Pharmacokinetics
When taken orally, it is quickly and almost completely absorbed from the gastrointestinal tract. Cmax in plasma is reached after approximately 30 minutes, in cerebrospinal fluid - after 2-8 hours. The apparent Vd is 0.6 l/kg. Does not bind to blood plasma proteins.
Distributed in all organs and tissues, penetrates the BBB and the placental barrier. Selectively accumulates in the tissues of the cerebral cortex, mainly in the frontal, parietal and occipital lobes, in the cerebellum and basal ganglia.
T1/2 from plasma is 4-5 hours, from cerebrospinal fluid - 6-8 hours. It is excreted unchanged by the kidneys. In renal failure, T1/2 increases.
Instructions for use, price, reviews analogues
Piracetam must be taken in accordance with the instructions for use, as tablets and capsules are intended for internal use. The daily dosage is calculated depending on the patient’s weight and is 30-160 mg per kilogram of weight. The drug is taken 2-4 times a day, but to prevent the occurrence of insomnia, the last dose should be no later than 17 hours before bedtime.
The dosage regimen is developed by the doctor. It may vary depending on the pathology. Thus, the drug is used in complex methods of rehabilitation therapy in the treatment of serious brain damage. For recovery from complex psychotic disorders, it is used in combination with psychotropic drugs.
The price of pirocetam may vary depending on the manufacturer. But in any case, it is accessible. Today you can buy analogues of the drug in pharmacies. They are presented as single drugs and complex drugs. When prescribing such drugs, the doctor must take into account their interaction with other medications.
All nootropic drugs are highly effective, as evidenced by numerous patient reviews. First of all, they note the cumulative effect of the drug. Many note the ability to withstand heavy loads without losing concentration. You can also often find positive reviews about the treatment of children.
Drug interactions
A case of interaction of piracetam with simultaneous use with a thyroid extract containing triiodothyronine and tetraiodothyronine is described, when the patient experienced anxiety, irritability and sleep disorders.
When used simultaneously with thyroid hormones, the development of central effects is possible - tremor, anxiety, irritability, sleep disturbances, confusion.
With the simultaneous use of central nervous system stimulants, the psychostimulating effect may be enhanced.
When used simultaneously with antipsychotics, an increase in extrapyramidal disorders is observed.
Article by S.G. Burchinsky "Dangers and risks of nootropic pharmacotherapy: myth or reality?" invites readers of our journal to a discussion that will allow us to discuss a number of extremely important aspects of modern rational pharmacotherapy as one of the foundations of evidence-based medicine. Naturally, the doctor’s knowledge and experience, his awareness of the latest therapeutic technologies play a significant role in the fight to improve the patient’s quality of life. Therefore, it would be unfair to make complaints against our colleagues regarding attachment to certain medications, a kind of “fetishization” of their clinical and pharmacological parameters, and sometimes even denial of other drugs available in our arsenal. We believe that it would be fair to be guided by the criterion formulated by WHO experts back in the 80s of the last century, according to which the focus of the doctor’s attention when choosing a pharmacotherapy tool should be the benefit/risk criterion. The editors hope that our readers will support further discussion on the use of pharmacotherapy both in psychoneurology and in other areas of clinical medicine.Editor-in-Chief of the journal “Rational Pharmacotherapy” A.P. Viktorov
The progress of modern pharmacology and clinical medicine is largely determined by the discovery of new biologically active substances. This process is developing especially intensively in the field of neuro- and psychopharmacology, which is largely due to the further actualization of nervous and mental pathology as one of the leading causes of morbidity, disability and mortality, especially in developed countries. This explains the increased attention of pharmacologists and clinicians to the development and implementation of new effective and safe drugs for use in neurology and psychiatry. The general criteria for the optimality of a drug for use in neurological practice include: 1) effectiveness and breadth of the therapeutic spectrum (possibility and feasibility of use in various forms of pathology); 2) safety; 3) width of the dose range, i.e. the gap between the minimum therapeutic and minimum toxic doses (possibility of use in the form of various dosage regimens and courses, “impact” and “maintenance” therapy, etc.); 4) minimal potential for drug-drug interaction (possibility of use both as monotherapy and as part of a combined pharmacotherapeutic effect); 5) economic accessibility. It should be noted that in this list, the WHO criterion “the safety of a drug is more important than its effectiveness” in neurological practice is actually the basis for ensuring such criteria as the width of the dose range and the minimum potential for drug-drug interactions. So, most of the criteria for the optimality of a neurotropic drug are determined by its safety characteristics. The classic components of the concept of “safety” in pharmacology, which are the end-points of many large-scale clinical trials, primarily include: 1) the absence or minimal severity of side effects; 2) absence of serious side effects. No less significant characteristics in this case are the following criteria: • the drug does not have active metabolites; • absence of cross-drug interaction with the most commonly used drugs of neuro- and somatotropic type of action within the framework of polypharmacy, which is almost inevitable in neurology. Therefore, it is quite natural for practitioners around the world to strive to use the safest groups of neurotropic drugs and their individual representatives, often even at the cost of a certain reduction in the effectiveness of treatment. At the same time, the result of attempts to optimize the pharmacotherapy of neurological diseases has been the creation of combination drugs containing two or more components with different mechanisms of action, which have different effects on the pathogenesis and clinical manifestations of specific forms of pathology, in order to minimize polypharmacy and reduce the risk of drug-drug interactions . However, at the same time, clinicians were faced with at least two undesirable phenomena: 1) the identification of new, unexpected side effects of seemingly well-known drugs that have been used in practice for decades (primarily due to the pathomorphism of the clinical picture of many diseases, increased resistance to treatment pharmacotherapy, the presence of largely unexplored interactions of drugs with various environmental factors, etc.); 2) identification in a number of cases of serious risks when using combination drugs, despite the impeccable theoretical justification for the feasibility and compatibility of their components. Thus, the problem of the safety of neuropharmacotherapy has come to the fore for both pharmacologists and clinicians and has forced them to pay serious attention to the possible risks when prescribing drugs of neuro- and somatotropic type of action. One of the most relevant groups of neuro- and psychopharmacological agents that have attracted increased attention in recent years are nootropics. The main, fundamental feature of the action of these drugs can be called the influence on the biochemical processes underlying the implementation of intellectual-mnestic functions, i.e. regulation of cognitive processes, learning, memory - the basis of higher nervous activity in humans. In addition, among the pharmacological effects of nootropics, one of the leading places is occupied by cerebroprotective and stress-protective actions, which determines the advisability of using these drugs under certain conditions in healthy individuals as pharmacoprophylactic tools. As a result, the breadth of indications for the use of nootropic drugs significantly exceeds that for all other neurotropic drugs. According to generally accepted opinion, nootropics are one of the safest groups of drugs, not only among neurotropic drugs, but also in pharmacology in general. Favorable pharmacokinetic parameters, minimal severity of drug-drug interactions, a limited number of side effects and a small number of serious side effects, over-the-counter availability for many of their representatives - all this has led to an extremely wide, but often unsystematic, unjustified and uncontrolled use of nootropic drugs. However, as it turned out, treating nootropics as drugs like vitamins and herbal syrups against “all diseases at once” (including symptoms of vegetative-vascular dystonia, headache, dizziness, drowsiness or insomnia, depression, anxiety, etc.) is fraught with serious , sometimes irreparable risks. The following provisions should become axioms for a practicing physician. 1. The prescription of nootropics should be carried out only with a clearly established diagnosis and for specific indications. 2. The need for strict adherence to course and daily dosage regimens. 3. The need to carefully consider the possible unfavorable combination of various drugs when taken simultaneously. 4. The need to take into account the patient’s age and the presence of concomitant pathology. It is advisable to consider the possible risks and dangers of nootropic pharmacotherapy using the example of individual, most frequently used drugs in this group. Piracetam still remains not only the ancestor, but also the gold standard of nootropic drugs. Its drugs make up more than half of the range of the entire European nootropic market. This popularity is primarily explained by the fact that today it is piracetam, in comparison with other drugs in this group, that has the maximum breadth of the pharmacological spectrum of nootropic activity. However, most of the pharmacological effects of piracetam are nonspecific, which may be due to both the insufficient effectiveness of this drug in a number of clinical cases and the development of side effects. Side effects during piracetam therapy, although in most cases are not serious, are nevertheless relatively common, especially when using doses above 2.4 g / day, as well as in elderly and senile people, and are associated with its stimulating effect, primarily on the catecholaminergic systems of the brain. The mentioned phenomena are manifested mainly by increased excitability, irritability, anxiety, aggressiveness, sleep disturbances, and, less commonly, dizziness, tremor, and allergic skin reactions [1, 11, 18, 20]. A measure to prevent sleep disorders can be taking the drug in the first half of the day. In addition, in some cases, when using piracetam, sexual arousal and dyspeptic symptoms (nausea, diarrhea, abdominal pain) are noted. It is important to note that in some cases, especially in the elderly, the increase in the manifestations of coronary insufficiency described for piracetam can be very dangerous, which is generally not typical for other representatives of nootropics [8, 11]. This complication should be considered as a potential serious risk of pharmacotherapy in geriatric practice. Finally, piracetam has the ability to reduce the threshold of convulsive readiness and cause activation of epileptic seizures [7]. Consequently, the prescription of piracetam requires special caution in elderly and senile people, in the presence of chronic coronary heart disease, epilepsy and states of psychomotor agitation of various nature in the anamnesis. Since prescribing piracetam in doses below 1.8-2.4 g/day often does not make clinical sense, the practitioner is faced with the difficult task of carefully taking into account the potential dangers of pharmacotherapy with this drug and assessing the benefit/risk ratio of its use. A very popular group of nootropic drugs are also GABAergic drugs, in particular aminalone. It should be noted that in general, aminalon, like other drugs in this group (Pantogam, Noofen, etc.), is quite safe. However, sometimes when using it, extremely unpleasant subjective sensations are possible - a feeling of heat, insomnia, nausea, vomiting and even an increase in body temperature, which can lead to refusal of treatment. Periodically, especially at the beginning of taking aminalon, quite pronounced lability of blood pressure may occur [8, 11]. In this case, an increase in pressure can be regarded as a manifestation of hypertension, and a decrease in pressure as systemic hypotension and, as a consequence, lead to the unreasonable prescription of antihypertensive or cardiotonic drugs. At the same time, the mentioned effect of aminalon can sometimes actually mask real surges in blood pressure that require appropriate correction. In addition, aminalone has a certain potential for drug-drug interaction, enhancing the effects of benzodiazepine anxiolytics, hypnotics and anticonvulsants, which can in some cases lead to corresponding side effects associated with excessive depression of the central nervous system (CNS). The possibility of developing peculiar side effects when prescribing nicotinoyl-γ-aminobutyric acid (picamilon) deserves special attention. During the use of this drug, reactions of hyperexcitation, irritability, anxiety, which are paradoxical for a central GABA mimetic, may be observed [11], associated with a complex system of interaction of GABA with other neurotransmitter systems (in particular, serotonin and adrenergic). In clinical practice, drugs that combine nootropic and vasotropic properties are widely used - nicergoline, vinpocetine, nimodipine. Despite the fairly high degree of safety of these drugs, it is necessary to remember the risks associated with their use. Nicergoline , being a typical a-blocker, has side effects that are characteristic of this group of drugs and are often difficult to tolerate by patients. These include erythema, facial hyperemia, tachycardia, orthostatic hypotension, and with parenteral administration - collapse. In addition, dizziness, headache, sleep disturbances, and dyspeptic disorders associated with increased gastric secretion are possible. From a clinical point of view, it seems particularly important to increase myocardial oxygen demand as a result of the use of nicergoline, which can contribute to exacerbation of angina or arrhythmia, especially with a corresponding history. Finally, nicergoline should be used with great caution when taking antihypertensive drugs and anticoagulants concomitantly [5, 7, 11]. Vinpocetine has a combined nootropic and selective vasotropic effect, in general it has the smallest range of side effects (up to 2.5% for tablets, up to 5% for injections of the original drug), which, however, in some cases can be clinically significant. Transient hypotension, headache, dizziness, dyspeptic reactions, tachycardia (with parenteral administration) may be observed, and several cases of arrhythmias (extrasystoles) have been described [4, 6, 7]. Noting the almost complete absence of drug interactions with vinpocetine, one should remember the impossibility of its simultaneous use (parenterally) with heparin. Nimodipine, as a blocker of calcium channels in the vascular wall, can cause a significant hypotensive effect, erythema, headache, as well as fluctuations in heart rate and symptoms of central nervous system overexcitation (motor activity, aggressiveness). When nimodipine is used in combination with antihypertensive drugs, nitrates, and β-blockers, a pronounced hypotensive reaction and even heart failure may develop [7, 11]. These drugs with vasotropic properties must be used with extreme caution in the following cases: • in the presence of severe (acute or chronic) cardiac pathology; • in the presence of clinically significant psychopathological symptoms; • in case of disorders of the hemocoagulation system; • in conditions of polypharmacy. Ginkgo preparations are effective and safe phytopharmacological agents for the treatment of various forms of cognitive impairment and cerebrovascular pathology, and have a minimum of side effects. At the same time, it should be remembered that the degree of purification of plant materials plays a decisive role in ensuring the safe use of these products (as well as other herbal medicines). Thus, it is known that, along with rare cases of headache and dyspepsia, some ginkgo preparations can exhibit a potentially dangerous hemorrhagic effect (especially with concomitant surgical or diagnostic interventions), associated with the presence of undesirable components-impurities of these drugs - ginkgo acids [2, 11 ]. One of the traditional areas of nootropic pharmacotherapy is the use of peptide drugs. The most popular remedy of this kind is considered to be Cerebrolysin , a complex of peptides obtained from the pig brain, the molecular weight of which does not exceed 10,000 daltons. It is practically free of side effects (extremely rarely - agitation, dizziness, dyspepsia). At the same time, using the example of Cerebrolysin, one can be convinced of the importance of technically correct parenteral administration of nootropic drugs to prevent their negative effects. With rapid intravenous administration of this drug, a pronounced hyperpyretic reaction may occur, sometimes in combination with dizziness and arrhythmia [11]. Therefore, it should be administered through slow intravenous infusions after dilution with standard infusion solutions. A similar rule should be applied to prevent side effects of the combined nootropic and vasotropic drug Instenon, which contains three active substances: hexobendine, etamivan and etophylline. If the side effects of this drug are minimal when taken orally, then when administered parenterally (intravenously, less often intramuscularly), severe headaches associated with increased intracranial pressure and often extremely difficult to tolerate, hypotensive reactions, tachycardia, and facial flushing are possible. Therefore, Instenon infusions should be carried out very slowly, under constant medical supervision. Combined nootropic drugs have gained wide popularity throughout the world in recent years, and domestic clinical practice is no exception. At the same time, upon closer examination it turns out that the range of such drugs on the domestic pharmaceutical market is not particularly diverse. A very popular combination of nootropic and vasotropic components within one drug has become the combination of piracetam with cinnarizine. Such drugs are the domestic drugs Pyracizin, Cizam, Noozam, Cinatropil, Neuronorm, as well as the foreign drug Phezam. All of them contain 0.4 g of piracetam and 0.025 g of cinnarizine in 1 tablet (capsule). In itself, such a combination seems quite appropriate. It is important, however, given the massive nature of the use of these funds, to clearly define the scope of their application and the potential risk arising in this case. The latter is associated with a very serious complication observed when taking cinnarizine - the development of drug-induced parkinsonism syndrome, which is worth dwelling on in more detail. According to modern data, cinnarizine-induced parkinsonism accounts for up to 43% of all cases of drug-induced parkinsonism [15], which suggests the greatest contribution of cinnarizine to the development of the mentioned severe form of pathology among all drugs that can cause extrapyramidal insufficiency. It is important to emphasize that this phenomenon has a clearly defined age-dependent nature. The older the patient, the higher the likelihood of developing the manifestations of parkinsonism as a result of taking zinnarizin [21]. This complication is directly related to the dose of the drug and the duration of its administration [16]. Symptoms of extrapyramidal failure of one degree or another of severity were observed in 75-100% of patients aged 60-65 years and older in terms of 1 month to 1 year after the start of cinnarizin [13, 21]. The clinical features of zinnarizin-induced parkinsonism are the predominance of the symptom of tremor (in contrast to Parkinson's disease, in which Akinia and rigidity dominate at the initial stage of the disease, as well as adverse prognostic characteristics (preservation of extrapyramidal symptoms for at least 7 years after the occurrence of the first manifestations) [15, 17]. The mechanisms of development of this complication are obviously associated with the ability of zinnarisine to block dopamine receptors in the nigrostrate system [12], as well as reduce the activity of tyrosinehydroxylasis - the key enzyme of dopamine biosynthesis [19], i.e. To aggravate the main mechanisms of brain aging that directly determine the increase in extrapyramidal pathology with age [10]. Probably, a significant deterioration in the clinical state in patients with Parkinson's disease after taking this drug is also associated with the same properties of zinnarizin [15]. In addition, in addition to the effect on the symptoms of parkinsonism, zinnarizin also has the ability to provoke the development of depression [16], which can be determined by antidopaminergic and antiserotonergic properties revealed in it [14]. Finally, the presence of antihistamines in zinnarisine can determine the development of a sedative effect and inhibitory, which limits when it is used the possibility of driving and working with devices. This effect is potentiated with the concomitant use of alcohol, sleeping pills and other neurotropic drugs [9]. All of the above can significantly affect the full implementation of the social function of patients - work, study, etc. Thus, zinnarizin, despite the positive vasotropic effects, taking into account the frequency and seriousness of the side effects caused by it, is a potentially very dangerous tool. This is especially important due to the fact that this drug is prescribed mainly to the elderly and senile age in various forms of chronic cerebrovascular insufficiency, vascular dementia, etc., requiring prolonged course therapy. Returning to the previously mentioned combined drugs, attention should be focused on the need to take into account the presence of piracetam in them in a very small dose, i.e. the use of the drug on 6-12 capsules per day to achieve the recommended optimal dose load for piracetam (2.4-4.8 g), which in itself exceeds the maximum recommended daily dose for this effective combination of zinnarisine and piracetam (6 capsules per day, That is, 2.4 g of piracetam). At the same time, the recommended dose of zinnarizine as a monopoly for cerebrovascular circulation disorders is 0.075 g/day, which corresponds to the use of 3 tablets (capsules) of these combinations. However, the daily dose of piracetam, equal to 1.2 g, in most cases is absolutely insufficient to achieve a real clinical effect. Its excess is fraught with excess of the recommended doses of zinnarizin, as a result of which the risk of developing these complications increases. Thus, it should be noted that the use of the considered combination of drugs can be justified, first of all, with relatively mild variants of the course of the vascular pathology of the brain, with the predominance in the clinical picture of vascular disorders in comparison with cognitive disorders, during the dizziness of mainly vasogenic nature, in a series cases - with increased excitability and anxiety, as well as in the disease of Menyer, Migraines and some other disorders, where it is advisable to combine the effects of piracetam, antispasmodic and sedative actions with relatively short -term intake courses. In addition, the purpose of such combined tools can be shown in some cases if patients have a reaction of pronounced excitability in response to monotherapy with piracetam, although from the point of view of clinical pharmacology, a combination with piracetam of vasoactive drugs with proven election cerebrovascular effects (Vinpocetine, nicergooli would be more logical ). In conclusion, answering the question made in the title of this article, it should be recognized that nootropic pharmacotherapy, despite the established opinion about its safety, is fraught with considerable risks (sometimes very significant) associated with: • incorrect diagnosis; • incorrect choice of a drug; • improper method and/or dose mode of use of the drug; • ignoring the patient’s anamnesis and the features of concomitant pharmacotherapy; • uncontrolled administration of the drug. So, the implementation of the strategy of rational and safe nootropic pharmacotherapy involves: 1) the doctor’s adoption of a reasonable decision on the advisability of prescribing nootropic in a particular patient; 2) the choice of the corresponding drug, based on the features of the diagnosis, anamnesis, the presence of concomitant pathology and the list of other drugs of neuro- and somatotropic type of action already prescribed; 3) the readiness (psychological and practical) of the doctor for the possible development of side effects and in this regard - to the replacement of the drug or canceling treatment, as well as to conduct a set of measures to minimize the consequences of the mentioned effects. Only with the attitude to the appointment of nootropic agents as a serious medical strategy in the framework of neuropharmacological effects, the effective and safe use of one of the most promising groups of drugs in modern medicine will become possible.
References 1. Avedisova A.S., Akhapkin R.V., Akhapkina V.I., Verigo N.I. Analysis of foreign studies of nootropic drugs (using the example of piracetam) // Ros. psychiatrist. magazine – 2001. – No. 1. – P. 46-53. 2. Astakhova A.V. Side effects of dietary supplement components. Cautions regarding their use in the pre- and postoperative periods // Drug Safety. Express information. – 2002. – P. 16-23. 3. Burchinsky S.G. Nootropics: classification, mechanisms of action, comparative characteristics of pharmacological properties. – K., 2004. – 21 p. 4. Vinpocetine // Reference. polycl. doctor – 2003. – T. 1. – No. 2. – https://www.consilium-medicum/com. 5. Elagin R.I. Adrenergic drugs. Alpha adrenergic blockers // Consilium-Provisorum. – 2003. – T. 3. – No. 7. – https://www.conilum-medicum/com. 6. Kamchatnov P.R. Vertebrobasilar insufficiency // https://www.rmj.ru. 7. Compendium 2006. – T. I-II. – K.: Morion, 2006. 8. Lesiovskaya E.E., Marchenko N.V., Pivovarova A.S. Comparative characteristics of drugs that stimulate the central nervous system. Nootropic drugs // https://www.pharmindex.ru. 9. Directory. Vidal. – M.: Astrapharmservice, 2002. 10. Brain aging / Ed. V.V. Frolkis. – L.: Nauka, 1991. – 277 p. 11. Shtrygol S.Yu., Kortunova T.V., Shtrygol D.V. Side effects of nootropic drugs // Pharmacist. – 2003. – No. 11. – https://www.provisor.com.ua. 12. Camps M., Keirtz J., Guilding B. et al. Effect of cinnarizine treatment on dopamine receptors in the brain of semescent BLe 57/ J mice // 4th Int. Symp. On Calcium Antagonist: Florence, Italy, May 1989. – Abstr – P. 263. 13. Capella D. Parkinsonism, tremor and depression induced by cinnarizine and flunarizine. Brit Med J 1988; 297: 722-723. 14. Garcia-Ruiz PJ, Mena MA, Penafiel N. et al. Cinnarizine-induced parkinsonism in primates. Clin Neuropharmacol 1992; 15: 152-154. 15. Marti-Masso JF, Poza JJ Cinnarizine-induced parkinsonism: ten years later. Mov Disord 1998; 13: 453-456. 16. Micheli F., Pardal MF, Gatto M. et al. Flunarizine- and cinnarizine-induced extrapyramidal reactions. Neurology 1987; 37: 881-884. 17. Negrotti A., Calzetti S. A long-term follow-up study of cinnarizine- and flunarizine-induced parkinsonism. Mov Disord 1997; 12: 107-110. 18. Neurochemical and Psychopharmacological Approaches to Cognitive Enhancers. – Kyoto, 1995. – 268 p. 19. Takeda M., Kono T., Kitai ST Flunarizine induces a transient loss of tyrosine hydroxylase immunoreactivity in nigrostriatal neurons. Brain Res 1992; 590: 311-315. 20. Winblad B. Piracetam: a review of pharmacological properties and clinical use. CNS Drug Rev 2005; 11: 169-182. 21. WHO information. Calcium channel blockers and Parkinson's disease. DRUGINFORM 2002; 23 (4): 27-29.
Source: rpt.health-ua.com
Pregnancy and lactation
Adequate and strictly controlled studies of the safety of piracetam during pregnancy have not been conducted. Use is possible only in cases where the expected benefit to the mother outweighs the possible risk to the fetus.
Piracetam appears to pass into breast milk. If it is necessary to use it during lactation, the issue of stopping breastfeeding should be decided.
Experimental studies on animals did not reveal any negative effects of piracetam on the fetus.
Indications for piracetam
Piracetam, the instructions for use indicate this, is in demand to combat many neurological, psychiatric and drug addiction problems. The wide scope of use is associated with the following properties:
- Positive effect on metabolic processes.
- The ability to improve blood circulation in the brain.
Indications for use are:
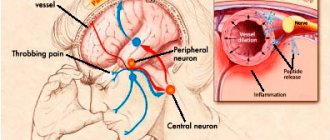
- Headaches and dizziness of various etiologies.
- The need to protect the brain from the effects of various damaging factors: intoxication, trauma, etc.
- The occurrence of cognitive impairment against the background of various diseases, which is manifested by memory deterioration.
The drug is used in the complex treatment of various mental illnesses and depressive conditions. It is also used in the treatment of chronic alcoholism, when persistent disorders of brain activity occur. When using the drug, it is possible to recover faster from brain injuries. This remedy improves the condition of patients with the development of dementia resulting from cerebral circulatory disorders. It is recommended for the prevention of Alzheimer's disease.
The drug is approved for the treatment of children in cases of confirmed dyslexia and other painful conditions, the symptoms of which are learning difficulties. The drug is indicated for perinatal brain damage. It is used for oligophrenia, cerebral palsy, and mental retardation.
Signs of memory impairment
A patient who has suffered a stroke usually faces difficulties in self-identification and other difficulties:
- Memories from childhood, adolescence or any other period of life disappear. He may not remember people he has ever encountered, certain significant situations and events.
- Loss of motor skills and loss of coordination. It’s as if the body is returning to childhood: it doesn’t remember how to eat, take care of itself in terms of hygiene, and learns everything all over again.
At the same time, there are situations when the victim remembers everything related to his profession down to the smallest detail. For example, he knows how to drive a car, knows musical notation, remembers how he wrote his dissertation, etc. - but does not have the skills of banal household self-service.
Sometimes amnesia is not immediately noticeable and appears much later in the process of secondary complications after a stroke.
When the disease occurs, the patient’s psyche also suffers: the person does not remember the people who communicate with him. Does not understand the purpose of certain items. Can’t remember professional skills – feels extremely uncomfortable. The victim may become depressed or be in a state of increased anxiety, which negatively affects the rehabilitation process and sometimes leads to psycho-emotional breakdowns.