What can cause an attack?
Infections that cause fever. The infection can be caused by bacteria, but more often febrile attacks occur with viral diseases (for example, roseola and influenza).
Vaccinations that cause fever. There is a small chance of febrile seizures after vaccination against measles, rubella and mumps, and diphtheria, tetanus and whooping cough. But the risks from incomplete vaccination are higher than the risk from a febrile attack after vaccination.
Heredity. If either parent has had a febrile seizure, the child is more likely to have seizures with fever.
A febrile attack, especially one occurring for the first time in life, is very frightening for parents. In fact, most of these attacks are not dangerous and do not lead to complications or brain damage. A child with simple febrile seizures is only slightly more likely to develop epilepsy than children who have never had a febrile seizure.
Prognosis and preventive methods
The disease is treatable, so the prognosis is positive in most cases. The situation can develop according to two scenarios - complete recovery of the patient, or transition of the pathology to epilepsy. The prognosis is made taking into account the risk of recurrence of seizures in the future, the development of epilepsy, neurological and intellectual disorders.
In most cases, attacks do not recur after the age of six. Neurological disorders are determined by the frequency and type of attacks. The prognosis worsens in the case of frequently recurring seizures of an atypical form - mental disorders are observed (developmental delay, mental retardation), the likelihood of transition to epilepsy increases to 15%.
“What to do about febrile seizures” is a question often asked by concerned parents. Our Center’s specialists advise, first of all, not to panic. When the first symptoms appear, you should immediately seek medical help!
How to help a child during an attack?
- Place your baby on his side on a flat surface and make sure he won't fall or hit anything during the cramp (such as crib bars).
- Record the time and tell the doctor when the attack began and how long it lasted.
Attention! Do not try to open the jaw, do not put anything into the child’s mouth during an attack, this can lead to injuries (broken teeth of the child and injured fingers of the person providing assistance). Do not try to restrict the child's movements during seizures, do not restrain him.
The child may be even more afraid of the attack than the parents. Try to calm him down and support him.
If the attack occurs for the first time in life, lasts longer than 5 minutes, the child is unusually sleepy and lethargic before or after the attack, call an ambulance.
In other cases, immediately show the child to the pediatrician. The doctor should examine the child after the attack to make sure there are no signs of a central nervous system infection (meningitis or encephalitis).
Togliatti Medical Consilium 2015 No. 03-04 2015
Modern look at febrile seizures
NG Lukshina
Summary
Febrile seizures are the most common type of seizure seen in the pediatric age group.
Experience shows, however, that they do not have a direct effect on cognitive function, so the prognosis for normal neurological function in children with febrile seizures is good. Children with febrile seizures have a slightly higher risk of later developing epilepsy compared with the general population risk (2% versus 1%). Risk factors for further development of epilepsy include complex febrile seizures, a family history of epilepsy or neurological disorders, and the presence of developmental delay. Febrile seizures are divided into 2 types: simple febrile seizures (which are generalized, lasting <15 minutes and do not recur within 24 hours) and complex febrile seizures (which are prolonged, repeat several times in 24 hours, or are focal). Clinicians, when assessing infants or young children following simple febrile seizures, should focus their attention on identifying the cause of the child's fever. Meningitis should be considered in the differential diagnosis for any febrile child, and therefore a diagnostic lumbar puncture should be performed if there are clinical signs or symptoms suggestive of meningitis. Any child 6 to 12 months of age who is admitted to the hospital with seizures and fever should have a lumbar puncture, especially if the child has not received the Haemophilus influenzae (Hib) or pneumococcal vaccine (i.e., has not received scheduled vaccinations such as recommended), or when immunization status is unknown, due to an increased risk of bacterial meningitis. A spinal tap is an option for children who have been treated with antibiotics. In general, simple febrile seizures usually do not require extensive testing, such as electroencephalography, blood tests, or neuroimaging. Prophylactic treatment for simple febrile seizures is not necessary. Key words:
febrile seizures, neuroimaging, electroencephalography
Summary
Febrile seizures are the most common type of seizures observed in the pediatric age group.
Evidence suggests, however, that they have little connection with cognitive function, so the prognosis for normal neurological function is excellent in children with febrile seizures. In 1980, a consensus conference held by the National Institutes of Health described a febrile seizure as, “An event in infancy or childhood usually occurring between six months and five years of age, associated with fever, but without evidence of intracranial infection or defined cause " Children with febrile seizures have a slightly higher incidence of epilepsy compared with the general population (2% vs 1%). Risk factors for epilepsy later in life include complex febrile seizure, family history of epilepsy or neurologic abnormality, and developmental delay. Febrile seizures are divided into 2 types: simple febrile seizures (which are generalized, last < 15 min and do not recur within 24 h) and complex febrile seizures (which are prolonged, recur more than once in 24 h, or are focal). Clinicians evaluating infants or young children after a simple febrile seizure should direct their attention toward identifying the cause of the child's fever. Meningitis should be considered in the differential diagnosis for any febrile child, and lumbar puncture should be performed if there are clinical signs or symptoms of concern. For any infant between 6 and 12 months of age who presents with a seizure and fever, a lumbar puncture is an option when the child is considered deficient in Haemophilus influenzae type b (Hib) or Streptococcus pneumoniae immunizations (ie, has not received scheduled immunizations as recommended), or when immunization status cannot be determined, because of an increased risk of bacterial meningitis. A lumbar puncture is an option for children who are pretreated with antibiotics. In general, a simple febrile seizure does not usually require further evaluation, specifically electroencephalography, blood studies, or neuroimaging. The prophylactic treatment of simple febrile seizures does not need. Keywords:
febrile seizures, neuroimaging, electroencephalography
Febrile seizures in children are the most common convulsive syndrome of childhood and occur only in connection with febrile fever in children aged 6 months to 5 years (approximately 2-5% of the European and American pediatric population and up to 8% in the Japanese) Studies conducted prove that they do not affect cognitive functions and have a generally good prognosis [1]. Febrile seizures (FS) are divided into three groups: - simple FS - complex FS - symptomatic FS
Epidemiology.
Approximately 70-75% of children with FS have only simple FS, another 20-25% have complex FS and 5% have symptomatic FS. Children with simple FS are at increased risk of recurrent febrile seizures; this occurs in about one third of cases. Children younger than 12 months at the time of their first episode of simple FS have a 50% chance of having them recur, and after 12 months this chance decreases to 30%. Children who have simple PS are at increased risk of subsequently developing epilepsy. The incidence of epilepsy in these children by age 25 years is approximately 2.4%, which is approximately twice the risk in the general population. The literature does not support the hypothesis that simple PS reduces intelligence (i.e., causes learning disabilities) or is associated with increased mortality [1]. Boys are significantly more likely to have PS (the exact frequency is not determined).
Etiology of simple FS:
It is based on the hereditary factor-gene PS on chromosomes 19p and 8q13-21 [2]. In different families, the modes of inheritance vary; in some families, this is the AD type of inheritance, and there may be a multifactorial variant.
Pathophysiology of febrile seizures.
FS most often occurs in young children, because their brain has a low seizure threshold at this age. In addition, at this age, children are more often susceptible to infections such as otitis media, upper respiratory tract infections, etc., to which they respond with febrile fever. Animal studies have shown an association between endogenous pyrogens, such as interleukin 1 beta, and increased neuronal excitability [5]. Also, ongoing studies show that in children the cytokine network is activated and plays a role in the pathogenesis of FS, but its exact clinical pathophysiological role is not yet clear [6, 7]. The risk of recurrence of FS
is higher in children who: - are younger than 15 months - have frequent fevers - whose parents and siblings had FS or epilepsy - had a short interval between the onset of fever and the onset of FS - had a low-grade fever before the onset of seizures - risk of FS in the child's siblings with FS about 10-20% and higher if parents also had FS [10, 18].
Clinical picture of febrile seizures.
Febrile convulsions are provoked by an increase in temperature of more than 38 ° C. Moreover, the temperature threshold that can provoke FS is unique for each child. Seizures can occur within the first 24 hours after the onset of the disease (in 25-50% of children, FS may be its first symptom) [3]. Seizures are accompanied by fever (before, during or after) without any: signs of infection NS metabolic disorders history of previous seizure disorders
Clinical picture of simple FS:
- established fever in a child in the age group 3 months-5 years - a single febrile seizure lasting no more than 15 minutes (usually 2 minutes or less) over a 24-hour period - the child does not have neurological impairment on neurological examination or according to the life and developmental history -seizures and fever are not symptoms of meningitis, encephalitis, or another condition affecting the brain -seizures are described as generalized tonic or tonic-clonic -the child does not have afebrile seizures -if there is onset of seizures in one limb or there is post-seizure weakness in one limb , then this excludes simple FS - after an attack, the child might somewhat confused or drowsy, but does not have weakness in the limbs after the seizures [8].
Clinical picture of complex FS:
— Age, neurological status, life history and fever, the same as for simple FS — Seizures are either focal or prolonged (> 15 minutes, series can be 30 minutes or >) — Or several convulsive paroxysms in a row over a 24-hour period — U the child may experience temporary weakness in the extremities in which there were convulsions
Symptomatic febrile seizures:
— Age, neurological status, life history and fever, the same as for simple FS — Child already has neurological impairment or acute illness
Diagnostics.
A thorough physical examination is necessary to assess the neurological status and psychomotor and speech development. It is necessary to exclude the presence of meningeal signs, symptoms of encephalitis, meningitis, etc. in the child.
Diagnosis of simple FS.
For simple PS there are no specific laboratory and instrumental studies [12]. First of all, it is necessary to find the cause of the feverish state. If some underlying disease is suspected, laboratory tests (eg, blood electrolytes for severe diarrhea, etc.) may be ordered. A general blood test is performed if necessary, to exclude infections and according to the child’s condition upon admission to the hospital. A general urine test is performed in patients without an obvious source of infection. In most cases, serum calcium, magnesium, phosphorus, electrolytes, and TBC levels are not indicated (Level of Evidence: B). Diagnostic lumbar puncture is mandatory for children under 12 months of age, and according to indications for children under 18 months of age. If the child received antibiotics before the onset of seizures, they may improve the symptoms of meningitis, and lumbar puncture is warranted in this situation regardless of age (Evidence Level D) [15]. If a child has meningeal signs, a lumbar puncture is mandatory (level of evidence B). In children aged 6 to 12 months who have not been fully vaccinated against Haemophilus influenzae type B and pneumococcus or their vaccination history is unknown, puncture is also indicated (level of evidence D) [16].
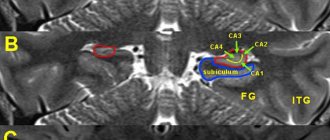
Neuroimaging in febrile seizures.
In simple PS, CT and MRI of the brain are not indicated (level of evidence B) [4, 8]. If a child has focal neurological symptoms, neurocutaneous signs, macro- and microcephaly, if neurodeficiency persists for several hours after PS, as well as with repeated complex PS, neuroimaging is performed [8]. It is also necessary if there is any doubt that these seizures are febrile in nature. Preference should be given to MRI rather than MSCT, as a more sensitive, informative and safe research method for children [17, 20].
Electroencephalography for febrile seizures.
EEG is not useful in prognostic terms in children with FS (level of evidence B). At the same time, epileptiform activity is often recorded during a continuous EEG (necessarily with recording of the sleep period). In addition, EEG has low sensitivity in children under 3 years of age (and routine EEG is practically useless). EEG also plays a limited role in the diagnosis of acute encephalopathies [18, 20].
Differential diagnosis for FS.
It is carried out with the following conditions: - Acute disseminated encephalomyelitis - Ischemic stroke - Thrombosis of the basilar artery - Idiopathic focal epilepsies of childhood - Meningococcal meningitis - Focal and generalized epilepsies - Neonatal meningitis - Viral encephalitis and meningitis
Treatment of febrile seizures.
Most simple FS goes away on its own, self-limiting, even before the patient is taken to the hospital. If the seizures are not stopped, the administration of benzodiazepines would be justified. Unfortunately, in Russia there are no the most effective and safe drugs to use: buccal midazolam, rectal diazepam, injectable lorazepam. Rectal diazepam (0.5 mg/kg) or lorazepam (0.1 mg/kg) should be administered if intravenous access cannot be established quickly [9]. Buccal midazolam (0.5 mg/kg; max dose 10 mg) was more effective than rectal diazepam in children [13]. Intravenous lorazepam is at least as effective as intravenous diazepam but is associated with fewer side effects (including respiratory depression) in the treatment of acute clonic and tonic-clonic seizures.
Preventive treatment of febrile seizures.
Continuous daily AC therapy can be carried out with phenobarbital and valproic acid drugs, but the side effects of drugs (phenobarbitalone on cognitive function, valproic acid on the liver and coagulation system) with a fairly favorable prognosis of FS are not justified [19, 20]. It is recommended to avoid continuous prophylactic administration of ACs for simple FS. In complex PS, the risks of therapy and the risks of recurrence of attacks, as well as further development of epilepsy, must be carefully weighed
Indications for hospitalization for febrile seizures.
— Undifferentiated infection — Severe infection requiring hospitalization — Repeated FS, complex FS — High degree of anxiety for parents and guardians
Consulting parents.
Febrile seizures cause great fear and anxiety in parents, so first of all, they need to be reassured and explained, most often, the benign prognosis for this condition. It is also necessary to explain to them how to behave during seizures and what help to provide to the child. It is also necessary to inform them about possible relapses of these conditions and, if the convulsions last more than 10 minutes, deliver the child by ambulance or your own transport to the nearest hospital. Febrile seizures are recognized as a benign syndrome, determined mainly by genetic factors and manifested by an age-related readiness to seizures, which eventually disappears with age. Long-term management of febrile seizures should focus on reducing parental anxiety. Long-term preventive treatment is recommended only for a small number of children with FS.
For correspondence
Lyukshina Natalya Gennadievna - Candidate of Medical Sciences, doctor of the highest category, head of the neurological department and head of the city epileptology department, member of the European Society of Child Neurologists, member of the International Association of Child Neurologists. e-mail
How to treat fever in a child who has previously had febrile seizures?
If the child does not have an increase in temperature during illness or after vaccination, it is not recommended to give antipyretic drugs! This does not reduce the risk of an attack.
If the temperature has risen, medications to reduce it make you feel better overall, but do not help with attacks.
The harm from anticonvulsants for the prevention of febrile seizures outweighs the benefits; they are almost never prescribed.
If a child’s febrile convulsions are prolonged, at the beginning of the attack it is recommended to administer a drug from the benzodiazepine group in the form of an enema, a spray in the nose or a gel on the cheek. Unfortunately, none of these forms are registered in Russia. Therefore, if an attack lasts longer than 5 minutes, an emergency doctor may give an injection of such a medicine.
For antipyretic drugs, children can be given ibuprofen at a dose of 10 mg/kg every 8 hours or paracetamol at a dose of 15 mg/kg every 6 hours. Don't give children aspirin!
Diagnosis and treatment
Treatment of febrile seizures is prescribed after:
- collection of anamnestic data (the period of manifestation of the disease, the dynamics of development, the frequency of attacks, the possibility of hereditary predisposition are taken into account);
- primary examination;
- laboratory tests (urine and blood tests);
- spinal puncture (if an inflammatory disease of the brain is suspected);
- carrying out EEG, CT, MRI.
Primary care for febrile seizures is aimed at relieving the attack and hyperthermia with the help of non-steroidal anti-inflammatory drugs and tranquilizers. Procedures for wiping the body with cool or warm water (to normalize the temperature) and ventilating the room are also carried out.
Treatment of atypical forms of pathology involves the use of antiepileptic drugs, as well as drugs with anticonvulsant effects (barbiturates, some types of diuretics, valproate).
It is important to know
Parents often mistake normal chills associated with fever for febrile seizures. With such chills, the child's arms and legs may shake rhythmically. This is similar to a seizure, but the child is conscious and reacts if spoken to. So that the doctor can better determine whether what happened was a seizure, and if so, what kind, try to clearly record the duration of the seizure, describe it as specifically as possible, and ideally, record what is happening on video (one person helps the child, the other films it on the phone).