, a dynamic MSCT of the brain was performed - without pathology, a stroke was excluded. During the examination, progression of kyphoscoliosis was noted, peripheral paresis of the proximal (3-3.5 points) and distal (1.5-2 points) parts of the left upper limb was detected with loss of reflexes, absence of pain, and the presence of vegetative-trophic disorders in the form of edema of the left hand , painful upper monohypesthesia of the left arm. Palpation revealed pronounced rigidity of the paravertebral muscles and neck muscles; trigger points were identified in the muscles of the neck and shoulder girdle on the left. According to the results of electroneuromyography (ENMG), a slight decrease in the speed of impulse conduction is recorded during antidromic stimulation of the sensory endings of the median and ulnar nerves on the left. The dynamics revealed an increase in the titer of antibodies to GAD - 101.50 U/ml.
The acute occurrence of brachioplexopathy on the left when performing arm movements against the background of severe muscle rigidity in the neck and shoulder girdle was probably due to the compression-ischemic factor in combination with dysimmune mechanisms. The latter is supported by an increase in the titer of anti-GAD antibodies, accompanied by a deepening of previously existing and the emergence of new clinical manifestations of the disease. In addition, upon examination, the patient had swelling of the feet (Fig. 3),
Rice. 3. Patient T. Swelling of the feet. painful hypoesthesia of the “sock” type, loss of Achilles reflexes on both sides. According to ENMG data, a decrease in the speed of impulse conduction was recorded during antidromic stimulation of the sensory endings of the sural and superficial peroneal nerves on both sides. Thus, along with plexopathy, the patient was diagnosed with damage to another part of the peripheral nervous system in the form of distal sensory-vegetative polyneuropathy of the lower extremities. The lack of data on the paraneoplastic process suggests that the most likely cause of the development of polyneuropathy in the observed patient is an autoimmune mechanism. In addition, given the patient's low body weight, it is possible to assume metabolic damage to the nerves of the lower extremities.
Taking into account the progression of neurological symptoms, an increase in the titer of antibodies to GAD, and the absence of changes in esophagogastroscopy, a course of pulse therapy with methylprednisolone was administered at a dose of 1000 mg 5 times. The patient was consulted by a physical therapy doctor, physical therapy was selected, and Trental and neurometabolic therapy (thioctic acid, Keltican complex) were added to the therapy. The patient was discharged in a stable condition, however, no significant changes in symptoms of damage to the peripheral nervous system were noted.