Description
Synonyms (rus): NMDA receptor, NMDAR-autoimmune encephalitis
Synonyms (eng): NMDAR-associated autoimmune disorder
Biomaterial: serum/cerebrospinal fluid
Indicator(s): Antibodies to NDMAR
Method(s): Indirect immunofluorescence reaction
Container type and preanalytical features: Sterile container, WITHOUT additives, 60 ml; / Biochemical tube with coagulation activator, 6 ml (red or brown cap)
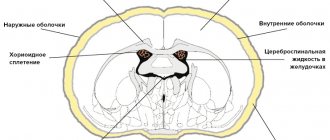
Antibodies to the NMDA (N-methyl-D-aspartate)-glutamate receptor belong to the family of “antineuronal antibodies” that react with the receptor apparatus of neurons, mediating interneuronal signal transmission and synaptic plasticity. They are the main marker of “classical” autoimmune encephalitis (AE), a disease that predominantly affects young women and adolescents. Encephalitis is often paraneoplastic in nature and is associated with teratoma of the ovaries and testicles. The disease debuts with behavioral disorders, then disturbances of consciousness and convulsions develop. In some cases, it is noted independently, without connection with the tumor. Detection of antibodies to NMDA in the cerebrospinal fluid is a more preferable approach to diagnosing autoimmune encephalitis.
Anti-NMDA receptor encephalitis
Part 1: Anti-NMDA receptor encephalitis and schizophrenia In search of the causes of mental illness, scientists reach the smallest structures: we are no longer talking about the lobes and sulci of the brain, but about antibodies, enzymes, cytokines and receptors. We first saw that neurotransmitters and their receptors are involved in the genesis of mental disorders in the example of psychotropic drugs: medical practice here was ahead of the understanding of the phenomenon. Only now, when more subtle research methods have become available, are scientists beginning to understand what exactly was discovered: what is happening with neurotransmitter metabolism and why. What makes a well-functioning mediator system go astray? One of the answer options is immune autoaggression . It was once believed that the brain was inaccessible to the immune system, but recently more and more evidence has emerged regarding the normal presence of immune agents in nervous tissue; Of course, the question also arises about what happens in pathology, including mental disorders. Indeed, there are significant deviations - the term “neuroinflammation” is very popular among psychiatrists. External agents as the cause of such disorders are excluded in the first place; it can only be immune; the question remains: is it inflammation that leads to dysfunction of the neurotransmitter system, which is corrected with psychotropic drugs. If this is true, the current approach to treating mental disorders is wrong: therapy should primarily target the immune system. This is already practiced: for example, NSAIDs are added to treatment regimens for schizophrenia and depressive episodes - and they get a good effect. In this case, it is enough just to detect the structures that have come under fire from one’s own immune system, and the mystery of mental disorders is solved. We know that pathogenesis must involve some part of the neurotransmitter metabolism (why not the receptor) and there is autoimmune inflammation, which may just affect it. anti-NMDA receptor encephalitis (anti-NMDAR encephalitis) caused so much emotion a clinical picture of a psychotic disorder that cannot be distinguished from schizophrenia, antibodies to NMDA receptors - it seems that we have begun to understand something. But as always, everything turned out to be not so simple. Anti-NMDAR encephalitis was first described as recently as 2007. For the first time, a fairly homogeneous group of patients was registered: young women with ovarian teratoma, who developed a psychotic state, then, against its background, neurological disorders, primarily motor ones. Neurological symptoms were completely polymorphic: extrapyramidal hyperkinesis and epileptic seizures, sleep disorders, vegetative manifestations, disturbances of consciousness up to coma. Psychopathological symptoms persisted throughout the entire illness, regardless of the severity of neurological symptoms (except for periods of loss of consciousness) and corresponded to the clinical picture of schizophrenia up to lucid catatonic episodes; It was these symptoms that appeared first, and most patients initially saw a psychiatrist.
Neurological symptoms progressed very quickly (within several months) and often threatened with death, but with removal of the tumor they resolved almost immediately - the disease was regarded as paraneoplastic. However, it later became clear that it could recur; After successful treatment, complete remission lasted from 3 months to 6 years. Attentive clinicians asked patients how the disease began - a quarter said that shortly before the development of the first symptoms they suffered something similar to a viral disease (upper respiratory tract catarrh, fever, headache). Antimycoplasma immunoglobulins, ASL-O, were identified from antibodies to bacterial antigens with DTP shortly before the development of symptoms . Here, some doctors recalled lethargic encephalitis: the same polymorphic picture of neurological and psychiatric disorders after a prodromal period reminiscent of an infection. Since encephalitis lethargic itself remains a mystery, it is impossible to confirm or refute this hypothesis; but, for example, characteristic postencephalitic parkinsonism was not noted in such patients. In addition to lethargic encephalitis, a connection with an increase in the titer of anti-NMDA receptor antibodies was found in Hashimoto's encephalitis and PANDAS syndrome, also autoimmune. Researchers became interested in NMDA receptors and antibodies to them, which served as a criterion for diagnosing the disease. Although it was quite rare, having collected more cases, doctors saw that, firstly, symptoms do not always develop against the background of a tumor disease (and not only against the background of teratoma, if it does exist). And secondly, especially when it is relatively mild, then if neurological disorders do not bring the patient to intensive care or are completely absent (while psychiatric disorders were always present), diagnosis presents great difficulties: it is almost impossible to suspect autoimmune encephalitis in a patient, and routine detection No one will carry out antibodies. It is logical to assume that in a certain number of patients seen by psychiatrists and neurologists with completely different diagnoses, the analysis will give a positive result. What if everyone has? Patients with schizophrenia were studied. Schizophrenia-like psychotic symptoms with transient pharmacological blockade of NMDA receptors in healthy volunteers have previously been reported, and this mechanism has been considered as a potential explanation for the genesis of schizophrenia; but to prove it as the main one, and even to see the reason, would be a breakthrough. In fact, antibodies to the NMDA receptor were found in a very small number of patients diagnosed with schizophrenia according to DSM-IV criteria: the largest percentage in the study was 6.5%, and according to the meta-analysis, even 1.49%. It is impossible to say that the cause of schizophrenia is autoimmune aggression against NMDA receptors, but at the same time the question arises of how to explain the pharmacological and genetic data confirming the role of these receptors. But we cannot ignore the small percentage of patients in whom antibodies were detected - apparently, they need treatment in accordance with the principles of therapy for autoimmune diseases. In addition, since patients with anti-NMDAR encephalitis are characterized by tumor processes, as well as autoimmune diseases, as revealed in further studies, patients with positive results must be further examined in a somatic clinic to exclude them. As one might expect, the pathogenesis of schizophrenia is still more complex than damage to a single type of glutamate receptor, but it does occur. What happens to most patients with schizophrenia at the neurotransmitter level - are there some other disorders in glutamate metabolism, maybe also autoimmune? Do disorders in other neurotransmitter systems produce the same symptoms? Or maybe schizophrenia is not at all a physiologically and biochemically homogeneous disease, and in different patients the symptoms are associated with heterogeneous disorders of neurotransmitter metabolism? Based on psychoproducts alone, it would be difficult for a physician to assess whether a patient is under the influence of LSD, which acts on serotonin receptors, or, for example, an anticholinergic drug. Perhaps a psychiatrist is in the same situation when he sees different patients with schizophrenia. The specific features of hallucinatory images for each mechanism of action of a narcotic drug can be identified by focusing on the differences and knowing exactly which drug is involved in each case, but the psychiatrist works differently. The content of the images is of little interest to him, and the criteria by which the diagnosis is made do not allow him to dwell on these differences. Therefore, the important opportunity that anti-NMDAR encephalitis gives us is to try to identify a group whose nature of disorders is more or less clear from the rest of the patients, and to more accurately trace the correlation between “physiology” and “phenomenology”. The obvious purpose of isolation is to provide such patients with adequate treatment that specifically targets the autoimmune process . Although, referring to what was said above about possible neuroinflammation (albeit not always in relation to NMDAR) in the vast majority of patients and the existing practice of prescribing NSAIDs in addition to antipsychotics, perhaps a patient with antibodies to NMDA receptors with a diagnosis of schizophrenia was just lucky switch earlier to treatment that is effective for all patients with this diagnosis. In terms of treatment, anti-NMDA receptor encephalitis does not present such difficulties as with diagnosis. A small number of patients (about 2%) were completely cured by removal of the tumor that triggered the autoimmune process. Most patients who had a tumor required treatment with drugs that affect the immune system in addition to surgery, and the same applied to patients who did not have a tumor. The first line of immunotherapy included steroids and intravenous immunoglobulins; in a smaller number of patients (according to the severity of the condition), plasmapheresis was used. Significant improvement occurred in half of those receiving this treatment within four weeks. The remainder were divided into two groups: the first continued to be treated with the same drugs or stopped altogether, the second switched to second-line therapy. This included the use of rituximab and cyclophosphamide; among those receiving these drugs, 78% were practically healthy at the examination after 2 years; Among those who continued first-line therapy or stopped treatment, the percentage of those who recovered after 2 years was 55%. In general, we can talk about a fairly high probability of regression of symptoms over time, even in the absence and ineffectiveness of treatment. Over a two-year follow-up period, relapse occurred in 12% of patients, mainly in those whose disease was not associated with a tumor process. More than half of all exacerbations were less severe than the first episode of the disease; the likelihood and severity of an exacerbation was significantly reduced by immunotherapy. But given the current clinical picture, the need for just such treatment is not obvious: data is provided that 77% of patients are initially treated by a psychiatrist, and the target of treatment is not the immune system. If there is a small percentage of such patients in every psychiatrist's practice, and they are treated with a diagnosis of schizophrenia, will they be any different from other patients in relation to psychopharmacological therapy? There is experience with the use of almost all types of antipsychotics for anti-NMDAR encephalitis; the features concern not so much their effectiveness as their side effects. Firstly, encephalitis itself can cause extrapyramidal symptoms. Not only does the prescription of typical antipsychotics increase the likelihood of its development and severity; If such symptoms appear after prescribing a classic antipsychotic to a patient with psychosis, they will be interpreted as a side effect of the antipsychotic and will complicate the diagnosis of autoimmune encephalitis. Secondly, in neuroleptic malignant syndrome (NMS), antibodies to NMDAR are produced even in those patients who previously did not have them; Apparently, autoimmune aggression against NMDA receptors is also one of the elements of the pathogenesis of NMS as an independent pathology. Due to the already existing NMDAR lesion, NMS in such patients will be even more severe, but, on the other hand, it can lead to overdiagnosis of anti-NMDAR encephalitis. Among mood disorders in patients with this type of antireceptor encephalitis, mania . The use of both valproic acid and lithium has been described, but given the possibility of seizures and associated sleep disturbances, the authors of a review on the psychopharmacology of anti-NMDA receptor encephalitis recommend benzodiazepines, including intravenously. They are also recommended if the patient develops catatonia . Prescribing antipsychotics here is dangerous, since NMS is more likely to develop: catatonia also refers to conditions accompanied by an increase in the titer of antibodies to NMDA receptors. A controversial measure is the use of electroconvulsive therapy (ECT) . Pathogenetically, it is justified, since there is evidence that after the use of ECT in the nervous tissue, the content of mRNA of NMDA receptor subunits increases, which would contribute to their restoration. On the other hand, it is reported that, having thus stopped an attack of catatonia, the doctor subsequently receives a more resistant psychosis. No significant differences from patients with schizophrenia were found in response to psychopharmacotherapy; in the absence of information about the nature of the disease, they would receive the same therapy as other patients with psychotic symptoms for a very long time. But the data on the results of immunotherapy are impressive: in the next two years after diagnosis, most patients achieved almost complete regression of symptoms, and if the disease recurred, as a rule, it was a single episode, much less severe compared to what psychiatrists treated for a long time and unsuccessfully before. We are, of course, talking about casuistic cases, but perhaps these constitute the diagnosis of schizophrenia. Even if this is one percent, it is important that within two years the patient can, as psychiatrists dream, be returned to society - and that scientists interested in the pathogenesis of schizophrenia can sleep one percent more peacefully.
Antireceptor encephalitis is quite rare: in developed countries (where it is generally possible to diagnose them), the prevalence is only 5–10 per 100 thousand people . They began to be “found” recently, at the beginning of this decade; Basically, testing for antireceptor antibodies is carried out in patients with an unclear etiology of the disease or for research purposes. Due to the high cost, such an analysis is simply not prescribed if there is no doubt about the diagnosis. However, firstly, these data could reveal to us new facets of the pathogenesis of long-known diseases, and secondly, since this group of diseases is new and little studied, doctors can easily fit the symptoms they see into the framework of long-known diseases, and Even scientists have not yet developed a complete understanding of how often it is actually necessary to check the level of antibodies to receptors. From what is known today, all antireceptor encephalitis shares common features (which are clearly seen in the example of anti-NMDA receptor encephalitis):
- psychiatric and neurological symptoms,
- often - association with tumors or predisposition to autoimmune diseases,
- good response to immunotherapy,
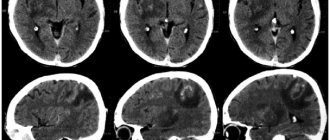
- Among the diagnostic signs: some patients have lymphocytic pleocytosis in the analysis of cerebrospinal fluid and abnormal MRI results (it is these indicators that often cast doubt on the previous neurological or psychiatric diagnosis - if it comes to them).
Part 2: The jungle of antibodies In the first part, we already noted why such diseases are really interesting: the ability to correlate the clinic with such a narrow lesion, affecting only one type of receptor. Anti-NMDAR encephalitis is the most well-known of all the diseases in this group, but since we are interested in pathogenesis, we must also talk about more rare receptor lesions. 1) Anti-GABA-B receptor encephalitis It was first described in 2010 and is rare even among anti-receptor encephalitis - it accounts for 5% of all diseases in this group . Manifested by symptoms of limbic encephalitis: amnesia, confusion and severe seizures - usually secondary generalized seizures with a source in the frontal lobe. Rarely, the disease begins with ataxia or opsoclonus-myoclonus syndrome , but always progresses to limbic encephalitis . It most often develops in elderly patients with small cell lung cancer (50% of those with anti-GABA-B receptor encephalitis have such a diagnosis, and manifestations of encephalitis may precede the detection of cancer). MRI shows unilateral or bilateral damage to the temporal lobes. In addition to antibodies to GABA-B, antibodies may be present that reflect a tendency towards an autoimmune process or the presence of a tumor. In addition to antireceptor encephalitis, limbic encephalitis can be paraneoplastic - there are only two possible reasons for its development. In the case of paraneoplastic disease, we are also talking about the formation of antibodies, but not to receptors, but more often to intracellular antigens. There are also surface-located antigens to which antibodies can be formed as part of a paraneoplastic reaction - VGPC, voltage-gated potassium channel proteins. This paraneoplastic process is especially common in patients with small cell lung cancer; there is a high probability of detecting both types of antibodies in the patient, so it is almost impossible to determine which symptoms are attributed to which autoimmune reaction. Immunotherapy gives very good results in such patients: 75% of patients recover partially or completely. The outcome largely depends on treatment of the primary tumor, if present, and care at the peak of neurological symptoms. 2) Anti-GABA-A receptor encephalitis To date, it has been reported in only 6 patients: 2 small children, 1 teenager and 3 adults from 23 to 68 years old. It was manifested by status epilepticus, which did not respond to any treatment and required an artificial coma. There were abnormalities in the analysis of cerebrospinal fluid in 5 out of 6 patients, different for all: pleocytosis, proteinosis, oligoclonal antibodies. Of all encephalitis, this one is characterized by the most pronounced changes on MRI: not only the temporal lobes are affected, as is usually the case; there are multifocal cortical and subcortical foci. Another feature was that most patients did not have tumor diseases - only one had a history of Hodgkin's lymphoma. Half of the patients received immunotherapy, and it gave good results. In one patient, the intensity of symptoms decreased over time without immunotherapy, but the epileptic syndrome persisted. The immune profile of the patients, although it served as the basis for making such a diagnosis, is quite complex. In addition to anti-GABA-A, most patients had antibodies to GAD (antibodies to glutamate decarboxylase, the main antigen of beta cells of the pancreas; they are detected, for example, in most patients with type 1 diabetes) and TPO (thyroid peroxidase, antibodies to it are a marker autoimmune thyroid diseases). Cases of limbic encephalitis with seizures have been described in the presence of a high titer of antibodies to GAD-65 - should they, after the appearance of such data, be classified as anti-GABA-A receptor encephalitis, or vice versa? The same problem occurs with so-called Hashimoto's encephalitis, which is associated with high titres of antibodies to TPO. Additionally, antibodies to GABA-A were detected in 12 patients, but at lower titers. Their range of symptoms was wider: 2 had opsoclonus-myoclonus syndrome, 4 had rigid person syndrome, and 6 had encephalitis with convulsions of lesser severity. 3) Anti-AMPA receptor encephalitis In addition to NMDA receptors, AMPA glutamate receptors can also become victims of autoimmune aggression. Its manifestation is, as with most anti-receptor processes, limbic encephalitis, but the peculiarity here is (as with anti-NMDAR receptor encephalitis) the greater severity of psychiatric symptoms. Convulsions, on the contrary, occur less frequently, occurring in less than half of patients. According to studies, there is also lymphocytic pleocytosis, and MRI shows damage to the medial parts of the frontal lobes. Elderly women suffered more often; 70% had tumors (lung, thymus, breast). 50% had a history of autoimmune diseases: thyroiditis, type 1 diabetes mellitus, Raynaud's syndrome or rigid man's syndrome. Their presence appears to seriously worsen the prognosis. Clinically, anti-AMPA receptor encephalitis itself is indistinguishable from anti-NMDA receptor encephalitis, this can be explained by the functional similarity of the receptors. However, in a third of patients, antibodies to other proteins of the nervous tissue were also detected, and in all cases a syndrome developed that was more characteristic of this particular autoimmune lesion. This raises the question about the specificity of antibodies to AMPAR: perhaps they can be secondary to other autoimmune lesions and cause their own symptoms to a lesser extent, but the opposite situation is also possible, when it is aggression against AMPA receptors that gives specificity to the process. 4) mGluR5 and mGluR1 In addition to ionotropic AMPA and NMDA, there are metabotropic glutamate receptors, which can also become a target of autoimmune aggression. A combination of Hodgkin's lymphoma with limbic encephalitis caused by the production of antibodies to mGluR5 is known - Ophelie syndrome and . So named because, in the setting of limbic encephalitis, this disorder is associated with a high likelihood of developing delirium. Since 1982, when the syndrome was first described, a total of 5 such cases have been reported. Against the background of Hodgkin's lymphoma, cerebellar ataxia can also develop as a result of damage to the mGluR1 receptor. 5) Anti-glycine receptor encephalitis The most common manifestation of this encephalitis was rigid man syndrome and its most severe form was PERM syndrome (progressive encephalomyelitis with rigidity and myoclonus). Rigid person syndrome by :
- Actually, rigidity with a predominance of tone in the muscles of the trunk and proximal muscles of the limbs, as well as in the extensors over the flexors, due to which the patient is in a characteristic position with his head thrown back, shoulders turned, and his back sharply straightened or arched in the lower back; increased tone may or may not be accompanied by hyperreflexia;
- Myoclonus;
- Autonomic disorders;
- A sharp increase in muscle tone and spasms in response to irritation is the so-called hyperekplexia, or startle syndrome.
With PERM syndrome, symptoms of encephalomyelitis are added, the most typical being various lesions of the trunk, convulsions and ataxia. In the largest study of patients with glycine receptor antibodies, which included 42 people, 33 patients were diagnosed. MRI in most patients was not indicative; in some patients, lesions of the parietal lobes or, more often, lesions of varying length in the spinal cord were detected. The most common CSF change is, as in previous cases, lymphocytic pleocytosis. This antireceptor encephalitis turned out to be less associated with tumor diseases than others, however, in two patients who had a history of tumor (thymoma and Hodgkin's lymphoma), PERM syndrome was combined with myasthenic muscle weakness and myoclonus in response to irritation (while ordinary PERM is characterized only increased tone).
Stiff person syndrome and PERM syndrome were previously thought to be caused by the autoimmune aggression against GAD-65 discussed above in connection with limbic encephalitis. In three patients in a prospective study and in many more cases retrospectively, glycine receptor and anti-GAD antibodies were detected simultaneously, and the same question is relevant here as with anti-AMPA receptor encephalitis: there are no unimportant proteins in the tissue, and any autoimmune lesion will have pathophysiological consequences, but in some cases the level that doctors see changes are achieved only with a combination of several antireceptor processes. One of them may be predisposing, and the other may give specificity and determine the clinic, but we are just beginning to understand what follows what and what causes what symptoms. Previously, with rigid person syndrome and PERM, only GAD-65 was detected, now a group of patients have been identified in whom only antibodies to the glycine receptor are detected, but there is also a group where two autoimmune processes intersect, and perhaps new antibodies will be discovered later, common to all three groups. 6) Anti-D2 receptor encephalitis Dopamine receptor type 2 - the D2 receptor - is widely known as the target of typical antipsychotics; it is directly related to psychotic disorders - as well as to the control of movements, the disorder of which we observe during treatment with classical neuroleptics. Since damage to the basal ganglia has a fairly specific clinical picture, here scientists “knew where to look,” and antibodies to this receptor were found in Sydenham’s rheumatic chorea and Tourette’s syndrome. Psychotic disorders remain questionable: as with anti-NMDAR encephalitis, it is possible that a proportion of patients with a psychiatric diagnosis have anti-receptor antibodies and are eligible for immunotherapy. Such studies are not yet sufficient, however, according to already available data among children with a first psychotic episode (autoimmune diseases, if not paraneoplastic, which has not yet been noticed for anti-D2 encephalitis, usually manifest quite early, so children were the object of the study) patients with high titers to the D2 receptor even more than to NMDAR. Antibodies can be produced not only to receptor subunits, but also to many other proteins of the nervous tissue. Unlike some genetic diseases, where the defect can be point-specific and all pathological processes become its branches, here many structures are damaged simultaneously: if a defect in the immune system predisposes it to auto-aggression as a whole, it is unreasonable to expect that only one type of receptor is damaged, antibodies to which we found. Most of the above “diagnoses” of antireceptor encephalitis are recent constructs, but they will not live long. Intersections between them are already being found, and with the expansion of our knowledge and diagnostic capabilities, more and more different manifestations of autoimmune aggression will be discovered. The set of clinical symptoms now attributed to the defeat of one receptor will pass into the hands of a whole group; some symptoms will disappear from it, what is now one of several cases will later turn out to be a statistically insignificant rarity for this syndrome.
On the one hand, today's data on antireceptor encephalitis give us reason to think about the relationship between the clinic and the subtlest pathophysiology; on the other hand, this area is an example of how quickly names and ideas in medical science can change when new discoveries are made on its front line. Sources
- https://vk.cc/7qenjL Graus F. et al. A clinical approach to diagnosis of autoimmune encephalitis //The Lancet Neurology. – 2016. – T. 15. – No. 4. – pp. 391-404.
- https://vk.cc/7qfsdk Kim TJ et al. Clinical manifestations and outcomes of the treatment of patients with GABA B encephalitis //Journal of neuroimmunology. – 2014. – T. 270. – No. 1. – pp. 45-50.
- https://vk.cc/7qfIOW Hirsch LJ A new encephalitis with GABAA receptor antibodies //The Lancet Neurology. – 2014. – T. 13. – No. 3. – pp. 239-240.
- https://vk.cc/7qfMiK Widman G. et al. Treating a GAD65 antibody-associated limbic encephalitis with basiliximab: a case study //Frontiers in neurology. – 2015. – T. 6.
- https://goo.gl/ope9Ja Carvajal-González A. et al. Glycine receptor antibodies in PERM and related syndromes: characteristics, clinical features and outcomes //Brain. – 2014. – T. 137. – No. 8. – pp. 2178-2192.
- https://goo.gl/4osQtK Höftberger R. et al. Encephalitis and AMPA receptor antibodies Novel findings in a case series of 22 patients //Neurology. – 2015. – T. 84. – No. 24. – pp. 2403-2412.
- https://goo.gl/2vR9HB Pathmanandavel K. et al. Antibodies to surface dopamine-2 receptor and N-methyl-D-aspartate receptor in the first episode of acute psychosis in children //Biological psychiatry. – 2015. – T. 77. – No. 6. – pp. 537-547.
- Nitta M. et al. Adjunctive use of nonsteroidal anti-inflammatory drugs for schizophrenia: a meta-analytic investigation of randomized controlled trials //Schizophrenia bulletin. – 2013. – T. 39. – No. 6. – pp. 1230-1241. https://vk.cc/7mddx4
- Köhler O. et al. Effect of anti-inflammatory treatment on depression, depressive symptoms, and adverse effects: a systematic review and meta-analysis of randomized clinical trials //JAMA psychiatry. – 2014. – T. 71. – No. 12. – pp. 1381-1391. https://vk.cc/7mde3p
- Lennox BR, Coles AJ, Vincent A. Antibody-mediated encephalitis: a treatable cause of schizophrenia. – 2012. https://vk.cc/7me2LH
- Pollak TA et al. Prevalence of anti-N-methyl-D-aspartate (NMDA) receptor antibodies in patients with schizophrenia and related psychoses: a systematic review and meta-analysis //Psychological medicine. – 2014. – T. 44. – No. 12. – pp. 2475-2487. https://vk.cc/7mfdNL
- Irani SR et al. N-methyl-D-aspartate antibody encephalitis: temporal progression of clinical and paraclinical observations in a predominantly non-paraneoplastic disorder of both sexes //Brain. – 2010. – T. 133. – No. 6. – pp. 1655-1667. https://vk.cc/7mfux5
- Titulaer MJ et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study //The Lancet Neurology. – 2013. – T. 12. – No. 2. – pp. 157-165. https://vk.cc/7mupq3
- Kuppuswamy PS, Takala CR, Sola CL Management of psychiatric symptoms in anti-NMDAR encephalitis: a case series, literature review and future directions //General hospital psychiatry. – 2014. – T. 36. – No. 4. – pp. 388-391. https://vk.cc/7mvsv8
Interpretation
A negative result of detecting antibodies to the NMDA receptor in the cerebrospinal fluid significantly reduces the clinical likelihood of autoimmune encephalitis. Clinical manifestations of NMDA encephalitis include symptoms of agitated behavior, paranoia, psychosis, memory and speech impairment, and seizures. Detection of antibodies in cerebrospinal fluid is more sensitive than serum testing. Sensitivity and specificity rates are close to 100%. If characteristic symptoms of the disease are present and the result is negative for the presence of NMDA antibodies, testing for antibodies to voltage-gated potassium channels (VGKC), in particular antibodies to LGI-1 and CASPR, may be recommended. Antibody titers in cerebrospinal fluid correlate better with disease relapses than in serum. In addition, patients with a favorable outcome have a faster and greater decline in cerebrospinal fluid antibody levels than patients with an unfavorable outcome.
References
- Surovtseva, A.V., Skripchenko, N.V., Ivanova, G.P. and others. Encephalitis with antibodies to NMDA receptors. Ros Westnperinatol and Pediat., 2014. - No. 6.
- Bogadelnikov, I.V., Bobrysheva, A.V., Vyaltseva, Yu.V. et al. Encephalitis caused by antibodies to NMDA receptors of neurons. ZR, 2013. - No. 3(46).
- Kasper, D., Fauci, A., Hauseret, S. Harrison`s Principles of Internal Medicine 19/E (Vol.1). McGraw-Hill Education, 2015.
- Strukov, A.I., Serov, V.V. Pathological anatomy: textbook. - M.: Litterra, 2010. - 848 p.
- Guasp, M., Dalmau, J. Encephalitis associated with antibodies against the NMDA receptor. Med Clin (Barc), 2021. - Vol. 151(2). — P. 71-79.
Autoimmune diseases
There is also a group of encephalitis that are caused by autoimmune processes in the body. In this case, the patient's own immune cells begin to attack the brain. Diseases of this nature are extremely difficult to treat, cause dementia, and lead to disturbances in brain activity and the functioning of the peripheral nervous system. In addition to dementia, the disease is accompanied by paralysis and seizures similar to epileptic ones. Diseases of this kind include, for example, limbic encephalitis. The disease causes an autoimmune response of the body to the presence of cancer cells or a disease that is infectious or viral in nature. The rate of development of limbic encephalitis divides the disease into acute and subacute types. The causes of anti-receptor encephalitis will be discussed below.
What is encephalitis?
Encephalitis causes various pathological disorders in the body and leads to the formation of dementia (dementia). The disease can affect not only the brain, but also some internal organs and joints.
Pathological conditions can be caused by a number of reasons. Based on the factors that provoke the disease, the following types of encephalitis are distinguished:
- inflammation caused by infection;
- bacterial or fungal encephalitis;
- a disease caused by exposure to a toxic substance;
- autoimmune encephalitis.
The disease affects different parts of the brain. Inflammation can be localized in its cortex, subcortex or cerebellum. Each type has its own signs, symptoms, and treatments.
What is anti-receptor encephalitis? More on this later.
Culture and society
The symptoms of anti-NMDA receptor encephalitis have formed the basis of many works of fiction about the possession of demons in humans. Since the clinical manifestations of the disease are quite diverse, for a long time they could not distinguish it into a separate group of pathologies.
Renowned New York reporter Suzanne Cahalan has published a book, Brain on Fire: My Month of Madness. Subsequently, the work became a bestseller. The journalist talks about how long it took her illness to be identified, and how treatment and rehabilitation were carried out. The cost of medical procedures amounted to $1 million.
Lineman Amobi Okoye, a defensive end for the Dallas Cowboys, was treated for encephalitis for 17 months, including a three-month coma induced by doctors to keep his condition stable. After recovery, the football player returned to professional sports.
Acute syndrome
In acute syndrome, the disease develops rapidly over three to five days. If urgent measures are not taken, death occurs very quickly. In the subacute course of the disease, the first signs become noticeable after several weeks from the initial moment of development of the pathology. These conditions are characterized by the following symptoms:
- memory impairment;
- cognitive disorders;
- epileptic seizures;
- mental disorders (high level of anxiety, depressive states, agitation);
- behavioral disorders.
In addition, obvious signs are: progressive dementia, sleep disturbances, epileptic seizures with hallucinations. It is not uncommon for autoimmune brain lesions to be correlated with the presence of cancer. Typically, such encephalitis is caused by lung cancer.
Possible complications
Autoimmune diseases are difficult to diagnose, so if the doctor does not have the proper experience, the patient may end up in a psychiatric clinic due to an incorrect diagnosis. Lack of necessary treatment leads to psychiatric disorders, which are often irreversible. In addition, there is a high chance that the patient may fall into a coma. If the patient does not take the medications necessary for treatment, a vegetative state develops very quickly, and death occurs in a third of patients.
Consequences
The consequences of suffering from anti-NMDA receptor encephalitis are reflected in the state of the cognitive sphere. In some cases, during the rehabilitation period you will have to relearn how to walk and control your body. Sometimes patients involuntarily make movements with their hands.
Dangerous consequences include loss of sensitivity of certain receptors (hunger, thirst). The patient may not eat or drink for a long time, which increases the risk of worsening his condition. Loss of skin sensitivity can lead to burns and various injuries.
The patient's memory is deteriorating. Some people do not remember events that happened earlier than a week ago. During rehabilitation and after recovery, the patient has to take a large amount of medications.
Complications include progressive dementia (dementia). However, it does not develop in all cases.
About 50% of patients recover completely. A third of patients have minor residual effects. According to statistics, 10% of cases of the disease are fatal. When the tumor is at the initial stage of development, body functions are completely restored. The chance of a favorable outcome increases if you consult a doctor at the first symptom.
Infectious and bacterial inflammations
The factors that cause infectious encephalitis are viruses and bacteria. For example, herpes virus, HIV infection, encephalitis virus, tuberculosis bacteria, streptococcus and staphylococcus, toxoplasma. In addition, tick-borne encephalitis is a serious problem. This is a viral disease spread by certain types of ticks. The virus enters the body after an insect bite.
However, with tick-borne encephalitis the brain is not always affected; in 50% of cases the patient experiences only fever. Japanese encephalitis is also a viral species. The disease is very dangerous and in most cases is fatal. This type of encephalitis is characterized by a rapid course; a few days after infection, the patient falls into a coma. Herpes encephalitis is fatal in nine out of ten cases and has virtually no cure.
How does anti-receptor encephalitis manifest? Let's tell you in more detail.