Cerebellar stroke is one of the rarest types of ischemic stroke. It has been studied very little, so doctors experience great difficulty in making a correct diagnosis. It is also considered one of the most dangerous, since the lesion can be located very close to the trunk and other vital nerve centers of the human brain.
A cerebellar stroke may appear as a ruptured blood vessel or tissue death (necrosis). The mechanism of development is very similar to other types of intracerebral strokes. Thus, the causes of occurrence and subsequent symptoms may be identical. People over the age of 40 most often suffer from cerebellar stroke, and the highest percentage of damage is observed in men. Medical statistics indicate a high mortality rate among victims. However, a favorable outcome is still possible if first aid to the victim was provided on time.
Causes of cerebellar stroke
- Blockage of a blood vessel by a thrombus or embolus;
- Rupture of the vessel wall, resulting in hemorrhage and hematoma formation.
- Dissection of a section of the vertebral artery. A very rare phenomenon, due to which a cerebellar stroke is possible in young people.
Impaired blood flow in the cerebellum due to thrombosis is most often observed in patients suffering from other blood pathologies, atherosclerosis. Patients who have recently suffered a myocardial infarction are often at high risk. Thus, blood clots can travel through the bloodstream from the heart into the cerebral arteries.
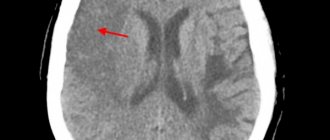
Hemorrhage in the tissues of the cerebellum is no less dangerous, and it is this that often causes the death of the victim. Blood permeating the brain tissue increases the volume of the hematoma. There is strong pressure on the cerebellar parenchyma, which in turn compresses and displaces the tissue of the brain stem. This is what can lead to sudden death of the patient.
Indications for MRI of the cerebellum
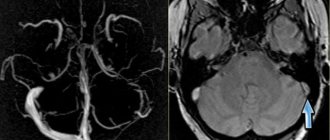
Magnetic resonance imaging is used for the primary detection of central nervous system pathologies and to clarify the diagnosis when other research methods are insufficiently effective. The scan allows you to assess the condition of the cerebellum and the meninges of the posterior cranial fossa and shows the characteristics of the blood supply to the area in question. Using MRI, the nature and pathogenesis of the disease, the degree of tissue damage, and the localization of the process are determined.
Arnold-Chiari malformation (II) on MRI
The cerebellum is a section of the central nervous system, located in the posterior cranial fossa and is responsible for coordination of movements, muscle tone, and the ability to maintain balance. The organ has three pairs of legs, with the help of which it receives information from the trunk and cortex of the cerebral hemispheres, basal ganglia, extrapyramidal system, and spinal cord.
Pathological changes in the structures and pathways of the cerebellum are accompanied by a characteristic clinical picture:
- paroxysmal headaches;
- fainting;
- dizziness;
- when the process is localized in one of the cerebellar hemispheres, deviation in the direction of the lesion is possible while walking;
- decreased muscle tone, loss of motor function;
- fine motor disorders;
- unsteady “cerebellar” gait, similar to the movements of a drunk;
- decreased blood pressure;
- memory and speech disorders.
The presence of these symptoms serves as a basis for prescribing MRI of the cerebellum. In case of injuries to the occipital part of the head, the procedure is carried out to identify internal injuries: hematomas, swelling, etc.
Indications for magnetic resonance scanning are suspicions of the following pathological conditions:
- benign and malignant neoplasms in the posterior cranial fossa;
- congenital malformations (Arnold-Chiari, Joubert malformations, Dandy-Walker syndrome);
- ischemic and hemorrhagic stroke of the cerebellum;
- encephalopathy;
- abscess, granulomatous inflammation of the cerebellar tissue;
- vascular malformations;
- demyelinating pathologies involving the cerebellum.
MRI is indicated before brain surgery. Scanning allows you to clarify the location and size of the pathological focus. 1-3 months after the intervention, a follow-up examination is carried out to assess the recovery processes.
Symptoms of cerebellar dysarthria
The basic symptom of the disorder is speech dyspraxia. It is characterized by:
- arrhythmia of speech;
- sounds and words are pronounced abruptly - there is no smoothness;
- the child does not use stress in words, there are no accents in speech.
Cerebellar dysarthria (the structure of the defect) is also manifested in the characteristics of the voice: its strength is inconsistent, the speech flow is jerky.
Children make many sounds through their nose. Long vowels sometimes sound trembling.
Another symptom of cerebellar dysarthria is slurred speech, which is difficult for the child. In the process of verbal communication, vasomotor reactions appear: the skin of the face turns pale or red, sweating is increased. He gets so tired of expressive speech that he tries to speak briefly or, if possible, remain silent.
Characteristics of cerebellar dysarthria such as unsteady gait, poor handwriting, poor coordination of movements are also noted; children have difficulty chewing solid food.
Forecast and prevention of cerebellar dysarthria
The prognosis for regression of the disease is good. But subject to timely and comprehensive treatment.
The first condition is to identify the cause of the disease and direct therapy towards its elimination.
The second condition is speech therapy work aimed at restoring and improving speech skills.
How pronounced the residual symptoms of cerebellar dysarthria will be depends on the degree of damage to the cerebellum. The most difficult disease to treat is one that develops against the background of oncology or hereditary diseases.
Contraindications
Unfortunately, this diagnostic method is not available to everyone. MRI of the cerebellum should not be performed on people who have metal-containing structures in their bodies. These are not only rods that are installed for fractures, but also crowns, implants, and pacemakers. Diagnosis can be difficult due to heavy weight. The space in the tomograph capsule is limited. If you have a weight above 250 kg, your doctor will recommend an alternative method of examining the cerebellum.
Relative contraindications include neurological or mental diseases, in which it is difficult to remain still for a long time, as well as pregnancy - in this case, the examination can be carried out in agreement with the attending physician.
Please note that scanning the cerebellum can also be carried out using contrast agents - in this case, before the study you should make sure that there is no allergic reaction.
Preventive actions
There is no specific prevention as such. Complete cure is excluded.
With good care and supportive treatment, the patient's life can be brought just a little closer to normal and extended as much as possible.
Creating comfortable conditions for the patient depends only on close people, if someone in the family is sick. And doctors can only help prevent the disease from progressing quickly.
How is the diagnosis done?
MRI of the brain is performed using two types of tomographs:
- open devices;
- devices with a tunnel (pipe).
The first ones are equipped with a couch and a magnetic frame. The patient lies on his back, his head is in the zone of action of the force field. Open tomographs allow people suffering from claustrophobia and overweight patients to do MRI. The disadvantage of the study is the insufficiently high resolution of the images.
Closed tomographs include a movable table, a tunnel, a gradient coil, software equipment and a monitor on which the image is received. The patient lies face up, the body and limbs are fixed with bolsters and fastenings. Special headphones provide noise protection. An alarm button is placed in the patient’s hand, with which you can stop the session.
MRI of the head on a closed tomograph
The presence of foreign electronic devices in the area of effect of the tomograph's force field can lead to breakdown of expensive equipment, so the doctor and x-ray technician are located at the equipment behind a transparent partition during the procedure. Communication with the subject is maintained via a microphone.
A gradient coil is installed above the patient's head, which produces an alternating electromagnetic pulse. When moving the table with the patient into the tomograph tunnel, a constant force field generator is turned on. The gradient effect provides cut selection, increases scanning speed and photo resolution.
Closed tomographs induce a magnetic field with a strength of 1.5 Tesla. This power is sufficient for a detailed study of internal organs and structures.
Scanning is carried out in axial, sagittal and frontal projections. The thickness of the section during the study is adjusted individually (from 1 mm). Sensors record the signal, and a computer program transforms the information into a series of black and white photographs on a monitor. If necessary, a three-dimensional reconstruction of a brain model is possible with a detailed display of the relative position of cerebral structures, nerves, and blood vessels.
When using contrast, scanning is paused after a series of native images. The patient is given a gadolinium solution through an intravenous catheter. The procedure is continued after filling the vascular bed and intercellular space in the area of interest with the drug.
Arnold-Chiari syndrome (displacement of the cerebellar tonsil below the boundaries of the foramen magnum)
MRI diagnostics takes up to half an hour, contrast enhancement increases the scanning time by 10-15 minutes.
Complications and consequences
The consequences of cerebellar atrophy are irreversible. In the absence of support from the body at the initial stage, the end may be complete degradation of the personality, both social and physiological.
As the pathology progresses, it is impossible to reverse the destruction processes, but it is possible to slow down and freeze the symptoms in order to prevent further progression. A patient with cerebellar atrophy begins to feel inferior because he develops: a disturbed, drunken gait, all movements become uncertain, he cannot stand without support, it is difficult for him to walk, speech is impaired due to impaired tongue movements, phrases are constructed incorrectly, he cannot clearly express his thoughts.
Social degradation is gradually occurring. The trembling of the whole body becomes constant, the person can no longer do basic things that were previously possible.
Symptomatic manifestations
Atrophy of the cerebellum of the brain is destructive for the patient, because with the death of nerve cells, pathological processes become irreversible.
Cerebellar disorders include several groups of disorders:
- First group. Impaired smooth movements of the limbs (mainly the arms). This is manifested by trembling of the hand at the end of any purposeful movement.
- Speech disorders.
- Voluntary movements and speech become slow. Next, the handwriting changes. Since the cerebellum is associated with motor acts, disturbances in its functioning are movement disorders.
Symptoms of cerebellar atrophy: asynergy of the muscles of the legs and torso, with difficulties arising when the patient attempts to rise from a lying position and sit down. These are very common signs of an affected cerebellum, and they indicate a disorder in the synergy of muscles (coordination of work) belonging to different muscle groups when they participate in the same motor act. The combination of simple and complex movements is completely disordered and disrupted.
Signs of cerebellar atrophy:
- The occurrence of incoordination of movements, the appearance of paralysis and various speech disorders. People cannot move smoothly, they sway in different directions, their gait becomes uncertain.
- Tremor and nystagmus (involuntary oscillatory movements of the eyeballs when they are abducted). Tremor is constantly present - during movement and at rest. Speech becomes scanned and dysarthric. What does this mean? A person with dysarthria has difficulty pronouncing words or distorts them due to unclear pronunciation.
- Scanned or telegraphic speech is possible. It is rhythmic, but the stresses are not placed according to the meaning, but correspond only to the rhythm.
- Muscle tone decreases due to atrophy of nerve fibers.
- Dysdiadochokinesis is a lack of coordination when the patient cannot perform rapid alternating movements.
- Dysmetria – the patient cannot control the amplitude of movement, i.e. accurately determine the distance between an object and himself.
- Hemiplegia arises from paralysis.
- Ophthalmoplegia is paralysis of the eyeballs, which can be temporary.
- Hearing impairment.
- Swallowing disorder.
- Ataxia - unsteadiness of gait; may be temporary or permanent. With such a drunken gait, the patient drifts towards the lesion.
- Severe cephalgia, with nausea and vomiting, dizziness due to increased intracranial pressure (ICP), and drowsiness are also possible.
- Hyporeflexia or areflexia is a decrease or complete loss of reflexes, urinary and fecal incontinence. Mental deviations are often possible.
Diagnostic measures
First, the neurologist conducts a reflex study to identify the location of the central nervous system lesion.
Also prescribed:
- MRI of cerebellar atrophy allows you to clarify in detail all the changes in the cortex and subcortex. The diagnosis can be determined in the early stages of the disease. This method is the most reliable.
- CT gives a complete picture of changes after strokes, identifies their cause, and indicates the location of cystic formations, i.e., all the causes of tissue trophic disorders. Prescribed for contraindications to MRI.
- Ultrasound examination is used to diagnose extensive brain damage due to strokes, TBI, trauma and age-related changes. Can identify the area of atrophy and determine the stage of the disease.