What causes facial paralysis?
The occurrence of Bell's palsy can be facilitated by various factors that disrupt the conductivity of the nerves of the facial muscles, which leads to their immobilization and disruption of blood flow to the face.
These factors are:
- Suffered a stroke.
- Frequent infectious diseases, for example: herpes, colds, flu.
- Suffered a concussion.
- Diabetes.
- Malignant neoplasms.
- Old age, as a result, deteriorates the elasticity of facial muscles and impairs blood flow throughout the body.
- Vascular thrombosis.
- Abuse of “beauty injections”.
- HIV.
- Facial injuries or injuries caused from outside.
Healthy people and even children can be at risk for developing pathologies. Among other factors, facial paralysis can even be triggered by a stressful or emotional situation, intoxication, or such a nuisance as an unsuccessful turn of the head, as a result of which one of the nerves may be pinched.
It's scary to hear that facial paralysis can occur from simple stress. However, there is a logical explanation for this: when a person is under stress for a long time, his body weakens, the functionality of muscles and organs decreases, due to which the body becomes susceptible to various infections and diseases, one of which can be Bell's palsy .
causes of facial paralysis
Physiotherapy
Physiotherapy, including physical exercises of the facial muscles and massage, has been used for a long time in the treatment of Bell's palsy. Today there was only one randomized follow-up study, which included 50 patients with severe mimetic paralysis (a trial period of 9 months) and in which a 10-year course was administered 4 5 sessions of physical therapy with limited rights are equal to any kind of treatment. Such treatment led to a significant increase in the number of blasphemous wounds, as well as associated physical and social disability. However, the results of the study were consistent with the previous observations, since the study was inconclusive and favored a heterogeneous control group.
Prerequisites for the occurrence of neuritis
Causes of Bella's Palsy:
- Genetics. One of the reasons for the development of Bella syndrome is a narrow canal of the facial nerve, which is inherited.
- Alcoholism and drug abuse.
- Necrosis of facial tissue due to severe hypothermia.
- Oncology.
- Plastic surgery.
The following prerequisites will help determine the development of pathology:
- Noticeable weakening of the facial muscles, inability to control one or another muscle.
- Difficulty closing the eyes completely. This pathology is called lagophthalmos.
- Increased sensitivity to loud noises.
- Dulling of taste buds.
- Unreasonable tearing of the eyes or, conversely, their excessive dryness and redness.
- There is noticeable facial asymmetry.
- Paralysis of parts of the face or individual muscles.
- Swelling of the face.
- Difficulty controlling salivation.
- Jaw dropping.
Paralysis of the facial nerves, or so-called Bella syndrome, is characterized by slow progression, thanks to which it is possible to determine the development of the pathology and take the necessary treatment measures in a timely manner.
List of sources
- Alperovich P.M. Bell's palsy (etiology, pathogenesis, clinical picture, course, outcome) / P.M. Alperovich, A.G. Korneychuk, T.I.
- Konstantinovich and others //J. neuropathology and psychiatry named after. S.S. Korsakov. 1978. - T.78, No. 6. -WITH. 836-846.
- Batysheva T.T., Kostenko E.V., Boyko A.N. Complex treatment of facial nerve neuropathy using neuromidin and antioxidant therapy // Journal. psychiatrist, and psychopharmacologist. - 2008. No. 4. - P. 199-201.
- Complex treatment of patients with facial neuropathy and trigeminal neuralgia. Guidelines. - M., 2005. - 32 p.
- Maksimova M. Yu., Sharov M. N., Domashenko M. A. et al. Neuropathy of the facial nerve // Pharmateka. - 2011. - No. 14. - P. 46-51.
- Markin S.P. Neuropathy of the facial nerve // Neurology and Rheumatology. Supplement to the journal Consilium Medicum. - 2010. - No. 1. - P. 10-14.
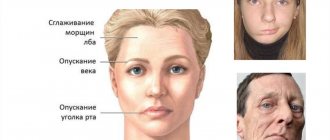
Symptoms of facial paralysis
It is worth paying attention to the occurrence of the following symptoms:
- Unpleasant and painful sensations behind the ear.
- Weakness of the facial muscles.
- Frequent migraines.
- Drooping of the corners of the mouth.
- The appearance of wrinkles in the nasolabial fold area.
- Pronounced swelling of the face.
- Unhealthy looking.
- Difficulty trying to squint.
- Dullness of hearing and smell.
As the disease progresses, the above symptoms of facial paralysis will not take long to appear.
It is especially important in the cold season to pay proper attention to protecting the face, since severe hypothermia can provoke tissue death, which can be the main cause of facial paralysis.
symptoms of facial paralysis
Pharmacotherapy
Numerical studies of LLN, including meta-analyses, have compared steroid therapy in patients treated with acyclovir or placebo. One of them, having accumulated the results of four published studies, showed a significant improvement in facial weakness with the use of glucocorticoids. Another meta-analysis, which included randomized controlled follow-up studies, showed that the initiation of hormone therapy at intervals of up to 7 days led to the development of permanent paralysis of half the face. There was a 17% increase in swelling (P = 0.005) compared with placebo. Evidence is available to show that corticosteroids reduce the incidence of permanent mimetic paralysis, although further research is needed to determine whether their use with antiviral drugs may be changing vagi.
The purpose of the rest for Bell's paralysis seems entirely logical. Acyclovir, a nucleotide analogue, blocks HSV DNA polymerase and suppresses replication. As a result of its low bioavailability (15–30%), new drugs are being tested, zocrema valacyclovir, famciclovir and sorivudine, which may have a better dosing regimen and therapeutic response in the treatment of herpetic infections ій.
The remaining systematic analysis shows that patients with NLN, treated with a combination of acyclovir and prednisolone, have a slightly better prognosis than those who found it without hormone therapy, although the results are not they looked around at Cochrane. The main determinant of the differential therapeutic response was the treatment of the ear at intervals of up to 3 days before the onset of the disease. There was also no difference in effectiveness between different routes of administration of the above-mentioned drugs. Their systemic administration should be considered in case of immunosuppression or massive herpetic infection of the central nervous system.
LITERATURE
- 1. Ahmed A. When is facial paralysis Bell palsy? Current diagnosis and treatment. Cleve Clin J Med. 2005 May;72(5):398-401, 405.
- 2. Alberton DL, Zed PJ. Bell's palsy: a review of treatment using antiviral agents. Ann Pharmacother. 2006 Oct;40(10):1838-42.
- 3. Allen D, Dunn L. Aciclovir or valaciclovir for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2004;(3):CD001869.
- 4. Gilden DH. Clinical practice. Bell's Palsy. N Engl J Med. 2004 Sep 23;351(13):1323-31.
- 5. He L, Zhou MK, Zhou D, Wu B, Li N, Kong SY, Zhang DP, Li QF, Yang J, Zhang X. Acupuncture for Bell's palsy. Cochrane Database Syst Rev. 2007 Oct 17;(4):CD002914.
- 6. Holland J. Bell's palsy. Clin Evid. 2006 Jun;(15):1745-50.
- 7. Holland NJ, Weiner GM. Recent developments in Bell's palsy. BMJ. 2004 Sep 4;329(7465):553-7.
- 8. Hughes R. Treatment of peripheral nerve disorders. Curr Opin Neurol. 2005 Oct;18(5):554-6.
- 9. Lunan R, Nagarajan L. Bell's palsy: a guideline proposal following a review of practice. J Paediatr Child Health. 2008 Apr;44(4):219-20.
- 10. Managing Bell's palsy. Drug The Bull. 2006 Jul;44(7):49-53.
- 11. Ohtake PJ, Zafron ML, Poranki LG, Fish DR. Does electrical stimulation improve motor recovery in patients with idiopathic facial (Bell) palsy? Phys Ther. 2006 Nov;86(11):1558-64.
- 12. Rahman I, Sadiq SA. Ophthalmic management of facial nerve palsy: a review. Surv Ophthalmol. 2007 Mar-Apr;52(2):121-44.
- 13. Salinas R. Bell's palsy. Clin Evid. 2003 Dec;(10):1504-7.
- 14. Salinas RA, Alvarez G, Ferreira J. Corticosteroids for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2004 Oct 18;(4):CD001942.
- 15. Shafshak TS. The treatment of facial palsy from the point of view of physical and rehabilitation medicine. Eura Medicophys. 2006 Mar;42(1):41-7.
- 16. Tiemstra JD, Khatkhate N. Bell's palsy: diagnosis and management. Am Fam Physician. 2007 Oct 1;76(7):997-1002.
- 17. Yeo SW, Lee DH, Jun BC, Chang KH, Park YS. Analysis of prognostic factors in Bell's palsy and Ramsay Hunt syndrome. Auris Nasus Larynx. 2007 Jun;34(2):159-64.
Acupuncture
A further systematic examination of the use of acupuncture for NLN has revealed the fact that this method of acupuncture speeds up the recovery and reduces long-term disability in this condition. This included three randomized controlled studies that treated 288 patients with varying degrees of mimetic paralysis in an hourly interval up to 2 days after the onset of illness. The meta-analysis was not carried out due to the shortcomings of the study design, the clinical implications between them, and the presence of prognostic variables that were not verified for this purpose.
In two studies, it was found that after 10 days of stagnation of acupuncture, the prognosis for inflammation was worse, equal to that of corticosteroids in a complex with B vitamins, dibazole and herbal herbal remedies. In the first of them, the “forcible effect” became 74%, the “moderate effect” - 23%, the “significant effect” - 3% (as opposed to 45, 31 and 23% in the pharmacotherapy group, p < 0.01), in the other The level of “fork” increased to 83%, and the “moderate effect” - 17% (on the contrary, apparently, 45 and 10% of those who took the bait, p < 0.01). The third study found that after 15 days of acupuncture in combination with medications (dexamethasone, group B vitamins and ribavirin), the overall prognosis was better, compared with pharmacotherapy. With a comprehensive assessment of such an approach to treatment in a specific group, “strong effect” fell to 52%, “pronounced effect” - 26%, “moderate effect” - 21%, and “significant effect” - 2% (on against, apparently, 12, 54, 20 and 14% in the daily drug treatment group, p < 0.01). Each of the names does not know about the side effects. The authors of this review revealed an inadequate interpretation of pre-study methods, a lack of accuracy in the calculated prognostic values, and heterogeneity of both the established methods of acupuncture and the trivialities of vicoristic acupuncture and methods for assessing the prognosis. u. According to these findings, “the results indicate the positive effects of acupuncture in patients with LP, but the limited number of available studies does not allow us to formulate clear recommendations.”
Diagnostics
Treatment of facial nerve neuritis is prescribed after an examination, which includes:
- general blood and urine tests, blood glucose levels;
- if the infectious nature of the disease is suspected (Lyme disease, HIV infection, syphilis and others) - appropriate serological tests;
- if sarcoidosis or brucellosis is suspected, chest X-ray;
- in the case of a prolonged course (more than 3 weeks), if damage to the brain stem or cerebellopontine angle is suspected, MRI is prescribed, and if the pathological process is localized in the area of the temporal bone, computed tomography is more informative;
- Electroneuromyography is used to assess the effectiveness of treatment;
- If a nerve tissue infection is suspected, a lumbar puncture and cerebrospinal fluid examination are performed.
If the patient has already been diagnosed with ear diseases, or has discharge from the ear canal or hearing loss, he should definitely consult an ENT doctor.
Facial neuritis is differentiated from Lyme disease, Ramsay Hunt syndrome, Melkersson-Rosenthal syndrome.
Treatment methods
Depending on what caused the inflammation, a course of treatment is prescribed. For bacterial lesions, the emphasis is on antibacterial therapy through systemic administration of drugs.
However, regardless of the reasons, the doctor prescribes painkillers to relieve pain and reduce inflammation. It could be:
- ibuprofen;
- paracetamol;
- analgin;
- ketorol;
- diclofenac.
All of the listed drugs can be prescribed either in the form of tablets for oral administration, or prescribed in the form of solutions for intramuscular administration.
When conservative methods are not possible, the help of a surgeon may be needed. This primarily concerns abscesses due to the eruption of wisdom teeth, pulpitis or other dental diseases. In this case, the abscess will be opened, pus will be removed, the wound will be treated with antiseptic, and the tooth will be removed, if necessary. If a pinched nerve occurs as a result of pathologies in the structure of the skull, the surgeon will perform an operation to correct the situation and free the nerve bundles.
As a complex therapy, massage, heating or exposure to a magnetic field and electric current can be prescribed. You cannot massage or warm the inflamed area yourself, because this can lead to complications associated with rupture of the purulent capsule, blood poisoning and paralysis of the facial nerve.
Separately, you may need to consult a neurologist who will determine the cause of the inflammation if other specialists have not found obvious foci of infection and abscesses.
Traditional methods of treatment are permissible only as an addition to the main therapy. For example, rinsing with chamomile decoction will relieve inflammation and reduce swelling. But you can resort to such procedures only with the permission of the attending physician.
Prevention of inflammation
To prevent the risk of developing inflammation of the trigeminal nerve, it is recommended to follow a number of measures:
- monitor oral hygiene and consult a dentist in a timely manner;
- do not stay in the cold for a long time or protect your face from freezing with a scarf;
- do not self-medicate otitis media.
At the first manifestations of pain on the face, you should immediately consult a doctor. This will stop the development of inflammation. In addition, early diagnosis allows for conservative treatment methods.
Why does nerve damage occur?
The primary manifestation of the disease is usually associated with a recent viral infection or a previous cold. The recurrent course of the disease is caused by various factors, such as:
- multiple sclerosis;
- injuries of various origins;
- cerebral aneurysm;
- tumor processes;
- parotitis;
- diabetes;
- acute otitis;
- Hunt's syndrome (damage to nerve fibers by herpesvirus);
- ischemia, or local disturbance of blood supply;
- suffered stress;
- pregnancy.
The cause of the pathological process can also be a rare neurological disorder - Melkerson-Rosenthal syndrome, which is presumably inherited.