Ischemic stroke is a pathological condition that is not a separate or independent disease, but an episode that develops as part of a progressive general or local vascular lesion in various diseases of the cardiovascular system. Often, ischemic stroke is accompanied by the following diseases: arterial hypertension, atherosclerosis, rheumatic heart disease, coronary heart disease, diabetes mellitus and other forms of pathology with vascular damage. The clinical picture of ischemic stroke consists of general cerebral and focal symptoms, depending on the location of vascular disorders. The most important method for instrumental diagnosis of ischemic stroke, as well as its differentiation from hemorrhagic stroke, is CT and MRI of the brain.
ICD-10
I63 Cerebral infarction
- Causes
- Pathogenesis
- Classification
- Symptoms of ischemic stroke Brain infarction in the MCA basin
- Cerebral infarction in the ACA basin
- Cerebral infarction in the PCA basin
- Cerebral infarction in the vertebrobasilar region
- Differential diagnosis
- Therapy in the acute period
Hemodynamic stroke
Hemodynamic ischemic stroke is an ischemic stroke caused by changes in pressure in the vessels and prolonged vascular spasm, which occurs with arterial hypertension, general prolonged hypotension, hypovolemia (possibly due to blood loss) and is observed in areas with a depleted vascular component located in areas of mixed blood supply: in frontal lobe, temporoparietal region and centrum semiovale.
Infarction in the subcortical border zone
Fig. 23 There is a lesion area in the paraventricular white matter and the centrum semiovale on the right, which has an increased MR signal on T2 and Flair (arrows) - ischemic stroke.
Fig. 24 In the semi-oval center on the right and subcortically, an area of a cloud-like structure is identified, located in the semi-oval center and subcortically, having an increased MR signal on T2, Flair and DWI - an area of ischemic infarction.
Infarction in the anterior border zone
Fig. 25 There is an ischemic lesion in the white matter and paraventricularly in the frontal lobe on the left, which has an increased MR signal in T2, Flair and a decreased signal in T1 (arrows).
Infarction in the posterior border zone
Fig. 26 In the paraventricular white matter and subcortically in the left parietal lobe there is a small area of ischemic stroke with an increased MR signal on T2, Flair and DWI.
Fig. 27 CT scan shows areas of long-term consequences of ischemic stroke in the form of zones of cystic-gliotic changes (arrows), located in the subcortical white matter and the previously existing cortex in the frontal lobes and parietal lobes - at the boundaries of the mixed circulation (intersection of the right MCA and PCA basins) .
Causes
Since ischemic stroke is not considered as a separate disease, it is impossible to determine a single etiological factor for it. However, there are risk factors associated with an increased incidence of ischemic stroke, which can be divided into two groups:
1. Modifiable.
- myocardial infarction
- arterial hypertension
- atrial fibrillation
- diabetes
- dyslipoproteinemia
- asymptomatic lesions of the carotid arteries.
2. Unmodifiable.
- hereditary predisposition
- age
In addition, there are risk factors associated with lifestyle: low level of physical activity, acute stress or prolonged psycho-emotional stress, excess body weight, smoking.
Short description
The middle cerebral artery (ICD-10 code - I63.0 - I63.8) is the largest branch of the internal carotid artery. It is divided into the left and right MCA and serves as the source of blood supply to the cerebrum, insula and cortex. Since the SMA is part of the circle of Willis, blood flow in the areas supplied by it does not occur through this circle, but through the cortical and meningeal branches.
The incidence rate of this type of pathology is small. Middle cerebral artery stroke is diagnosed in 3% of all cases.
Pathogenesis
A certain sequence of molecular biochemical changes in the brain substance, caused by acute focal cerebral ischemia, can lead to tissue damage, resulting in cell death (cerebral infarction). The nature of the changes depends on the level of decrease in cerebral blood flow, the duration of this decrease and the sensitivity of the brain substance to ischemia. The degree of reversibility of tissue changes at each stage of the pathological process is determined by the level of decrease in cerebral blood flow and its duration in combination with factors that determine the sensitivity of the brain to hypoxic damage.
The term “infarction core” refers to a zone of irreversible damage, and the term “ischemic penumbra” (penumbra) refers to a zone of reversible ischemic damage. The duration of the penumbra's existence is the most important point, since over time, reversible changes become irreversible. The oligemic zone is a zone in which a balance is maintained between tissue needs and the processes that provide these needs, despite the decrease in cerebral blood flow. It is capable of existing for an indefinitely long time without passing into the core of the infarction, therefore it is not classified as a penumbra.
Therapy
If the victim is not provided with medical assistance within 2.5 hours, irreversible changes in the brain will occur. For treatment use:
- Medicines to lower blood pressure.
- Medicines to eliminate thrombosis.
- Diuretics.
In some cases, surgery is performed, including embolectomy, as well as stenting of the arteries that are affected.
Classification
Ischemic stroke can be a consequence of one or another disease of the cardiovascular system. There are several pathogenetic variants of ischemic stroke. The TOAST (Trial of Org 10172 in Acute Stroke Treatment) classification, which is most widely used, distinguishes the following types of ischemic stroke:
- cardioembolic - ischemic stroke caused by arrhythmia, valvular heart disease, myocardial infarction;
- atherothrombotic - ischemic stroke that occurred due to atherosclerosis of the large arteries, which resulted in arterio-arterial embolism;
- lacunar - ischemic stroke caused by occlusion of small arteries;
- ischemic stroke associated with other, more rare causes: blood hypercoagulation, arterial wall dissection, non-atherosclerotic vasculopathies;
- ischemic stroke of unknown origin - a stroke with an unknown cause or with the presence of two or more possible causes, when it is not possible to establish an accurate diagnosis.
In addition, a minor stroke is distinguished when the existing symptoms regress during the first three weeks of the disease.
There are also several periods of ischemic stroke:
- The most acute period is the first 3 days. Of these, the first three hours were defined as a “therapeutic window”, when it is possible to use thrombolytic drugs for systemic administration. In case of regression of symptoms during the first day, a transient ischemic attack is diagnosed;
- acute period - up to 4 weeks;
- early recovery period - up to six months;
- late recovery period - up to 2 years;
- period of residual effects - after 2 years.
Cardioembolic stroke
Cardioembolic ischemic stroke occurs when an artery is occluded by an embolus, which most often occurs on the heart valves due to the development of inflammation, infection, or increased blood clotting. There may also be embolism with particles of atherosclerotic plaque from the carotid artery and very rarely air or fat embolism. Morphologically it is difficult to distinguish between a heart attack caused by atherothrombosis or embolism. With the cardioembolic mechanism, a hemorrhagic infarction occurs much more often, caused by lysis of the thrombus and the relatively “rapid” restoration of blood flow in the nervous tissue that has already died from ischemia. Clinically, such a stroke is manifested by a sharp deterioration and development of focal neurological symptoms against the background of complete well-being during vigorous activity.
Symptoms of ischemic stroke
The clinical symptom complex of ischemic stroke is varied and depends on the location and volume of the brain lesion. The most common localization of the lesion is in the carotid region (up to 85%), less often in the vertebral-basilar region.
Cerebral infarction in the MCA basin
A feature of a heart attack in the blood supply of the middle cerebral artery is the presence of a pronounced collateral blood supply system. Occlusion of the proximal middle cerebral artery can cause a subcortical infarction, while the cortical area of the blood supply remains unaffected. In the absence of these collaterals, an extensive infarction may develop in the area of the blood supply to the middle cerebral artery.
For a heart attack in the area of blood supply to the superficial branches of the middle cerebral artery, deviation of the eyeballs and head towards the affected hemisphere is typical. In this case, in case of damage to the dominant hemisphere, ipsilateral ideomotor apraxia and total aphasia develop, and in case of damage to the subdominant hemisphere, anosognosia, dysarthria, aprosody and contralateral neglect of space develop.
The main clinical manifestation of cerebral infarction in the region of the branches of the middle cerebral artery is contralateral hemiparesis and contralateral hemianesthesia. In the case of extensive lesions, concomitant abduction of the eyeballs and gaze fixation towards the affected hemisphere may occur. With infarctions of the subdominant hemisphere, emotional disturbances and spatial neglect develop.
The spread of paresis during a heart attack in the blood supply of the striatocapsular arteries depends on the location and size of the lesion (upper limb, face or the entire contralateral part of the body). In the case of extensive striatocapsular infarction, typical manifestations of middle cerebral artery occlusion (aphasia, homonymous lateral hemianopia) usually develop. Lacunar infarction is clinically manifested by the development of lacunar syndromes (isolated hemiparesis and hemihypesthesia or their combination).
Cerebral infarction in the ACA basin
The most common clinical manifestation of a heart attack in the blood supply of the anterior cerebral artery is motor disturbances. In most cases of occlusion of the cortical branches, motor deficits develop in the foot and entire lower limb, as well as mild paresis of the upper limb with extensive damage to the tongue and face.
Cerebral infarction in the PCA basin
As a result of occlusion of the posterior cerebral artery, infarctions of the occipital temporal lobe, as well as the mediobasal parts of the temporal lobe, develop. In such cases, clinical manifestations are visual field defects (contralateral homonymous hemianopsia). It is also possible that they may be combined with visual hallucinations and photopsia.
Cerebral infarction in the vertebrobasilar region
Stroke in the vertebrobasilar blood supply occurs as a result of occlusion of the only perforating branch of the basilar artery and is usually accompanied by symptoms of damage to the cranial nerves on the ipsilateral side. Occlusion of the vertebral artery or its main penetrating branches arising from the distal parts leads to the development of Wallenberg syndrome (lateral medullary syndrome).
Ischemic stroke in the posterior cerebral arteries: problems of diagnosis and treatment
I.A. KHASANOV, E.I. BOGDANOV
Republican Clinical Hospital of the Ministry of Health of the Republic of Tatarstan, Kazan
Kazan State Medical University
Khasanov Ildar Akramovich
doctor of the neurological department for patients with acute cerebrovascular accidents
420064, Kazan, st. Orenburgsky Trakt, 138, tel. (843) 237-35-47, e-mail
In the light of modern data, the article examines the problems of diagnosis and treatment of ischemic strokes in the posterior cerebral arteries (PCA), taking into account the characteristics of their etiology, clinical picture and neuroimaging data. The paired posterior cerebral arteries, formed by the bifurcation of the basilar artery and being its terminal branches, serve as the main sources of blood supply to the upper part of the midbrain, the thalami and the posteroinferior parts of the cerebral hemispheres, including the occipital lobes, the mediobasal parts of the temporal lobes and the inferomedial parts of the vertex. Ischemic strokes in the posterior cerebral artery basin account, according to various sources, from 5-10 to 25% of cases of all ischemic strokes. The most common cause of isolated infarctions in the PCA territory is embolic occlusion of the PCA and its branches, which occurs in approximately 82% of cases. In 9% of cases, thrombosis in situ is detected in the PCA; in another 9% of cases, the cause of stroke is vasoconstriction associated with migraine and coagulopathy. A very rare cause of infarction in this region can also be arterial dissection affecting the PCA. The most common and characteristic signs of infarctions in the PCA region are visual disturbances (homonymous hemianopsia), central paresis of the facial nerve, headache, sensory disturbances, aphasic disorders, hemiparesis and nigility.
Key words:
ischemic stroke, cerebral infarction, posterior cerebral artery, neuroimaging, thrombolytic therapy
I.A. KHASANOV, EI BOGDANOV
Kazan State Medical University
Republican Clinical Hospital of the Ministry of Health of the Republic of Tatarstan, Kazan
Ischemic stroke in a system of posterior cerebral arteries: problems of diagnosis and treatment
In the article on the basis of present knowledge are considered the problems of diagnosis and treatment of ischemic strokes in a system of posterior cerebral arteries (PCA) taking into account their causation, clinical presentation and neuroimaging data. Paired posterior cerebral arteries, which are shaped by basilar artery bifurcation and are its terminal branches, are the main sources of blood supply of the upside of midbrain, thalamus and back and bottom parts of cerebral hemispheres, including occipital lobes, mediobasal branches of temporal lobes and lower medial crown branches. Ischemic strokes in a system of posterior cerebral arteries amount to 5-10% or up to 25% of all ischemic strokes. The most common cause of isolated heart attacks
in a system of PCA is the embolic occlusion of PCA and its branches, which occurs in about 82% of cases. In 9% of cases in PCA is revealed thrombosis, in other 9% of cases the cause of stroke are vasoconstriction associated with migraine, and coagulopathy. A very rarely reason for a heart attack in this system can be artery dissection which affects the PCA. The most frequent and characteristic features of heart attacks in a system of PCA are visual impairments (equilateral hemianopsia), central paresis of facial nerve, headache, sensation disorders, aphatic disorders, hemiparesis and neglect.
Key words:
ischemic stroke, cerebrovascular accident, posterior cerebral artery, neuroimaging, thrombolytic therapy.
Ischemic strokes in the posterior cerebral arteries (PCA) account, according to various sources, from 5-10 to 25% of cases of all ischemic strokes [1-4]. They can be the cause of a number of clinical symptoms, which are not always promptly and adequately recognized by the patients themselves, their relatives and doctors, because an acute gross motor deficit, which is usually associated with a stroke, in this case may be unexpressed or completely absent. A delay in timely diagnosis or incorrect diagnosis casts doubt on the possibility of providing the patient with adequate therapy (primarily thrombolysis), which in turn cannot but affect the outcome of the disease [5]. An important role in making a diagnosis is played by the possibility of using neuroimaging, the correct choice of method and competent interpretation of the results [2]. It seems important to present and analyze the features of the clinical picture, neuroimaging and treatment of ischemic strokes in the posterior cerebral arteries in the light of modern data.
The most common cause of isolated infarctions in the PCA territory is embolic occlusion of the PCA and its branches, which occurs in 82% of cases. At the same time, cardiogenic genesis is observed in 41% of cases, while arterio-arterial embolism from the vertebral and basilar arteries is observed in only 32% of cases. In 10% of patients, the source of the embolism cannot be determined. In 9% of cases, thrombosis in situ is detected in the PCA. Vasoconstriction associated with migraine and coagulopathies are the causes of cerebral infarction in 9% of cases [6]. If isolated infarctions in the PCA territory in most cases are of a cardioembolic nature, then involvement of the brainstem and/or cerebellum in combination with an infarction in the PCA territory is most often associated with atherosclerotic lesions of the vessels of the vertebrobasilar system [7, 8]. A very rare cause of infarction in this region can also be arterial dissection affecting the PCA [9]. Regardless of the cause of the infarction, it usually only partially involves the PCA territory [10, 11].
Paired posterior cerebral arteries, formed by the bifurcation of the basilar artery and being its terminal branches, serve as the main sources of blood supply to the upper part of the midbrain, thalamus and posteroinferior parts of the cerebral hemispheres, including the occipital lobes, mediobasal parts of the temporal lobes and inferomedial parts of the vertex [10, 12, 13].
In the early stages of development of the human body, the posterior cerebral artery is a branch of the internal carotid artery (ICA) and is supplied with blood from the carotid system, while the posterior communicating artery (PCA) plays the role of its proximal segment. Subsequently, blood begins to flow into the posterior cerebral arteries from the main artery, and the PCA, being a branch of the internal carotid artery, becomes the most significant anastomosis between the carotid and vertebrobasilar areas. According to various sources, from 17 to 30% of adults have a fetal (embryonic) type of PCA structure, in which the ICA remains the main source of blood supply to the PCA throughout life. The fetal type of PCA structure is in most cases observed unilaterally, with the opposite PCA usually starting from an asymmetrically located, curved basilar artery. In cases where both posterior cerebral arteries are branches of the internal carotid arteries, as a rule, well-developed large posterior communicating arteries are observed, and the superior segment of the basilar artery is shorter than usual (the basilar artery ends with the two superior cerebellar arteries arising from it). In approximately 8% of cases, both PCAs originate from the same ICA [7, 8, 12, 14, 15].
The PCA joins the PCA approximately 10 mm distal to the bifurcation of the basilar artery. Each PCA can be conditionally divided into 3 parts: the precommunication part, or P1 segment according to Fisher, - the section of the PCA proximal to the place where the PCA flows into it, the postcommunication part, or P2 segment, located distal to the place where the PCA flows into the PCA, and the final (cortical) the part that gives off branches to the corresponding areas of the cerebral cortex [12, 16]. The paramedian mesencephalic, posterior thalamoperforating and medial posterior choroidal arteries depart from the precommunicative part, participating primarily in the blood supply to the ventrolateral nuclei of the thalamus and the medial geniculate body. The left and right posterior thalamoperforating arteries may arise from a common trunk called the artery of Percheron; a similar variant of the structure usually occurs in combination with unilateral hypoplasia of the P1 segment and the fetal structure of the PCA. The branches of the postcommunication part are the peduncular perforator, thalamogeniculate and lateral posterior choroidal arteries, supplying the lateral geniculate body, dorsomedial nuclei and thalamic cushion, part of the midbrain and the lateral wall of the lateral ventricle [2, 12, 17]. The main cortical branches of the PCA are the anterior and posterior temporal, parietotemporal and calcarine arteries [10]. The boundaries of the watershed of the middle and posterior cerebral arteries basins fluctuate significantly. Usually the border of the PCA basin is the Sylvian fissure, but sometimes the middle cerebral artery supplies blood to the outer parts of the occipital lobe up to the occipital pole. At the same time, the PCA always supplies blood to areas of the cerebral cortex in the area of the calcarine sulcus, and the optic radiation in some cases receives blood from the middle cerebral artery; accordingly, homonymous hemianopsia does not always imply a heart attack in the PCA territory [12].
With ischemic strokes in the PCA region, depending on the location of the vessel occlusion, as well as on the state of collateral blood supply, the clinical picture may reveal symptoms of damage to the midbrain, thalamus and cerebral hemispheres. In general, up to 2/3 of all infarctions in the PCA territory are cortical, the thalamus is involved only in 20-30% of cases, and the midbrain in less than 10% of cases [7, 18, 19]. Accordingly, the most common variant of ischemic stroke in the PCA basin is an isolated infarction of the cerebral hemispheres, primarily the occipital lobes; combined damage to the thalamus and cerebral hemispheres is less common, in a small percentage of cases - an isolated infarction of the thalamus and, finally, a combination of damage to the midbrain, thalamus and /or hemispheres is the rarest option [2].
Sometimes there is bilateral damage to areas of the brain supplied by blood from the PCA. This occurs primarily in top of the basilar syndrome, which is an embolic occlusion of the distal basilar artery and is characterized by depression of consciousness, visual disturbances, oculomotor and behavioral disorders, often without motor dysfunction [2].
According to a number of authors, the most common and characteristic signs of infarctions in the PCA are visual disturbances (up to 95% of cases), homonymous hemianopia (66.7% of cases), central paresis of the facial nerve (52% of cases), headache, mainly in the occipital region. areas (50 cases), sensory disorders (40% of cases), aphasic disorders (38% of cases), hemiparesis (18% of cases) and niglect (10% of cases). Patients usually have a combination of symptoms [2, 7, 8, 11].
Homonymous hemianopia occurs on the contralateral side with infarctions in the areas of blood supply to the hemispheric branches of the PCA due to damage to the striate cortex, optic radiation or lateral geniculate body. In the absence of occipital pole involvement, macular vision remains intact. The visual field defect may be limited to only one quadrant. Superior quadrant hemianopsia occurs when there is an infarction of the striate cortex below the calcarine sulcus or inferior part of the optic radiation in the temporo-occipital region. Inferoquadrant hemianopsia is a consequence of damage to the striate cortex above the calcarine sulcus or the superior part of the optic radiation in the parieto-occipital region. Occlusion of the calcarine sulcus may also be associated with pain in the ipsilateral eye. Visual disturbances may also be more complex, especially with bilateral occipital lobe lesions, including visual hallucinations, visual and color agnosia, prosopagnosia (agnosia for familiar faces), blindness denial syndrome (Anton syndrome), visual attention deficits, and optomotor agnosia ( Balint's syndrome). Often, visual impairment is accompanied by afferent disorders in the form of paresthesia, disorders of deep, pain and temperature sensitivity. The latter indicate involvement of the thalamus, parietal lobe or brainstem (due to occlusion of the proximal vertebrobasilar region) [2, 8, 10, 20].
Neuropsychological abnormalities associated with PCA infarctions vary significantly and are present in more than 30% of cases. A stroke in the basin of the callosal branches of the left PCA in right-handed people, affecting the occipital lobe and splenium of the corpus callosum, is manifested by alexia without agraphia, sometimes color, object or photographic anomia. Right hemisphere infarctions in the PCA territory often cause contralateral hemiglect. With extensive infarctions involving the medial parts of the left temporal lobe or bilateral mesotemporal infarctions, amnesia develops. Also, with mono- or bilateral mesotemporal infarction, agitated delirium may develop. Extensive infarcts in the territory of the left posterior temporal artery may clinically manifest as anomia and/or sensory aphasia. Thalamic infarctions in the areas of blood supply to the penetrating branches of the PCA can cause aphasia (if the left pillow is involved), akinetic mutism, global amnesia and Dejerine-Roussy syndrome (disorders of all types of sensitivity, severe dysesthesia and/or thalamic pain and vasomotor disturbances in the contralateral half of the body, combined with usually transient hemiparesis, choreoathetosis and/or ballism). Also, infarctions in the PCA region may be associated with dyscalculia, spatial and temporal disorientation. [6, 12, 21, 22].
Bilateral thalamic infarcts are often associated with deep coma. Thus, occlusion of the Percheron artery causes the development of bilateral infarcts in the intralaminar nuclei of the thalamus, which leads to severe impairment of consciousness [2, 12].
Hemiparesis during infarctions in the PCA region occurs in only 1/5 of patients, is often mild and transient and is usually associated with involvement of the cerebral peduncles in the pathological process [23, 24]. Cases of infarctions in the PCA region have been described, when patients exhibited hemiparesis without involvement of the cerebral peduncles. These patients had damage to the distal parts of the PCA, primarily involving the thalamogeniculate, lateral and medial posterior choroidal arteries [23, 25]. It is assumed that hemiparesis during infarctions in the posterior choroidal arteries may be associated with damage to the corticobulbar and corticospinal tracts, even in the absence of visible damage to the internal capsule or midbrain according to neuroimaging data [23]. There are opinions that the development of hemiparesis is associated with compression of the internal capsule by edematous tissue of the thalamus [12].
Infarctions in the PCA territory mimic infarctions in the carotid system in 17.8% of patients [24], especially with combined lesions of the superficial and deep branches of the PCA, which is observed in approximately 38% of cases [7, 19, 26]. Differential diagnosis can be difficult due to the presence of aphasic disorders, nigella, sensory deficits, and usually mild and transient hemiparesis resulting from the involvement of the pyramidal tracts. In addition, memory impairment and other acute neuropsychological disorders can significantly complicate the examination of such patients [2, 18, 19].
Among other conditions that often clinically mimic infarctions in the PCA, we should highlight some infectious diseases (primarily toxoplasmosis), posterior reversible leukoencephalopathy syndrome, neoplastic lesions, both primary and metastatic, and thalamic infarctions caused by deep cerebral vein thrombosis [2 , 27]. Neuroimaging methods often play a decisive role in making a diagnosis.
The main requirements for neuroimaging in the acute period of ischemic stroke are the speed of the study and the information content of the data obtained. The main tasks facing the doctor when using these methods are to exclude a non-ischemic cause of the patient’s symptoms, determine the location and size of ischemic foci and the presence of viable brain tissue, determine the condition of the cerebral vessels, identify cerebral edema and displacement of the midline structures, as well as the presence of hemorrhagic impregnation of ischemic foci. These data should help in quickly determining the patient’s treatment tactics—the possibility of intravenous or intra-arterial thrombolysis, mechanical plaque removal, and brain decompression surgery [28, 29].
Computed tomography (CT) usually does not detect ischemic changes in the brain parenchyma during the first few hours after the onset of stroke, the time most important for initiating therapy, and sometimes even later in the disease. Visualization of the posterior regions of the brain is especially difficult due to artifacts caused by the bones of the skull. However, with strokes in the territory of the PCA, as well as with strokes in the territory of the middle cerebral artery, in some cases, CT may show a hyperintense signal from the PCA itself, which is the earliest sign of a stroke in its territory and is detected in 70% of cases within the first 90 minutes from onset of the disease and in 15% of cases within 12 to 24 hours. This sign appears due to visualization of a calcified embolus or atherothrombosis in situ. On a standard CT scan, the slice plane is parallel to the orbitomeatal line (the line connecting the outer corner of the eye with the external auditory canal and then going to the first cervical vertebra). Based on the course of the SMA, its lumen is usually visualized in one section, which makes it easy to identify hyperdense SMA, especially in the presence of atrophic changes in the brain. The course of the PCA is more complex. Typically, its proximal segment ascends laterally around the cerebral peduncles and, reaching the bypass cistern, goes horizontally inward to the temporal lobe, in close proximity to the tentorium cerebellum. The circular part (P1 and P2 segments) ends in the quadrigeminal cistern, where the cortical part of the PCA begins. Only the P2 segment runs parallel to the cut inside the bypass tank and, accordingly, hyperdensity, if present, can most likely be detected in this area. Subsequently, CT signs of ischemic changes appear as areas of hypointensity in the brain parenchyma [2, 3, 30].
Magnetic resonance imaging (MRI) makes it possible to more accurately determine the presence and nature of ischemic changes in the brain during stroke. Diffusion-weighted imaging (DWI) can detect early ischemic changes, often within an hour of symptom onset, and localize and extend lesions more accurately than CT [2]. The combined use of DWI, ADC and FLAIR modes makes it possible to differentiate acute, subacute and chronic ischemic changes in the brain parenchyma, as well as to distinguish cytotoxic brain edema observed in ischemic stroke from vasogenic edema in the syndrome of posterior reversible leukoencephalopathy and hypertensive encephalopathy [2, 27, 31 , 32].
CT angiography (CTA) plays a significant role in the non-invasive diagnosis of steno-occlusive lesions of large extra- and intracranial arteries. This technique makes it possible to identify the degree of stenosis, plaque morphology, as well as the presence of arterial dissection in both vertebrobasilar and carotid vessels. In addition, the anatomical features of collaterals and circulation options of the PCA are assessed [2, 33, 34]. Additional information about vascular anatomy can be obtained using contrast-enhanced MR angiography, which, in combination with CTA, allows for data that previously could only be obtained using classical angiography. In addition, these methods are important in assessing the effectiveness of thrombolytic therapy in the case of arterial recanalization [2].
Currently, thrombolytic therapy for ischemic stroke can be used for damage to the arteries of both the carotid and vertebrobasilar areas. Nevertheless, all currently existing guidelines for thrombolysis are focused primarily on vascular catastrophe in the carotid region, primarily the middle cerebral artery; this is primarily due to the presence in such patients of obvious neurological deficits in the form of severe paresis and sensory disturbances. A typical functional deficit in a patient with a heart attack in the PCA region in the acute period is not always regarded by the doctor as disabling. The assessment of neurological deficit according to the National Institutes of Health Stroke Scale (NIHSS), which is one of the criteria for selecting patients for thrombolytic therapy, usually is not able to fully reflect the severity of the condition of a patient with a vertebrobasilar infarction [7]. There are no recommendations at all regarding an isolated visual field defect in acute infarction in the PCA territory [2]. Therefore, thrombolytic therapy in patients with infarctions in the PCA is not widely used. However, given that hemiparesis in some cases is a significant clinical component of infarctions in the PCA territory, such patients, in the absence of contraindications, are justifiably treated with systemic and/or intra-arterial thrombolysis [35].
When comparing the efficacy and safety profiles of intravenous thrombolysis administered within the first three hours from the onset of symptoms in patients with carotid infarctions and PCA infarctions, no significant difference in safety and treatment outcome was found [7]. At the same time, according to a number of authors, when conducting intravenous thrombolytic therapy for ischemic lesions in the vertebrobasilar region, and in particular the PCA, it is possible to expand the therapeutic window to 6.5-7 hours and even more compared to 4.5 hours for infarctions in the carotid pool [36, 37].
Intra-arterial thrombolysis for occlusion of the middle cerebral artery is recommended within 6 hours from the onset of symptoms, and for occlusion of the basilar artery - no later than 12 hours [28]. However, to date there are no clear recommendations on the time limits for intra-arterial thrombolysis in patients with PCA lesions [15]. N. Meier et al. (2011) described 9 cases of intra-arterial thrombolysis in patients with PCA occlusion within the first 6 hours from the onset of the disease. 3 months after treatment, functional independence (modified Rankin scale 0-2 points) was detected in 67% of patients, which correlates with similar data for the carotid system [15].
An early diagnosis of ischemic stroke in the PCA allows the doctor to promptly determine the patient’s treatment tactics and, in the absence of contraindications, consider the possibility of thrombolytic therapy, which undoubtedly makes the prognosis for the patient more favorable.
LITERATURE
1. Brandt T., Steinke W., Thie A., Pessin MS, Caplan LR Posterior cerebral artery territory infarcts: clinical features, infarct topography, causes and outcome. Multicenter results and a review of the literature // Cerebrovasc. Dis. - 2000. - Vol. 10. - P. 170–182.
2. Finelli P. Neuroimaging in acute Posterior Cerebral Artery Infarction // The Neurologist. - 2008. - Vol. 14. - P. 170-180.
3. Krings T., Noelchen D., Mull M. et al. The hyperdense posterior cerebral artery sign // Stroke. - 2006. - Vol. 37. - P. 399-403.
4. Hill MD Posterior cerebral artery stroke // e-medicine, 2005.
5. Khasanov I.A. Features of infarctions in the basin of the posterior cerebral arteries // Neurological Bulletin. - 2012. - T. XLIV, issue. 3. - pp. 69-74.
6. Caplan L. Posterior Circulation Ischemia: Then, Now, and Tomorrow: The Thomas Willis Lecture-2000 // Stroke. - 2000. - Vol. 31. - P. 2011-2023.
7. Breuer L., Huttner H. B., Jentsch K. et al. Intravenous Thrombolysis in Posterior Cerebral Artery Infarctions // Cerebrovasc Dis. - 2011. - Vol. 31. - P. 448-454.
8. Caplan L., Bogousslavsky J. Posterior cerebral artery syndromes // Cerebrovascular Disease: Pathology, Diagnosis and Management. - 1998. - P. 1028.
9. Caplan L., Estol C., Massaro A. Dissection of the posterior cerebral arteries // Arch Neurol. - 2005. - Vol. 62. - P. 1138-1143.
10. Brazis P. Topical diagnostics in clinical neurology / P. Brazis, D. Masdew, H. Biller - M.: MEDpress-inform, 2009. - 736 p.
11. Caplan L. Posterior Circulation disease: Clinical Findings, Diagnosis and Management / Boston, MA: Butterworth-Heinemann, 1996. - 533 p.
12. Beer M. Topical diagnosis in neurology according to Peter Duus / M. Beer, M. Frotscher. - M.: Practical Medicine, 2009. - 468 p.
13. Tatu L., Moulin T., Bogousslavsky J. et al. Arterial territories of the human brain // Neurology. - 1998. - Vol. 50 - P. 1699-1708.
14. de Monye C, Dippel DW, Siepman TA et al. Is a fetal origin of the posterior cerebral artery a risk factor for TIA or ischemic stroke? A study with 16-multidetector-row CT angiography // J. Neurol. - 2008. - Vol. 255 - P. 239-245.
15. Meier N., Fischer U., Schroth G. Outcome after thrombolysis for acute isolated posterior cerebral artery occlusion // Cerebrovasc. Dis. - 2011. - Vol. 328. - P. 79-88.
16. Phan T., Fong A., Donnan G. et al. Digital map of posterior cerebral artery infarcts associated with posterior cerebral artery trunk and branch occlusion // Stroke. - 2007. - Vol. 38. - P.1805-1811.
17. Chaves CJ Posterior cerebral artery. Stroke syndromes. 2nd edition / Chaves CJ, Caplan LR Cambridge, New York: Cambridge University Press. — 2001. — 747 p.
18. Cals N., Devuyst G., Afsar N. et al. Pure superficial posterior cerebral artery territory infarction in the Lausanne Stroke Registry // J. Neurol. - 2002. - Vol. 249. - P. 855-861.
19. Kumral E., Bayulkem G., Atac C., Alper Y. Spectrum of superficial posterior cerebral artery territory infarcts // Eur. J. Neurol. - 2004. - Vol. 11. - P. 237-246.
20. Ng YS, Stein J, Salles SS et al. Clinical characteristics and rehabilitation outcomes of patients with posterior cerebral artery stroke // Arch. Phys. Med. Rahabil. - 2005. - Vol. 86. - P. 2138-43.
21. Brandt T., Thie A., Caplan L. et al. Infarkte in Versorgungsgebiet der A. cerebri Posterior // Nervenarzt. - 1995. - Vol. 66. - P. 267-274.
22. Savitz SI, Caplan LR Vertebrobasilar disease // N. Engl. J. Med. - 2005. - Vol. 352. - P. 2618-26.
23. Finelli P. Magnetic Resonance Correlate of Hemiparesis in Posterior Cerebral Artery Infarction // Journal of Stroke and Cerebrovascular Disease. - 2008. - Vol. 17. - P. 378-381.
24. Maulaz AB, Bezerra DC, Bogousslavsky J. Posterior cerebral artery infarction from middle cerebral artery infarction // Arch. Neurol. - 2005. - Vol. 62. - P. 938-941.
25. Neau J.-P., Bogousslavsky J. The syndrome of posterior choroidal artery territory infarction // Ann. Neurol. - 1996. - Vol. 39. - P. 779-788.
26. Lee E., Kang DW, Kwon SU, Kim JS Posterior cerebral artery infarction: diffusion-weighted MRI analysis of 205 patients. Cerebrovasc. Dis. - 2009. - Vol. 28. - P. 298-305.
27. Bogdanov E.I., Khasanov I.A., Mamedov Kh.I. and others. Posterior reversible leukoencephalopathy syndrome in patients with preeclampsia and eclampsia // Neurological Journal. - 2011. - No. 5. - P. 35-40.
28. Adams H., Del Zoppo G., Alberts M. et al. Guidelines for the early management of adults with ischemic stroke // Stroke. - 2007. - Vol. 38. - P. 1655-1711.
29. Wahlgren N., Ahmed N., Davalos A. et al. Thrombolysis with alteplase for acute ischemic stroke & the Safe implementation of thrombolysis in stroke - monitoring study (SITS-MOST): an observational study // Lancet. - 2007. - Vol. 369. - P. 275-282.
30. Berge E., Nakstad PH, Sandset PM Large middle cerebral artery infarctions and the hyperdense middle cerebral artery sign in patients with atrial fibrillation // Acta Radiol. - 2001. - Vol. 42. - P. 261-268.
31. Covarrubias DJ, Leutmer PH, Caumpeau NG Posterior reversible leukoencephalopathy syndrome: prognostic utility of quantitative diffusion-weighted MR image // AJNR Am J. Neuroradiol. - 2002. - Vol. 23, N 6. - P. 1038-1048.
32. Garg R. Posterior leukoencephalopathy syndrome // Postgrad. Med. J. - 2001. - Vol. 77, N 903. - P. 24-28.
33. Choi C., Lee D., Lee J. et al. Detection of intracranial atherosclerotic steno-occlusive disease with 3D time-of-flight magnetic resonance angiography with sensitivity encoding at 3T // AJNR Am J. Neuroradiol. - 2007. - Vol. 28. - P. 439-446.
34. Lev M., Farkas J., Rodrigues V. et al. CT angiography in the rapid triage of patients with hyperacute stroke to intraarterial thrombolysis: accuracy in the detection of large vessel thrombus // J Comput Assist Tomogr. - 2001. - Vol. 25. - P. 520-528.
35. Ntaios G., Spengos K., Vemmou AM et al. Long-term outcome in posterior cerebral artery stroke // European Journal of Neurology. - 2011. - P. 156-162.
36. Forster A., Gass A., Kern R. et al. MR Imaging-Guided Intravenous Thrombolysis in Posterior Cerebral Artery Stroke // AJNR Am J. Neuroradiol. - 2011. - Vol. 32. - P. 419-421.
37. Montavont A., Nighoghossian N., Derex. L et al. Intravenous r-TPA in vertebrobasilar acute infarcts // Neurology. - 2004. - Vol. 62. - P. 1854-1856.
Diagnostics
When collecting anamnesis, it is necessary to determine the onset of cerebrovascular accidents, establish the sequence and rate of progression of certain symptoms. Ischemic stroke is characterized by the sudden onset of neurological symptoms. In addition, attention should be paid to possible risk factors for ischemic stroke (diabetes mellitus, arterial hypertension, atrial fibrillation, atherosclerosis, hypercholesterolemia, etc.).
A physical examination of a patient with a possible diagnosis of ischemic stroke is carried out according to generally accepted rules for organ systems. When assessing the neurological status, pay attention to the presence and severity of cerebral symptoms (headache, impaired level of consciousness, generalized convulsions, etc.), focal neurological symptoms and meningeal symptoms. Laboratory tests should include general and biochemical blood tests, coagulogram, and urinalysis.
Instrumental diagnosis of ischemic stroke:
- MRI of the brain. The effectiveness of a new MRI mode, which produces diffusion-weighted images, has been proven. As a result of cytotoxic edema during ischemic stroke, water molecules move from the extracellular space to the intracellular space, which leads to a decrease in the rate of their diffusion. These changes appear on diffusion-weighted MRI images as an increase in signal, which indicates the development of irreversible structural damage to the brain substance.
MRI of the brain. Area of diffusion restriction in the cerebellum and brainstem on the left (acute ischemic stroke)
- CT scan of the brain. One of the early CT signs of ischemic damage in the MCA system is the lack of visualization of the lenticular nucleus or insular cortex (due to cytotoxic edema developing in the affected area). In some cases, with ischemic stroke, hyperdensity of sections of the middle and, much less frequently, posterior cerebral artery on the affected side is determined as early changes (a sign of thrombosis or embolism of these vessels). Already at the end of the first week, in the zone of ischemic damage in the gray matter, an increase in density to an isodense and even slightly hyperdense state is observed, which indicates the development of neovasogenesis and restoration of blood flow. This phenomenon has a “fogging effect”, because Difficulties arise in identifying the boundaries of the ischemic lesion zone in the subacute period of cerebral infarction.
CT scan of the brain. Extensive ischemic stroke in the temporal and parietal lobes on the right
Differential diagnosis
MRI and CT of the brain are also used to differentiate ischemic stroke from other forms of intracranial pathology and dynamic monitoring of tissue changes during the treatment of ischemic stroke. First of all, ischemic stroke must be differentiated from hemorrhagic stroke. Neuroimaging research methods will play a decisive role in this issue. In addition, in some cases there is a need to differentiate ischemic stroke from acute hypertensive encephalopathy, metabolic or toxic encephalopathy, brain tumor, as well as infectious brain lesions (abscess, encephalitis).
Clinical picture
The right hemisphere of the brain is a place of accumulation of nerve cells that provide perception of the surrounding world through the senses, spatial awareness of the body, as well as processing information coming from analyzers. The peculiarity of left-handers is that their speech center is located in the right hemisphere.
Obstruction of the right carotid artery often has no specific signs. The development of neurological disorders in this case is due to insufficient blood supply in the anterior, middle and posterior cerebral arteries on the right side. Neurologists at the Yusupov Hospital sometimes note a “flickering” of symptoms in patients with this form of circulatory disorder. With this condition, patients may develop complete or partial left-sided paralysis, combined with speech impairment, but it disappears after a few minutes or hours.
Spasm or blockage of the right internal carotid artery is manifested by low blood pressure in the retina of the right eye, enhanced by pulsation in the facial arteries. A neurologist can detect a blood clot in a major vessel by palpating the neck, as well as by angiography. If this formation is detected, urgent surgical intervention is performed at the Yusupov Hospital.
The rehabilitation period is characterized not only by impaired motor functions, but also by emotional manifestations: a depressive state is sharply replaced by unreasonable joy, lack of a sense of proportion and tact. Extensive damage to the right hemisphere of the brain is manifested by immobility of the face and left half of the body. Some patients have speech impairment and problems swallowing.
Lacunar ischemic stroke of the right side is diagnosed in patients with hypertension and diabetes mellitus. General cerebral symptoms of the disease are mild. In this case, in 50% of patients there is a violation of the sensitivity of the left side of the face. Some patients are unable to determine the temperature of an object and its shape by touch.
Expert opinion
Author: Olga Vladimirovna Boyko
Neurologist, Doctor of Medical Sciences
Ischemic stroke of the right hemisphere occurs as a result of severe damage to the blood vessels of the brain, which leads to impaired circulation, death of tissues and cells. Often, late access to doctors leads to death. Knowing the causes of ischemic stroke of the right hemisphere, you can prevent serious consequences.
The main and most obvious manifestations of the lesion are disturbances in auditory, visual and tactile functions. The person loses coordination of movements, has no control over his own body, and experiences uncontrolled bowel movements and urination. If therapy is provided in a timely manner, it is possible to avoid death, but with extensive lesions, health problems remain for the rest of life.
The main causes of ischemic stroke of the right hemisphere are:
- Vascular atherosclerosis at the stage when plaques increase in size to the extent that they completely block the lumen of the vessels.
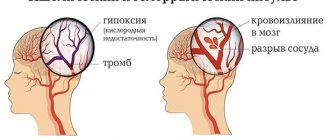
- Hypertensive crisis, in which the walls of blood vessels burst and blood enters the membranes of the brain.
- Thromboembolism, in which the lumen of the vessel is closed by a thrombus, stopping the flow of blood to one or another part of the brain.
Quite often, drug and alcohol dependent patients suffer from cerebral strokes. Factors that increase the risk of pathology include diabetes mellitus, tobacco smoking, high cholesterol levels in the blood, disorders of the heart and blood vessels, stress, and dehydration. Doctors at the Yusupov Clinic conduct a comprehensive examination of patients and, based on an accurate diagnosis, prescribe combined treatment.
Treatment of ischemic stroke
If an ischemic stroke is suspected, the patient should be hospitalized in specialized departments. If the illness is less than 6 hours old, go to the intensive care unit of the same departments. Transportation should only be carried out with the patient's head elevated to 30 degrees. Relative restrictions to hospitalization are considered to be terminal coma, terminal stage of cancer, as well as a history of dementia with severe disability.
Non-drug treatment of ischemic stroke should include measures to care for the patient, correction of swallowing function, prevention and treatment of infectious complications (pneumonia, urinary tract infections, etc.). A coordinated multidisciplinary approach to it should be applied in a specialized vascular department with an intensive care unit (ward) with the ability to perform ECG, CT, clinical and biochemical blood tests, and ultrasound examinations around the clock.
Therapy in the acute period
Drug treatment of ischemic stroke is most effective at the very beginning of the disease (3-6 hours after the first signs of the disease appear). For thrombotic etiology of stroke, selective or systemic thrombolysis is performed; for cardioembolic origin, anticoagulant therapy is performed.
In the first 48 hours of the disease, it is necessary to periodically determine the oxygen saturation of hemoglobin in arterial blood. If this figure reaches 92%, oxygen therapy should be carried out, starting from 2-4 liters per minute. A decrease in the patient’s level of consciousness to 8 points or less (Glasgow Coma Scale) is an absolute indicator of tracheal incubation. The decision on the issue in favor of mechanical ventilation or against it is made based on the basic general resuscitation principles.
If there is a reduced level of wakefulness, if there are clinical or neuroimaging signs of cerebral edema or increased intracranial pressure, it is necessary to maintain the patient's head in an elevated state of 30 degrees (without flexing the neck!). It is necessary to minimize (and if possible eliminate) cough, epileptic seizures and motor agitation. Infusions of hypoosmolal solutions are contraindicated.
Planned therapy
An important component of the treatment of ischemic stroke is the correction of vital functions and the maintenance of homeostasis. This requires constant monitoring of basic physiological indicators, correction and maintenance of hemodynamics, water-electrolyte balance, respiration, correction of increased intracranial pressure and cerebral edema, prevention and control of complications.
- Infusion therapy. Routine use of glucose-containing solutions is inappropriate due to the risk of developing hyperglycemia; therefore, the main infusion solution in the treatment of ischemic stroke is sodium chloride solution (0.9%). With concomitant diabetes mellitus, patients are transferred to subcutaneous injections of short-acting insulin, except in cases where adequate glycemic control is carried out, and the patient is in clear consciousness and without impaired swallowing function.
- Providing food. Regardless of the location of the patient (intensive care unit, intensive care unit or neurological department), the daily task of basic therapy for ischemic stroke is adequate nutrition of the patient, as well as control and replenishment of water and electrolyte losses. An indicator for enteral tube feeding is considered to be the progression of certain swallowing disorders. In this case, the calculation of nutrient doses should be carried out taking into account the metabolic needs and physiological losses of the body. When administering food orally or through a tube, the patient should be in a semi-sitting position for 30 minutes after feeding.
- Prevention of thrombosis. In order to prevent deep vein thrombosis in ischemic stroke, wearing compression stockings or appropriate bandaging is recommended. For these purposes, as well as to prevent pulmonary embolism, direct anticoagulants (low molecular weight heparins) are used.
- Neuroprotection. Its main direction is the use of drugs with neuromodulatory and neurotrophic effects. The currently best-known neurotrophic drug is a hydrolyzate from pig brain. The brain and spinal cord do not have storage properties, and cessation of blood flow for 5-8 minutes causes the death of neurons. Therefore, the introduction of neuroprotective drugs must be carried out already in the first minutes of an ischemic stroke.
Thus, early rehabilitation against the background of basic therapy, as well as a combination of reperfusion and neuroprotection, can achieve certain successes in the drug treatment of ischemic stroke.
Surgery
Surgical treatment of ischemic stroke involves surgical decompression - reducing intracranial pressure, increasing perfusion pressure, and maintaining cerebral blood flow. Statistics indicate a decrease in the mortality rate for ischemic stroke from 80 to 30%.
Rehabilitation
During the rehabilitation period after an ischemic stroke, all efforts of neurologists are aimed at restoring the patient’s lost motor and speech functions. Electromyostimulation and massage of paretic limbs, exercise therapy, and mechanotherapy are performed. To correct speech disorders (aphasia, dysarthria), as well as swallowing disorders, consultation with a speech therapist is necessary.
Lacunar stroke
Lacunar ischemic stroke occurs almost anywhere in the brain, but the most common sites are the basal ganglia, centrum semiovale, and brainstem. Lacunar infarction is a focus of ischemia, measuring 1-1.5 cm in diameter, which occurs more often against the background of stress or arterial hypertension.
In the periventricular region and centrum semiovale
Fig. 28 In the paraventricular white matter on the left there is a focus of ischemic stroke, which has an increased MR signal in T2 and Flair (lacunar ischemic stroke).
In the area of the basal ganglia
Fig. 29 In the basal ganglia on the right there is a small focus of ischemic stroke, which has an increased MR signal by DWI, T2 and Flair (lacunar ischemic stroke).
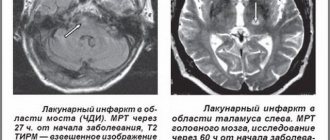
In the bridge
Fig. 30 In the left half of the pons there is a small focus of ischemic stroke, which has an increased MR signal in T2 and Flair (lacunar stroke in the brainstem).
In the amygdala of the cerebellum
Fig. 31 In the left cerebellar tonsil there is a small focus of ischemic stroke, which has an increased MR signal according to DWI, T2 and Flair.
The consequence of lacunar strokes (lacunar cysts) are small cavities in the medulla that arise after the resorption of dead nervous tissue due to lacunar ischemic stroke, also often located in areas where this type of ischemia occurs.
Fig. 32 In the paraventricular white matter, lacunar cysts are identified, also located in the basal ganglia and semi-oval center, having the appearance of local rounded voids surrounded by a rim of gliosis against the background of manifestations of vascular encephalopathy (multiple foci and diffuse zones of gliosis - increased MR signal on T2 and hypodense structure on CT).
Prognosis and prevention
The prognosis for ischemic stroke depends, first of all, on the location and volume of brain damage, the age of the patient, and the severity of concomitant diseases. The most severe condition of the patient occurs in the first 3-5 days of the disease, when cerebral edema increases in the area of the lesion. Next comes a period of stabilization or improvement with the possible restoration of impaired functions. Currently, the percentage of deaths from ischemic stroke is 15-20%.
The basis for the prevention of ischemic stroke is the prevention of thrombosis of blood vessels, which occurs when “cholesterol plaques” form in the blood. This requires maintaining a healthy lifestyle, adequate body weight, and abstaining from smoking and other bad habits. Patients suffering from various diseases of the cardiovascular system, arterial hypertension, hypercholesterolemia and diabetes are also at risk.
Secondary prevention of ischemic stroke is a comprehensive program that includes four areas: antihypertensive therapy (angiotensin-converting enzyme inhibitors and diuretics); antithrombotic therapy (indirect anticoagulants and antiplatelet agents); lipid-lowering therapy (statins); surgical treatment of carotid arteries (carotid endatherectomy).
You can share your medical history of what helped you in the treatment of ischemic stroke.
Consequences
Ischemic stroke is characterized by an acute circulatory disorder that does not go away without leaving a trace on the body. Neurologists at the Yusupov Hospital emphasize to patients and their relatives that these consequences may be irreversible.
With an ischemic stroke, general cerebral symptoms appear: impaired consciousness, vomiting and nausea, intense headache. The first consequence of a right-sided stroke is a violation of facial expression, since the facial muscles are innervated by the unilateral hemisphere. In right-sided ischemic stroke, the right side of the face is affected.
The right hemisphere provides motor functions to the left side of the body, which is why paralysis and paresis occur there. Another consequence of a right hemisphere stroke is loss of sensation on the left side of the body.
In right-handed people, speech centers are located in the left hemisphere, so with a right-sided stroke, only articulation may be impaired. If a person is left-handed, then after a stroke he may experience a loss of communication.
Poor blood circulation in the right hemisphere causes consequences such as memory impairment, disorders of will and emotions, and a depressive state. Correction of these consequences in the Yusupov Hospital occurs in the process of rehabilitation, which begins from the first days of the patient’s stay in the clinic.
Make an appointment
Rehabilitation therapy
Neurologists have developed a scheme for how to recover from an ischemic stroke in the left MCA or in another area of the brain. It includes:
- Massage. Rubbing and kneading the muscles improves blood supply and helps restore damaged innervation.
- Physiotherapy. A magnet, laser and other hardware procedures are used to improve tissue microcirculation and restore the conductivity of nerve fibers.
- Exercise therapy. An individually selected set of exercises helps restore motor function. With the help of exercise therapy, treatment after stroke, if the side of the body is paralyzed, is carried out by making the patient passive flexion and extension movements in the immobilized limbs.
- Diet. The diet of patients should consist of foods that are easily digestible. You should exclude fatty meats, smoked and pickled foods, baked goods, and also limit the consumption of salt and sugar. It is recommended to include vegetables, vegetarian soups and cereals in the menu.
- Classes with a speech therapist. Necessary for restoration of speech functions.
Neurologists are positive if folk remedies are used in addition to the main treatment. It is recommended to drink tincture of fir cones or decoctions of chamomile, St. John's wort, and sage. Traditional medicine recipes help improve the functioning of internal organs and prevent possible inflammation associated with weakened immunity.
Dangerous consequences
Complications that appear after an ischemic stroke on the left side depend on the location of the lesion on the cerebral hemisphere (hemisphere). Let us consider the consequences characteristic of left-sided ischemic stroke that may persist after treatment and rehabilitation.
Physical activity
If the motor centers are affected, then a person develops:
- sagging of half the face (half-lowered eyelid, swollen cheek, distorted mouth);
- decreased muscle strength (in severe cases, paralysis occurs);
- impaired sensitivity (the skin of the affected limbs reacts poorly to external irritations).
Difficulty in movement and sensory disturbances in left-sided cerebral ischemia occur on the right side of the body.
Internal organs
Ischemic stroke in the left hemisphere is not limited only to disruption of the innervation of muscles and skin; organs located on the right (kidney, lung, and partially the digestive tract) are affected.
The degree of change in the functioning of organs depends on how severe the innervation disorder is:
- Easy. The deviation is minor, the functions are preserved.
- Average. There is a decrease in organ functions. The patient's right side of the chest lags behind when breathing, and there may be problems with digestion and bowel movements.
- Heavy. Paralysis and complete cessation of functions occurs.
Stopping the functioning of the lung, liver or kidney is considered one of the dangerous consequences of an ischemic stroke on the left side. It is noteworthy that the severity of external and internal deviations are not related to each other. People may be paralyzed on the right side of the body, but the functionality of the internal organs is not impaired.
Speech
The centers responsible for speech are on the left. Depending on the area of damage to the hemisphere, the victim will have:
- Difficulty in grammatically constructing sentences. People begin to speak in short, simple phrases reminiscent of telegraph style. Intonation disappears. This occurs when the anterior lobes of the hemisphere are affected.
- Problems with sounds. The patient confuses sounds, placing them incorrectly in words. This is typical for stroke of the posterior lobe.
- Problems with the perception of spoken language. A person hears words addressed to him, but cannot associate them with known concepts. Similar problems arise when trying to read text. Such patients speak mainly in prepositions or conjunctions, with long, but uninformative phrases. The disorder appears with ischemia of the temporal lobe.
- Complete aphasia. Extensive ischemic stroke of the left hemisphere is often accompanied by a complete loss of the ability to speak and perceive speech.
There is also false aphasia, when the impairment of the ability to speak is associated with paralysis of the muscles of the tongue or larynx. Such people understand what is being said to them and can adequately formulate their thoughts, but when they try to speak, the result is slurred, blurred speech or isolated sounds.
Ability to think
The left side of the brain marks the ability for logical thinking. The consequence of a left-sided stroke can be:
- loss of ability to remember numbers (dates, phone numbers);
- inability to perform simple arithmetic operations in the mind (add, multiply);
- difficulty in perceiving abstract concepts;
- difficulty when trying to draw conclusions from the information received;
- difficulty making independent decisions.
Such people do not always understand their condition and often commit stupid or ridiculous actions. They are uncritical of their actions.
Psycho-emotional sphere
Another consequence of a stroke in the left hemisphere is a change in the psyche. The patient may experience depression associated with limited mobility and dependence on the care of loved ones. The person becomes:
- Maudlin. He often feels sorry for himself and cries, saying that he has become a burden to his relatives.
- Restless. Anxiety and fear appear associated with the fear of being left without outside help.
- Aggressive. The patient finds fault with others, conflicts over trifles. May complain to strangers about poor feeding or care, attracting attention to himself.
- Irritable. Such people are dissatisfied with everything, find fault with little things, and often accuse loved ones of waiting for their death.
Often, those who have suffered a cerebral infarction experience sudden mood swings when, during a calm conversation, a person becomes angry, starting to throw objects or punch the bed.