Currently, more and more attention is being paid to how immunity affects various processes in our body. Disturbed immune responses discovered in new studies become the missing link in pathogenesis. This stimulates the search for new drugs and other preventive and therapeutic effects. In this text we will discuss the special immune status of the brain - its isolation from systemic immune processes. In addition, let's talk about disorders that violate the immune sovereignty of the central nervous system - autoimmune encephalitis.
Privileged body
The brain is an organ that is remarkable in many ways [1]. The infinite complexity of the device, its functionality and the connection between our lives and its state attract the attention of researchers to the brain. The relationship between the brain and the immune system of our body is also special: the brain is an immune-privileged organ. Immune reactions that easily develop in other tissues (liver cells, muscles, fatty tissue) rarely occur in the brain. Along with the brain, the thyroid gland, testicles and some eye tissues, in particular the cornea, found themselves in such a special relationship with the immune system.
In the minds of doctors in the second half of the twentieth century, the brain was a structure completely isolated from the immune processes of the rest of the body. At the beginning of the last century, Japanese scientists conducted experiments on implanting sarcoma cells (a malignant tumor of muscle tissue) into various organs of mice [2]. It turned out that when sarcoma cells are placed in brain tissue, the tumor actively develops, but when they are implanted under the skin of rodents or into muscle tissue, the tumor does not develop. The researchers suggested that the “center” (the brain) is isolated from the immune processes that successfully fought off the sarcoma “in the periphery” (other tissues). Further research only confirmed this conclusion. The brain, in the minds of scientists, has become a “clean zone” in which an immune response does not develop. In the 1950s, the term “immunological privilege” arose, coined by British scientists named Billingham and Boswell [3].
Overcoming barriers
It has long been believed that the basis of the immune privilege of the brain is the presence of the blood-brain barrier (BBB). The BBB is a complex of cellular and extracellular structures that separate the blood flowing in the capillaries from the neurons of the brain parenchyma. The cells of the vascular walls, the basement membrane on which they lie, and astrocytes participate in the formation of the BBB. The immune privilege of parts of the central nervous system was in good agreement with the extent of the BBB within it. The brain parenchyma is reliably protected by the BBB, and inflammatory processes (encephalitis) rarely occur in it. The choroid plexus, which produces cerebrospinal fluid, and the membranes of the brain do not have such cover, and their inflammation (choroiditis, meningitis) is much more common (Fig. 1).
Figure 1. Structure of the central nervous system. The parts that are well protected by the BBB include the gray and white matter. Other components do not have this protection.
[2]
There are cases in which even the BBB does not save the nervous system, and inflammation processes occur in the brain. However, it is important to answer the question for yourself: do they proceed in the same way as in the rest of the body? Maybe the brain has a special way of immune response, and immune privilege has additional explanations? In vitro, an immune response in tissues can be induced by injecting bacterial lipopolysaccharide (LPS). It is a structural component of the cell wall of gram-negative bacteria that triggers a cascade of immune reactions in our body. When studying the reaction of different body tissues to the introduction of LPS, it turned out that an immune response in the skin and choroid plexuses of the central nervous system occurs to the same dose of LPS [4]. This is logical, because in neither case is there special protection in the form of the BBB. At the same time, to cause an immune reaction in the brain parenchyma similar to that occurring in the skin, a dose 100 times greater than the “skin” dose is required. In this case, compartmentalization of the immune response occurs - predominantly the white matter (the processes of neurons) is affected, and not the gray matter (their bodies). This experience points to another explanation for immune privilege: the weakness of our brain's own, “intrinsic” immune response. The brain parenchyma turns out to be extremely passive in relation to bacterial invasion: the brain does not seem to want to notice foreign components inside itself. Next we will try to figure out what is the reason for this immune “inattention”.
Weak link
If we are talking about the weakness of the local immune response, then we need to figure out what is “broken” in it. This may be impaired recognition with the normal ability of immune cells to attack antigens (weakness of the afferent link). Another option: normal antigen recognition with impaired ability to attack it (weakness of the efferent link). Studies have shown that the efferent part of the brain is preserved and functions normally [2]. Then efforts were focused on searching for disorders in the afferent link. Over time, it became clear that the problem was in recognizing the antigen and further working with it (Fig. 2).
Figure 2. The immune response occurs in several stages. The formation of a reaction to an antigen occurs in two ways: information about the antigen is delivered to local lymph nodes in “liquid” (the antigens themselves) and “solid” form (previously activated cellular elements of the immune system). In an immune reaction outside the brain, both pathways operate. When the brain's immune system reacts to an antigen, cellular elements do not reach the local (cervical) lymph nodes. It is one of the main components of a weak immune response in the brain.
[2]
You can read more about these processes in the article “Immunity: the fight against strangers and... our own” [5].
The brain has difficulty delivering activated immune cells to the cervical lymph nodes. Dendritic cells are responsible for working with antigens in the brain. In other organs, they recognize the antigen and then provide information about it to T and B lymphocytes in the lymph nodes. During inflammation in the brain, this process does not occur: dendritic cells do not migrate to the lymph nodes and do not present antigen. The immune response becomes localized and is regulated by dendritic cells in the brain parenchyma. If in other organs the cellular elements of immunity, after the presentation of the antigen, rush to the site of bacterial penetration [6], then with the development of inflammation in the brain parenchyma this does not happen. The brain has to rely on itself. A similar locality of the immune response is observed in the parenchyma, but not in the choroid plexuses and meninges.
Immigrants in the brain
If we continue to describe the special immune status of the brain in our body, then it is necessary to say a few words about microglia. Microglia are the main cell type responsible for the innate immune response in the brain (Fig. 3) [7]. Microglia have phagocytic activity, are able to recognize microorganisms and contribute to the development of inflammatory reactions in the brain parenchyma, that is, they behave not like a neuron, but a real immune cell [8]. This is explained by the fact that microglia in our brain are of hematopoietic origin [9]. The precursors of microglia in the prenatal period are the “brothers” of all other immune cells that find themselves in the central nervous system. They did not lose their immune functions and began to carry them out locally. It turns out that microglial cells can be called emigrants of the immune system.
Clinical picture
The disease is characterized by a gradual onset. The following phases characteristic of encephalitis with antibodies to NMDA receptors are distinguished: prodromal, psychotic, areactive, hyperkinetic and a phase of gradual regression of symptoms.
The prodromal period lasts 5-7 days with the presence of ARVI-like symptoms (fever, headache, fatigue). The transition to the next stage (psychotic) is accompanied by the appearance of a number of neurological disorders, such as apathy, lack of emotions, depression, withdrawal, fear, short-term memory disorders, and difficulties in using electronic equipment. Auditory and visual hallucinations, as well as other schizophrenia-like symptoms, may occur.
14 days after the psychotic period, the areactive period begins, which is accompanied by a disturbance of consciousness, reminiscent of a catatonic state, mutism, akinesia, and lack of response to verbal commands with open eyes. A number of patients have been noted to have a violent grimace resembling a smile.
The appearance of hyperkinesis indicates the onset of a hyperkinetic period. The most characteristic manifestations are orolingual dyskinesia (lip licking, chewing), athetoid dyskinetic postures of the fingers. With complications, pretentious orofacial and limb dyskinesias appear, such as prolonged movements of the lower jaw, strong clenching of the teeth, dystonia of mouth opening, intermittent forced abduction or contraction of the eyeballs, hand movements reminiscent of dancing. Of particular danger is hypoventilation associated with the production of antibodies to the NR1 subunit of NMDA receptors.
Within two months, the disease shows a gradual regression of symptoms. Hyperkinetic disorders go away, and neuropsychiatric status improves.
Autoimmune encephalitis
After talking about the special immune status of the brain, we will move on to the topic of autoimmune encephalitis - a group of diseases that are associated with damage to the membrane and intracellular structures of neurons by the body’s own immunity. In modern practice, autoimmune encephalitis is rarely diagnosed. This is explained by the fact that the first cases were described in detail only in 2005 [10]. It can be assumed that there are actually more cases of this disease than are recorded by specialists. Some patients with autoimmune encephalitis may be diagnosed with other disorders, such as schizophrenia or infectious encephalitis. This is due to the fact that doctors have little knowledge about this disease. Doctors diagnose only those diseases that they know. The more arsenal of diagnoses a doctor has in stock, the more accurate the diagnosis and the more correct the treatment.
Autoimmune encephalitis can be divided into two groups:
- diseases caused by activated T cells (something similar occurs in multiple sclerosis [11]);
- diseases that occur when antibodies act on intra- and extracellular components of a neuron, such as ion channels.
The first group of autoimmune encephalitis is characterized by cell damage by antibodies and activated T lymphocytes [12]. These encephalitis are more severe and require intensive therapeutic interventions, unlike representatives of the second group.
In the second group of encephalitis, neuronal damage is only “superficial” in nature. The effect of specific antibodies on surface-located structures leads to the “contraction” of receptors (in English this is called capping) and their subsequent internalization (capture) into the cytoplasm (Fig. 3) [13]. In addition, autoantibodies themselves can bind to receptors, blocking their work [14].
Figure 3. The changes that occur in receptors in autoimmune encephalitis are similar to the changes in synapses in myasthenia gravis. Normally (left side of the figure), the receptors are free and easily interact with the neurotransmitter acetylcholine. In case of illness, antibodies begin to affect the receptors, and their ability to bind to the neurotransmitter is impaired. The “clumped” acetylcholine receptors are gradually drawn into the cytoplasm, where they are destroyed.
www.memorangapp.com
Antibodies penetrate from the outside, from outside the BBB, or are produced by brain-infiltrated and activated B-lymphocytes [15]. In cases where antibodies are directed against intracellular structures, the attack on neurons is led by cytotoxic T lymphocytes. With the help of perforin and granzyme B, they damage the membrane of neurons, which leads to their death [16], [17]. The GEB, which we talked about above, in this light appears to be a reliable fortress wall protecting a quiet city that is no longer used to fighting. If a gap appears in the wall, the city will quickly fall: the nerve cells will be too sensitive to the effects of immune factors.
Looking for flags
Signs of autoimmune encephalitis are very varied, but three types of symptoms can be distinguished.
- Psychiatric symptoms: psychosis, aggressive actions, sexual disinhibition, panic attacks, obsessive actions, feelings of euphoria or fear.
- Motor symptoms: increased muscle tone and unevenness, muscle twitching and repetitive movements of the limbs.
- Seizures: generalized epileptic seizures, status epilepticus.
The initial manifestations of autoimmune encephalitis may be symptoms of a mental disorder: memory impairment, hallucinations or the appearance of delusional ideas. For example, with autoimmune damage to glutamate NMDA receptors, 80% of patients showed symptoms of mental illness, and more than 60% were initially hospitalized in psychiatric departments [18], [19]. Psychiatrists must be able to identify patients with autoimmune encephalitis or at least suspect this disease in order to promptly send the patient for appropriate examinations and consultations with other doctors.
Among the variety of symptoms that can be caused by different reasons, it is easy to get lost. The doctor needs at least rough guidelines to suspect the diagnosis of autoimmune encephalitis. As a result of the analysis of many cases of the disease, signs were identified that most likely indicate this diagnosis - the so-called “red flags” of autoimmune encephalitis [20]. These include:
- Lymphocytic pleocytosis or the appearance of oligoclonal bands on CSF electrophoresis.
- Epileptic seizures.
- Faciobrachial dystonic seizures.
- Suspicion of neuroleptic malignant syndrome.
- Abnormalities on MRI.
- EEG abnormalities.
In addition, the researchers also identified “yellow flags” - signs that should alert the doctor and make him think about a possible diagnosis of autoimmune encephalitis [20]. Yellow flags for autoimmune encephalitis are:
- Reduced level of consciousness.
- Violation of posture and movements.
- Instability of the autonomic nervous system.
- Focal neurological symptoms.
- Speech disorders (aphasia and dysarthria).
- Rapid progression of psychosis, despite treatment.
- Hyponatremia.
- Catatonia.
- Headache.
- The presence of other autoimmune diseases, including thyroiditis.
If a doctor sees symptoms from the group of “red flags” in a patient, the study authors recommend testing for specific autoantibodies for the timely diagnosis of autoimmune encephalitis. If a patient has symptoms from the list of “yellow flags,” the doctor should suspect the possibility of such a diagnosis and examine the patient more carefully to look for more reliable signs of autoimmune encephalitis.
Additional Arguments
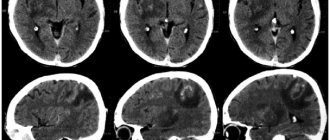
In addition to the combination of previously described symptoms, the diagnosis of autoimmune encephalitis must be confirmed by laboratory tests and other diagnostic procedures [21].
For example, you can test for antibodies to specific receptors. In autoimmune encephalitis that affects glutamate NMDA receptors, an increase in the titer of antibodies to them can be detected. Interestingly, in encephalitis the amount of immunoglobulins of class G increases, and in schizophrenia - classes A and M [22]. Currently, a correspondence has been established between antibodies that affect specific neuron structures and the symptoms of encephalitis (Table 1). Magnetic resonance imaging (MRI) may show changes in brain structure, and electroencephalography (EEG) may show abnormal brain function in the case of autoimmune encephalitis. Table 1. Correspondence of symptoms and autoantibodies in autoimmune encephalitis [20]
| Structure to which an antibody is produced | Psychiatric symptoms | Other symptoms | Typical patient |
| NMDA receptor | Psychosis, schizophrenia-like disorders, catatonia, aggression | Epileptic seizures, dyskinesia, autonomic instability, speech and consciousness disorders | Young women, common association with ovarian teratoma |
| Caspr2 | Insomnia, panic attacks, depression, schizophrenia-like disorders | Morvan's syndrome, neuromyotonia, muscle spasms, fasciculations | Middle-aged and older patients, possible connection with thymoma |
| LGI1 | Amnesia and other memory impairments, confusion, depression | Limbic encephalitis, faciobrachial dystonic seizures, hyponatremia | Middle-aged and older patients, male to female ratio 2:1, possible association with thymoma |
| Glycine receptor | Behavioral changes, schizophrenia-like syndrome | Tight muscle syndrome, progressive encephalomyelitis with rigidity, myoclonus, hyperekplexia | Middle-aged and older patients, possible association with thymoma and lymphoma |
| Synaptic antigens (GAD) | Schizophrenia-like syndrome, autism, attention deficit hyperactivity disorder | Limbic encephalitis, stiff muscle syndrome, seizures, brainstem dysfunction, ataxia | Middle-aged and older patients, possible association with small cell lung cancer |
| Onconeural antigens (Yo, Hu, CV2, Ri, Ma2) | Behavioral disorders | Limbic encephalitis, cerebellar degeneration, sensory neuropathy | Elderly patients, often with malignant tumors |
In some cases, autoimmune damage to the central nervous system is caused by the development of paraneoplastic syndrome, which may accompany the appearance of a malignant tumor in the body. In paraneoplastic syndrome, the tumor can begin to independently produce hormones and hormone-like substances, disrupting the regulation of various processes in the body. In addition, paraneoplastic syndrome can manifest itself in the form of an autoimmune disease, for example, autoimmune encephalitis.
The pathogenesis of autoimmune encephalitis within the paraneoplastic syndrome is as follows. In a malignant tumor of a certain tissue, genes that are typical for it are expressed, as well as genes that are usually “silent” in it. Among the “silent” genes there may be those that are normally expressed only in the brain, under the protection of the BBB. Therefore, the resulting proteins are called cancer-neuronal antigens. During the maturation of the immune system, it becomes familiar with almost all the proteins of the body, but these proteins are hidden from it and, accordingly, are perceived as foreign. From the point of view of our immunity, there is no difference between them and bacterial antigens. The tumor begins to produce cancer-neuronal antigens, and the immune system recognizes them and produces autoantibodies specific to them. Through minimal gaps in the BBB, autoantibodies penetrate the central nervous system and begin to attack neurons [14].
For this reason, when diagnosing autoimmune encephalitis, special attention is paid to searching for a tumor in the patient’s body. Removal of the tumor in cases of paraneoplastic origin of autoimmune encephalitis will lead to a significant improvement in the patient's condition. While the tumor is in the human body, antibodies continue to be produced, and the patient’s condition worsens.
A blow to the immune system
Steroids and immunoglobulins administered intravenously are used as first-line drugs for the treatment of autoimmune encephalitis. Steroids have a powerful anti-inflammatory effect. They are capable of suppressing immune responses at a variety of levels. The use of steroids leads to a decrease in the synthesis of inflammatory mediators and stabilization of lysosome membranes that secrete inflammatory factors. In addition, under the influence of steroid hormones, the migration of monocytes decreases. Plasmapheresis, which cleanses the blood of “extra” antibodies, can also help.
If first-line therapy does not work, then switch to the use of rituximab and cyclophosphamide. Rituximab is a monoclonal antibody against the CD20 receptor, which is found on the surface of B lymphocytes [23]. B lymphocytes produce a variety of antibodies, including autoantibodies against nerve cells, and their destruction can lead to improvement. The CD20 receptor appears on the surface of normal B-lymphocytes and B-lymphocytes that have undergone the process of malignancy (malignancy). Due to this property, rituximab is effective in autoimmune diseases and B-cell lymphomas. The drug binds to the CD20 receptor on the surface of the lymphocyte and enables other components of the immune system to destroy the cell.
Cyclophosphamide has an immunosuppressive effect and is able to suppress the body's excessive immune response. After passing through the liver, cyclophosphamide is converted into several active metabolites that penetrate the cell and tightly connect the two strands of DNA. This prevents tumor cells or other rapidly dividing cells (such as B and T lymphocytes) from dividing. For this reason, cyclophosphamide is included in the treatment regimen for some autoimmune diseases. The subtlety of using steroids, cyclophosphamide and rituximab for autoimmune encephalitis is that these drugs can complicate the diagnosis of those tumors that are associated with the appearance of autoantibodies. In case of lymphoma, the use of these drugs can temporarily improve the condition, but when discontinued, the tumor will again “take up the old ways” and produce autoantibodies. Although lymphoma is not so often complicated by autoimmune encephalitis, this feature must be taken into account during therapy.
Using autoimmune encephalitis as an example, we can consider two of the most important trends in modern medicine. The first trend is the study of the influence of immune processes on the functioning of the human nervous system and attempts to intervene in this process in the treatment of neurological and mental diseases. We are now close to understanding that the brain is not just an electrochemical laboratory under the skull, but also a special immune world with its own rules. It is in our interests to learn these rules and begin to play by them to our advantage. The second trend is the biologization of psychiatry, the search for specific biological changes in the body that lead to mental health problems. Psychiatry is a part of medicine, a large branch where theoretical knowledge and its practical application are combined. Without a biological basis, medicine will cease to be scientific. If you ignore biological laws and knowledge within one of the medical specialties, then the same thing will happen to it. Psychiatry must become biological in order to remain scientific and fulfill its medical goals.
New Horizons
Recently, researchers and doctors have been paying more and more attention to innate immune responses during the development of neurodegenerative diseases (Alzheimer’s disease [24], Parkinson’s disease [25], Huntington’s chorea [26]) and mental disorders [27]. The accumulation of beta-amyloid, which itself is most likely involved in the immune responses of the central nervous system [28], is associated with an imbalance between its accumulation and elimination (removal). The latter process depends in part on how toll-like receptor 2 (TLR2) is expressed [29]. Mouse models have shown that the lower the level of TLR2 expression, the worse the removal of beta-amyloid [30]. Decreased elimination of beta-amyloid leads to its accumulation in nerve cells and subsequent disruption of their function and death. Studying the internal immune processes of the brain can become the basis for the search for new drugs for neurodegenerative diseases. Pharmaceutical companies are now testing monoclonal antibodies to treat Alzheimer's disease, but success remains modest.
Etiology
The exact cause of the disease is currently unclear. Often the pathology is diagnosed in young women against the background of concomitant diseases such as ovarian teratoma, schizophrenia, catatonia, and drug addiction. It is also worth noting that in more rare cases, the disease debuts with severe short-term memory impairment, reminiscent of limbic encephalopathy. Recently, the disease has been increasingly diagnosed in children and adolescents: a 2009 study found that out of 81 people, 32 (40%) were under 18 years of age, with younger and male patients more likely to have no tumors.
Alternative names
Names used in the literature to describe the complex of symptoms before the discovery of the connection with the NMDA receptor:
- acute diffuse lymphocytic meningoencephalitis - English. acute diffuse lymphocytic meningoencephalitis
- acute transient limbic encephalitis acute reversible limbic encephalitis
- acute early female nonherpetic encephalitis - English. acute juvenile female nonherpetic encephalitis
- acute non-herpetic encephalitis of young people - English. juvenile acute nonherpetic encephalitis
Treatment
Treatment of this disease involves both influencing the pathogenesis of the disease and treating individual syndromes. Pathogenetic therapy includes the administration of glucocorticosteroids and intravenous immunoglobulins. It is possible to use monoclonal antibodies (rituximab), plasmapheresis or cytostatics (azathioprine).
Phenobarbital and clonazepam are used to treat seizures, and antipsychotics are used to control dyskinesias.
Another important aspect in the treatment of encephalitis with antibodies to NMDA receptors is the early removal of the tumor as a source that triggers the production of antibodies that cross-damage nervous tissue.
Since the symptoms of anti-NMDA receptor encephalitis and herpetic encephalitis are very similar, many patients received acyclovir before a final diagnosis was made.
Example of a disease
Brief description of a clinical case from the abstract of an article in the journal Nature Clinical Practice Neurology, 2007:
A 34-year-old woman consulted doctors about headache, fever and anxiety. These symptoms were soon followed by ideas of harm, aggressive agitation, seizures, hypoventilation, hyperthermia, and severe autonomic instability requiring intubation and sedation. Episodes of hypotension and bradycardia developed with asystolic periods of up to 15 seconds. When sedatives are withdrawn, the eyes open without reacting to external stimuli. Muscular rigor, frequent facial grimaces, rhythmic contractions of the abdominal muscles, kicking movements of the legs, and intermittent dystonic postures of the right hand were noted.