YES.
Kuzhel, G.V. Matyushin, T.D. Fedorova E.A., Savchenko, T.M. Zadoenko KGUZ "Krasnoyarsk Regional Hospital No. 2" GOUVPO "Krasnoyarsk State Medical Academy"
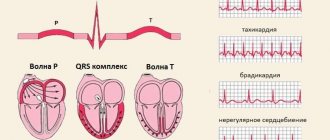
An electrocardiogram in 12 standard leads is the method of choice in the diagnosis of acute myocardial infarction (AMI). Quick and accurate diagnosis of AMI is vital, as it makes it possible to immediately begin reperfusion therapy, which reduces the area of necrosis and improves the patient's prognosis. One of the generally accepted criteria for myocardial infarction is ST segment elevation in two or more anatomically adjacent leads [10]. The importance of timely identification of ST segment elevation associated with AMI is emphasized by the fact that neither ST segment depression nor increased biochemical markers of cardiac necrosis (MCN) in the blood serum are indications for thrombolytic therapy [4, 9].
In the early stages of AMI, diagnosis can be significantly difficult, since the ECG is often normal or has minimal abnormalities. Moreover, only half of patients with AMI have obvious diagnostic changes on the first ECG. At the same time, approximately 10% of patients with proven AMI (based on clinical data and positive MCI) will not develop typical changes on the ECG, such as ST segment elevation or depression [4]. However, in most cases, serial ECGs in individuals with AMI show a characteristic evolution that usually corresponds to the typical changes observed in myocardial infarction. In the domestic school of cardiology, it is customary to distinguish four stages of the course of AMI [1].
I.
The most acute stage
. In this stage, which lasts from several hours to several days, changes in the ECG affect only the ST segment and the T wave. The earliest signs of acute myocardial infarction are difficult to distinguish and usually include an increase in the amplitude of the T wave in the affected area, which becomes symmetrical and directional ( hyperacute). Typically, hyperacute T waves are most evident in the anterior precordial leads and are most noticeable when an older ECG is available for comparison. Changes in T wave amplitude can be observed within a few minutes of the onset of infarction and are accompanied by corresponding changes in the ST segment. The optimal time for delivery of a patient to a medical facility is considered to be an interval of up to four hours from the onset of AMI. Unfortunately, ECG changes in the acute stage of myocardial infarction are often not properly assessed, which significantly increases the time it takes for the patient to be delivered to a specialized facility and prolongs the start of reperfusion therapy.
II. Acute stage.
In the acute stage, which usually lasts up to one week, ST segment elevation is recorded and Q waves begin to form. In practice, ST segment elevation is often the earliest sign of AMI and usually becomes noticeable within a few hours from the onset of symptoms. At the initial stages, the angle between the T wave and the ST segment, characteristic of a normal ECG, is lost. The T wave becomes wide and the ST segment rises, losing its normal concavity. During further ascent, the ST segment becomes convex upward. The degree of ST segment elevation varies between small changes of less than 1 mm to pronounced elevation of more than 10 mm. Sometimes the QRS complex, ST segment and T wave merge, forming the so-called monophasic curve.
III. Subacute stage.
The subacute stage of myocardial infarction lasts up to several weeks. During this stage, the ST segment begins to approach the isoline, and negative T waves are formed. In the case of transmural myocardial infarction, the necrosis process is accompanied by changes in the QRS complex, which include a decrease in the amplitude of the R waves and the development of pathological Q waves. Such changes develop as a result of the loss of viable myocardium under recording electrode, therefore Q waves are the only ECG criterion that verifies myocardial necrosis. Q waves can develop within 1 to 2 hours of the onset of AMI symptoms, although this often takes 12 to 24 hours. The presence of pathological Q waves, however, does not necessarily indicate a completed infarction. If ST segment elevation and Q waves are detected on the ECG and the chest pain is of recent onset, the patient may still benefit from thrombolysis or interventional therapy.
IV. Scar stage.
Consolidation of scar tissue ends on average 8 weeks after myocardial infarction. At this stage, the ST segment reverts to the isoline and the amplitude of negative T waves decreases. In the case of extensive myocardial infarction, pathological Q waves are a stable marker of cardiac necrosis. In small infarcts, scar tissue may include viable myocardium, which may reduce the size of the electrically inert region and even cause the eventual disappearance of Q waves.
One of the curious features of the ECG in AMI is the so-called pseudonormalization phenomenon. Wilson's theory of the formation of Q waves implies the formation of a so-called electrical window in case of necrosis, through which the recording electrode records the electrical potentials of the opposite wall. However, despite necrosis, some of the myocardial fibers in the infarction zone remain viable, which explains the characteristic flattening of Q waves during myocardial infarction. However, the potentials of these fibers remain hidden behind the powerful electric vector of the opposite wall. With a repeated infarction, which involves the opposite wall, this vector is significantly reduced, which, in turn, makes it possible to record the potentials of myocardial fibers in the area of the old scar. As a result, in the area of the old scar with pathological Q waves (for example, in the anterior wall), in the event of a re-infarction of the opposite wall (for example, the posterior wall), R waves begin to be recorded. Thus, the registration of R waves in the area where pathological Q waves were previously observed, strongly suggests the formation of an infarction in the opposite wall.
Dynamics of changes in the ST segment and T wave in AMI
The ECG picture during myocardial infarction has its own characteristic development. Firstly, ST segment elevation, as a rule, leads to the formation of Q waves. Secondly, the formation of negative T waves occurs against the background of a characteristic arcuate ST segment elevation.
ST segment elevation associated with myocardial infarction in the anterior wall can persist for a long time if dyskinesia or left ventricular (LV) aneurysm develops. Negative T waves can also persist for a long period and sometimes remain a permanent sign of myocardial infarction. It should be noted that the absence of formation or “restoration” of pre-inverted T waves in the acute stage of myocardial infarction strongly suggests the development of post-infarction pericarditis [11].
T wave changes in ischemic heart disease
With ischemic heart disease, the T wave can be changed in two situations.
- With ischemia associated with an attack of angina, a negative T wave may be recorded in two (or more than two) adjacent leads.
- In the acute phase of myocardial infarction with ST elevation, a high positive T may be recorded.
Look at ECG 5 with an example of ischemia and inverted T waves.
ECG 5. Negative T waves in myocardial ischemia
ECG source.
ECG 5 shows inverted T waves in the left leads: V5-V6, I, aVL.
Negative T values indicate ischemia if the following conditions are met.
- The depth of negative T must be at least 1 mm.
- Negative T waves must be recorded in at least two adjacent leads.
- The QRS complex before the negative T has a tall positive R wave.
- Dynamics of change. These should be “new” inverted Ts (they should not be on old cardiograms). Within some time (hours or days) there should be a return of the T wave to the isoline.
In addition, it should be remembered that inverted T wave in leads III, aVR, V1 is a normal variant.
ECG 6 shows another example of a change in the T wave in coronary artery disease: high coronary T wave in the acute phase of myocardial infarction with ST elevation. This is the initial and very short period of a heart attack, so it is not always possible to register it on an ECG.
ECG 6. High positive T wave in the acute phase of myocardial infarction
ECG source.
Reciprocal ST segment depression
ST segment depression in leads opposite the affected area, otherwise known as reciprocal depression, is a highly sensitive indicator of AMI. The pathogenesis of reciprocal changes remains unknown. Reciprocal changes have high sensitivity and a positive predictive value of up to 90% and are observed in approximately 70% of lower and up to 30% of infarcts involving the anterior wall of the LV, although, of course, their absence does not exclude the diagnosis of AMI [4, 5]. As a rule, ST segment depression is horizontal or oblique. The presence of reciprocal changes is especially important when there is doubt about the clinical significance of the recorded ST segment elevation. We especially note that reciprocal changes may be the only sign of AMI against the background of still unobvious ST segment elevation. Similar situations often occur in cases of myocardial infarction with damage to the lower wall. The presence of severe ST segment depression in the precordial leads against a background of normal heart rate or bradycardia in a patient with an ischemic painful attack strongly requires the exclusion of AMI.
Symptoms of depression of the ischemic segment
ST segment depression (what is it, people often ask) leads to the appearance of coronary artery disease. It is difficult to recognize based on clinical symptoms. Detection of pathology is rarely observed during a medical examination. The main symptom is pain that occurs behind the sternum, where the source of pain is located.
Additional visual characteristics of the diagnosis include: cold sweat, bluish skin, rapid breathing, and muscle fatigue.
To assess the ability of the heart muscles to respond to an increase in heart rate, it is necessary to do tests with physical activity.
When a person is healthy, he has no pathologies, since the heart reacts adequately to a possible increase in load. During physical activity, arterial hypertension decreases, and sometimes there is an increase in systolic pressure.
After a patient has suffered a myocardial infarction, the cause of low blood pressure is myocardial ischemia. When the heart beats are repeated abnormally frequently, reduced cardiac functionality is evidence of ventricular dysfunction. This situation occurs when cardiotropic drugs are used.
Myocardial infarction of the anterior wall
Anteroseptal ST-segment elevation infarction in leads V1-V3 is a highly accurate indicator of left anterior descending coronary artery (LADCA) involvement. ST segment elevation in these three leads and in lead aVL, combined with ST segment depression of more than one mm in lead aVF, indicates occlusion of the proximal segment of the LCA. ST-segment elevation in leads V1, V2, and V3 without significant ST-segment depression in the inferior leads suggests occlusion of the LCA after origin of the first diagonal branch.
In some cases, the LPNCA wraps around the apex of the LV and supplies blood to the apical parts of the inferior wall in the distal part of the posterior interventricular groove. Rarely, the LCA extends along the entire length of the posterior sulcus, replacing the posterior descending artery. In the case of ST segment elevation in leads V1, V2 and V3 with ST elevation in the inferior leads, occlusion of the LCA of the distal origin of the first diagonal branch, in the area that irrigates the inferoapical parts of the LV, can be assumed [7].
Lower IM
AMI with isolated ST-segment elevation in leads II, III, and aVF is usually associated with damage to the right coronary artery (RCA) or the distal circumflex artery (CA). A rather unpleasant feature of AMI with damage to the inferior wall is that the ST segment elevation associated with the infarction can develop over a long period, up to two weeks, to become evident on the ECG [4]. The inferior wall can be supplied with blood from the right coronary artery (in 80% of cases) or from the OA, which is a branch of the left coronary artery.
ST segment elevation in lead III is greater than in lead II, and ST segment depression of more than one mm in leads I and aVL suggests damage to the RCA, which supplies the inferior wall. In the case of blood supply to the lower wall from the OA, the rise of the ST segment in lead III does not exceed the rise in lead II. In this case, either an elevation of the ST segment in aVL is observed, or it is located on the isoline [6, 7].
Signs of ischemia on the ECG
Highly probable signs of “pre-scar” cardiac ischemia are ST segment displacements: this is characterized by a rise (elevation) and a decrease (depression). Holter monitoring records these changes as follows: the ST trend deviates from the zero “beard” and “peak” level.
All layers of the myocardium die and on the ECG this fact is reflected by the Q wave (it will be wide, with an amplitude of more than a quarter of the height of the R wave in the same direction).
ST elevation and the presence of Q are included in the diagnosis formulations: acute myocardial ischemia with ST segment elevation, as well as Q-forming infarction. There may be other causes of ST segment depression on the ECG.
Such ST elevation also occurs in other conditions.
Early repolarization syndrome is characterized by the appearance of a notch on the descending limb of the R wave. This condition is fixed on the halter for quite a long time.
Also, pericarditis with changes in almost all leads cannot be ruled out.
ST depression on the ECG (we are looking into what it is) may be associated with an overdose of glycosides, but will differ in a different segment shape, in this case it resembles a “trough”.
All other changes in the QRS complex are considered possible. This means that they are not diagnosed. Most often this is manifested by a negative T wave.
If a patient has acute chest pain and any changes on the ECG, you need to remember a simple rule - he should be hospitalized without fail. Even if he doesn't have a heart attack. It’s worse not to do this, and the person will die.
Right ventricular myocardial infarction
Right ventricular MI is usually associated with occlusion at the level of the proximal RCA. The most sensitive ECG sign of right ventricular MI is ST segment elevation of more than one mm in lead V4R with a positive T wave in this lead [5]. This sign is rarely observed more than 12 hours after AMI, so right leads should be recorded as soon as possible in all patients with inferior wall infarction. On a standard 12-lead ECG, signs of AMI involving the right ventricle are ST segment elevation in lead V1 combined with ST segment elevation in leads II, III, and aVF (STIII greater than STII).
Right ventricular infarction is often missed because the standard 12-lead ECG does not have high sensitivity for right ventricular infarction. At the same time, the diagnosis of right ventricular infarction is important, as it may be associated with a state of hypotension caused by treatment with nitrates or diuretics. At the same time, in contrast to cardiogenic shock, which requires differential diagnosis, the patient responds well to fluid administration.
In approximately 40% of cases, inferior wall AMI is complicated by right ventricular infarction [2, 6]. Less commonly, right ventricular infarction is associated with occlusion of the circumflex artery and, if this branch is dominant, may be associated with inferolateral infarction. Right ventricular infarction can complicate anterior wall AMI and can rarely occur as an isolated phenomenon [15].
Depression
Atherosclerosis
Thyrotoxicosis
Rheumatism
Arthritis
Gastritis
18820 January 30
IMPORTANT!
The information in this section cannot be used for self-diagnosis and self-treatment.
In case of pain or other exacerbation of the disease, diagnostic tests should be prescribed only by the attending physician. To make a diagnosis and properly prescribe treatment, you should contact your doctor. Depression is one of the most common mental disorders.
The criteria for a depressive episode are a daily decrease in mood that occupies most of the day, significantly different from the person’s usual state, for two weeks or more, an obvious decrease in interest and pleasure in activities usually associated with positive emotions, increased fatigue and motor retardation.
To the above symptoms you can add the following:
- decreased attention;
- loss of appetite;
- insomnia;
- decreased self-esteem;
- thoughts about one's own guilt;
- suicidal thoughts.
Types of depression
- Psychogenic depression develops as a reaction to traumatic events.
- Endogenous depression is caused by changes in the levels of hormones and neurotransmitters.
- Exogenous depression occurs with various somatic diseases, as a result of brain damage and with the use of psychoactive substances.
- Hidden (“masked”) depression manifests itself in the form of a somatic illness.
Causes of depression
The greatest difficulty is in diagnosing hidden, otherwise latent, depression.
When diagnosing it, it is important to exclude the presence of any organic diseases. After all, such depression has many manifestations, with which patients turn to general practitioners, cardiologists, neurologists, etc. However, examinations do not reveal any organic pathologies.
The most common form of such depression is cardiac. Patients feel excruciating pain in the heart area, palpitations, weakness, dizziness, but when undergoing a cardiac examination, no abnormalities are detected.
The abdominal variant is also common, in which pain occurs in any part of the abdomen, nausea, and loss of appetite.
The skin variant is characterized by redness and changes in skin sensitivity, the appearance of eczematous rashes, increased sweating, itching, often local (for example, itching of only the palms or legs).
The causes of the development of exogenous depression can be traumatic brain injuries, neuroinfections, tumor and vascular diseases of the brain (atherosclerosis, strokes and cerebral infarctions), and atrophic processes.
Psychogenic depression occurs after exposure to psychological trauma, which is an individually significant stressful event.
Endogenous depression occurs as an independent disease, and can also accompany bipolar disorder, which is characterized by alternating phases of mania, depression and mental stability.
There are frequent cases of depressive disorders in people who use psychoactive substances and alcohol.
Somatic diseases that can lead to depression are divided into groups.
- Cardiac pathologies: myocardial infarction, arterial hypertension, chronic heart failure, arrhythmias.
- Endocrine disorders: diabetes mellitus, hypo- and hyperthyroidism.
- Gastrointestinal disorders: liver cirrhosis, colitis, etc., leading to impaired absorption and detoxification of harmful substances.
- Rheumatic diseases: rheumatism, systemic connective tissue lesions, arthritis, etc. are accompanied by severe pain and require long-term treatment.
- Neoplasms, especially malignant ones.
Postpartum depression is worth considering separately.
The development of this condition is facilitated by features of the postpartum period: hormonal changes in the body occur (the concentration of female sex hormones decreases), and the volume of circulating blood decreases.
Deterioration in health after childbirth, problems with breastfeeding, and changes in appearance have a significant impact. Depression develops in 10% of primiparous women from the 2nd to the 6th month after birth and is manifested by symptoms characteristic of all depression: motor retardation, worsening mood, tearfulness, changes in appetite. A feature of postnatal depression is a decrease in a woman’s interest in the child, irritation from the need to care for him. It is very important to diagnose this condition in a timely manner and undergo a course of treatment, since it is the child who suffers first.
Which doctors should I consult if I have depression?
In most cases, with depression, they seek help from a doctor, , , , depending on the cause of the complaints. Many patients avoid seeking help from a psychiatrist or psychologist. However, specialists in the field of psychiatry and psychology not only diagnose the causes of depression, but also help to cope with the depressive state.
Diagnosis of depression
A doctor of any specialty can suspect depression. However, diagnosis of depression is possible only by a psychiatrist who will conduct a survey and analyze the data obtained. To exclude organic pathology in masked and exogenous depression, depending on the symptoms, the doctor may prescribe a set of laboratory and instrumental examinations:
- clinical blood test;
Myocardial infarction of the posterior wall
The posterior descending coronary artery (PDCA), which supplies blood to the posterobasal sections, can be a branch of the RCA (in 85-90% of cases) or a branch of the OA (12), which determines the right or left type of coronary circulation. The diagnosis of AMI with posterior-basal lesions is often difficult when using a standard 12-lead ECG, while early detection of coronary thrombosis is very important from the point of view of prescribing thrombolytic therapy.
Changes in the ECG during AMI of the posterior basal sections are indirectly manifested in the anterior precordial leads. Leads V1-V3 record the potentials of not only the anterior, but also the opposite (posterior) wall, and changes in blood supply in this area are reflected in these leads. Typically, there is an increase in R waves that become wider and more dominant, as well as ST segment depression and high amplitude T waves pointing toward the posterior wall [3]. The use of leads V7-V9, recording posterobasal potentials, will show ST segment elevation in patients with AMI.
These additional leads provide valuable information and help in identifying patients who may benefit from urgent invasive therapy. In any case, registration of ST segment depression in leads V1-V2 should serve as a reason to exclude AMI of the posterobasal parts of the LV. In the cicatricial stage, a previous myocardial infarction in the posterior-basal sections will be indicated by the ratios R/S > 1 in lead V2 and RV2 > RV6, recorded against the background of the horizontal position of the electrical axis of the heart [2].
Lateral wall infarction.
Lesions in the proximal circumflex artery are often associated with lateral infarction and changes in leads I, aVL, V5-V6. Often, AMI can manifest itself as changes that occur isolated in lead aVL. In such cases, it is customary to diagnose AMI with damage to the high lateral parts of the LV [3].
ST SEGMENT DYNAMICS IN HEALTHY PEOPLE
Normal values during Holter recording of an electrocardiogram (ECG) are the most difficult and often controversial values. Also Norman. Holter noted that significant electrocardiographic changes can be detected during normal life in clinically healthy individuals [4]. The same results may have different diagnostic significance depending on age and gender [3]. Analysis of the ST segment is necessary primarily in the diagnosis of myocardial ischemia, including painless ones. However, the morphology of the ST segment depends on many factors [1,2], and not just on insufficient blood supply to the myocardium. The question of the diagnostic significance of ST segment changes in practically healthy individuals has been little studied. Purpose of the study. To study the dynamics of the ST segment in practically healthy people over 50 years old according to Holter monitoring. Materials and methods of research. The study included 30 apparently healthy volunteers (15 men and 15 women) aged from 51 to 74 years, average age - 54.71.14 years. The average age of men and women did not differ significantly. Inclusion criteria: no complaints; normal blood pressure, resting ECG and chest fluorography data; absence of pathological findings during physical examination. Exclusion criteria: chronic diseases of the cardiovascular system, respiratory and digestive organs; bad habits (alcoholism, smoking); taking medications at the time of the study; obesity. Holter monitoring was carried out using the MYOCARD-HOLTER system in 3 leads (V2, V5, and VF) for 24 hours. The maximum depression and elevation of the ST segment, the duration of episodes of depression and elevation, and possible reasons for the deviation of the segment from the isoline were assessed. Research results and discussion. In 2 (6.67%) cases, the automatic analysis of maximum ST segment depression was erroneous due to the presence of interference. In most cases – 18 (64.29%) the maximum depression was less than 1 mm, in 10 (35.71%) the degree of depression was ≥1 mm. The incidence of ST segment depression ≥1 mm was similar in men and women. All episodes lasted less than 1 minute, that is, they were of a nonspecific nature, which is consistent with literature data. A. Dabrowski et al. note that ST segment depression of more than 1 mm is recorded in 30-40% of healthy patients [1]. The greatest depression of the ST segment was observed in leads V5 and a VF and amounted to 0.76±0.08 (from 0.2 to 1.8) mm and 0.76±0.07 (from 0.2 to 1.5) mm, respectively , which exceeded the indicator in lead V2 by 0.43 mm (56.58%) (P In women, the degree of depression was 0.36 mm (38.71%) more pronounced (P
Table 1
Maximum ST segment depression in apparently healthy patients over 50 years of age (mm) (M ± m)
| Leads | Men(n=15) | 5) | ||
| Depression | HR/min | Depression HR/min | ||
| V2 | 0,35±0,09 | 91,50±10,50 | 0,32±0,06 94 | ,54±4,03 |
| V5 | 0,57±0,12 | 100,58±8,26 | 0,93±0,11 11 R | 9,93±5,19 R |
| AVF | 0,74±0,13 | 93,71±6,57 | 0,78±0,06 10 | 7,29±4,09 |
Note. P - error in the reliability of differences in comparison with the indicator for men.
According to the literature, ST depression is detected in women 30 times more often than in men: in 0.8% of monitoring cases in men and in 30% of cases in women [1]. The reasons are: the influence of the autonomic nervous system - depression of the ST segment occurs as a manifestation of hypersympathicotonia, more often in women (18% of women and 1% of men) with concomitant tachycardia, without typical anginal pain, during physical activity - which is most often associated with tachycardia. When analyzing the maximum ST segment elevation, it turned out that in 2 (6.67%) cases the automatic analysis was also erroneous due to the presence of interference. Episodes of ST segment elevation were recorded in 18 (64.28%) patients, 57.15% more often in men (92.86 vs. 35.71%) (P The greatest elevation was observed in leads V2 and V5 - 0.98±0, 07 (from 0.5 to 1.7) mm and 0.92±0.09 (from 0.3 to 1.9) mm with a heart rate of 83.26±2.86 (from 66 to 110) per minute and 72.89 ±2.96(from 51 to 95) per minute. According to the literature, significant elevation of the ST segment (more than 1 mm) is recorded from 0 to 60% of healthy individuals, more often in young people [1, 3]. Table 2
Maximum ST segment elevation in apparently healthy patients over 50 years of age (mm) (M ± m)
| Leads | Men(n=15) | Women(n=15) | ||
| Elevation | Heart rate | Elevation. | Heart rate | |
| V2 | 1,18±0,08 P | 85,00±4,07 | 0,75±0,05 | 81,38±4,12 |
| V5 | 1,12±0,15 P | 70,92±3,71 | 0,74±0,08 | 74,86±4,70 |
| and VF | 0,89±0,13 P | 73,46±3,73 | 0,52±0,07 | 82,08±5,27 |
Note. P is the error in the significance of differences in comparison with the indicator in women.
In most cases (57-100%) episodes were recorded during wakefulness with normal heart rate. In 7 (25%) patients, elevation was caused by early left ventricular repolarization syndrome, which occurred in men and women with the same frequency - in 3 (21.43%) and 4 (28.57%), respectively. In other cases, elevation was due to vagotonia (recorded at rest) and/or positional changes. In men, the degree of elevation in all leads was greater than in women: in lead V2 - by 0.43 mm (36.44%) (P The data obtained are consistent with literature data. Normally, ST segment elevation in leads from the extremities to 1 is acceptable mm, in precordial leads V1–V2 up to 2–3 mm [3].Patients with vegetative-vascular dystonia are especially prone to this, in whom ST segment elevation during a Holter study is recorded 10 times more often than in the control group of patients [1]. Conclusions 1. In healthy people over the age of 50 years with CM, episodes of ST segment depression of more than 1 mm and lasting less than 1 minute were recorded in 35.71% of cases, episodes of elevation of more than 1 mm and lasting more than 1 minute were recorded in 64.28%. 2. Depression of the oblique type, recorded mainly in leads V5 and a VF, more pronounced in women and caused by sympathicotonia 3. Elevations of the ST segment were observed more often in lead V2, in men and were caused by the syndrome of early repolarization of the left ventricle, vagotonia and positional changes.
Bibliography
1. Dabrowski A. Daily ECG monitoring / A. Dabrowski, B. Dabrowski, R. Piotrovich// - M.: Medpraktika, 2000. -208 p. 2. Makarov L.M. Holter monitoring. 3rd ed. – M.: Publishing House “MEDPRACTIKA-M”. – 2008. – 456 p. 3. Ryabykina G.V., Sobolev A.V. Holter bifunctional monitoring of ECG and blood pressure - M.: ID "MEDPRA KTIKA -M". – 2010. – 320 p. 4. Holter N. Ann New York Academy of Science. – 1957. – 65. – 913.
ECG predictors of reperfusion
Pathogenetic therapy for AMI has the goal of restoring blood flow in the affected artery. Lack of restoration of blood flow (reperfusion) is the most powerful predictor of the development of LV systolic dysfunction and the risk of death after AMI. In the absence of reperfusion, 30-day mortality can reach 15% [14]. In turn, the resolution of ST segment elevation is an indicator of improved short-term (30-day) and long-term (one-year) prognosis [5]. Assessing ST segment resolution is also useful for deciding on further management of the patient.
Failure to resolve the ST segment within the first 90-120 minutes after thrombolytic administration should be a reason to consider angioplasty. A specific marker of reperfusion that has occurred is considered to be a reduction in ST segment elevation by more than 50-70% in the lead with maximum elevation, which is associated with the most favorable further prognosis. At the same time, a number of authors propose a criterion of 50% reduction in ST segment elevation after 60 minutes of reperfusion therapy as a predictor of a good prognosis in individuals with AMI [13]. Considering that the maximum effect from subsequent angioplasty after thrombolysis is achieved no later than 6-8 hours from the onset of AMI [14], reducing the time for assessing reperfusion has good reason.
Other ECG markers of reperfusion include T wave inversion within four hours of AMI onset. T wave inversion, which occurs within the first hours of reperfusion therapy, is a highly specific sign of restoration of blood flow. T wave inversion, which develops after more than four hours, is associated with natural ECG dynamics during AMI and does not indicate restoration of blood flow. Accelerated idioventricular rhythm 60-120 beats/min, late, paired, ventricular extrasystoles are also a highly specific marker of reperfusion. These rhythms are considered not dangerous and, as a rule, do not require antiarrhythmic therapy. Polymorphic ventricular tachycardia and ventricular fibrillation can also be associated with reperfusion, but are rare and more often a consequence of persistent coronary occlusion.