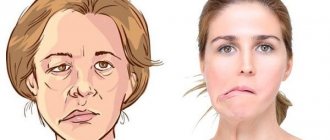
Bell's palsy is a sudden facial paralysis that usually affects the entire face or part of one side of the face. The risk of developing Bell's palsy is approximately 1 in 60. Few people develop Bell's palsy more than once in their lifetime.
Bell's palsy is a frightening condition that appears suddenly with symptoms that make many people think they are having a stroke. In fact, the signs of a stroke are completely different, and Bell's palsy is a relatively harmless condition that usually goes away without treatment.
Causes of Bell's palsy
The specific cause of Bell's palsy is unclear, but most researchers believe the most likely cause is a viral infection (herpes) that causes swelling and inflammation of the facial nerve. Although research has shown that the herpes simplex virus is present in all people with Bell's palsy, a direct link to the virus has not been proven.
Some people are more prone to Bell's palsy than others. Your risk is higher if you have any of the following conditions:
- colds or other similar diseases;
- herpes;
- any type of diabetes;
- flu;
- pregnancy.
Bell's palsy symptoms and complications
You may find that you are unable to change your facial expressions as usual. Typically, you will not be able to close one eye completely. Other possible symptoms:
- altered sense of taste;
- no tears in one eye;
- facial pain, discomfort in or behind the ear (less than 50% of cases);
- sensitivity to noise on the affected side.
There is none of the confusion, language difficulties or severe headaches that are commonly seen in stroke victims. You may have problems with speech, but these are purely muscle problems, whereas stroke victims have difficulty finding the right words.
Symptoms usually appear immediately. Sometimes they get worse within a few days. Persistent, progressive paralysis over several weeks is not a sign of Bell's palsy.
The most serious complication seen with Bell's palsy is permanent mild facial paralysis. This occurs in a minority of cases. Overall, about 80% recover completely within 3 weeks, and the majority of the rest clearly improve.
Another complication is an increased risk of stroke. Stroke prevention and follow-up are recommended.
Some people do not recover completely. It is more common in people over 60 who experience weakness or paralysis on both sides of the face.
People who do not fully recover may be left with one or more of the following symptoms:
- abnormal blinking;
- asymmetrical smile;
- corneal damage;
- drooling from a paralyzed mouth;
- dry eye;
- excessive sweating;
- frozen muscles in the nostril area;
- hyperacusis (perception of sounds as unusually loud);
- impaired taste;
- speech disorder;
- synkinesis (involuntary movement associated with voluntary movement).
Establishing diagnosis
Bell's palsy is diagnosed based on symptoms and physical signs. There are a number of conditions, including head trauma, that can cause facial paralysis, but few are as severe as Bell's palsy. Additional tests such as an MRI of the head are usually not needed.
Bell's palsy must be differentiated from Lyme disease, Guillain-Barre syndrome, sarcoidosis, parotid tumor, and stroke. Lymphoma can also in rare cases cause facial paralysis.
Paralytic strabismus
- Causes
- Diagnostics
- Treatment
Paralytic strabismus is caused by paralysis or paresis of one or more extraocular muscles, caused by various reasons: trauma, infections, neoplasms, etc. It is characterized primarily by the limitation or lack of mobility of the squinting eye in the direction of the action of the paralyzed muscle. When looking in this direction, double vision or diplopia occurs.
If with concomitant strabismus a functional scotoma relieves double vision, then with paralytic strabismus another adaptation mechanism arises: the patient turns his head in the direction of the action of the affected muscle, which compensates for its functional insufficiency. Thus, the third symptom characteristic of paralytic strabismus arises - forced rotation of the head. So, with abducens nerve palsy (impaired function of the external rectus muscle), for example the right eye, the head will be turned to the right. Forced rotation of the head and tilt towards the right or left shoulder with cyclotropia (displacement of the eye to the right or left of the vertical meridian) is called torticollis.
Ocular torticollis should be differentiated from neurogenic, orthopedic (torticollis), and labyrinthine (with otogenic pathology). Forced rotation of the head allows you to passively transfer the image of the object of fixation to the central fovea of the retina, which eliminates double vision and provides binocular vision, although not quite perfect.
As a result of deviation, as with concomitant strabismus, a disorder of binocular vision occurs. It should, however, be noted that in children, topical diagnosis of paralytic strabismus, and sometimes differential diagnosis with concomitant strabismus, is very difficult.
Causes
Paralytic strabismus may be caused by damage to the corresponding nerves or a violation of the function and morphology of the muscles themselves. Paralysis can be central or peripheral. The first arise as a result of volumetric, inflammatory, vascular or dystrophic disorders and injuries in the brain, and the second - in the presence of similar processes and consequences of injuries in the orbit and in the nerve branches themselves.
Changes in muscles and nerves can be congenital or occur as a result of infectious diseases (diphtheria), poisoning (botulism), orbital phlegmon, and often as a result of direct injury (rupture) of the muscle itself. Congenital paralysis is not a common occurrence and is usually combined. With simultaneous paralysis of all optic nerves, complete ophthalmoplegia occurs, which is characterized by eye immobility, ptosis and pupil dilation.
Complete damage to the oculomotor (III cranial) nerve causes paralysis or paresis of the superior, medial and inferior rectus muscles of the eye, the muscle that lifts the upper eyelid, and, as a rule, loss of pupillary response to light and accommodation. With complete damage, ptosis (drooping of the upper eyelid), deviation of the eye outward and slightly downward (due to the predominance of the activity of the abducens nerve and superior oblique muscle) and dilation of the pupil are also detected.
Compressive lesions of the oculomotor nerve (aneurysm, tumor, herniation) usually cause dilation of the pupil on the affected side; ischemic damage (for example, in diabetes mellitus) covers the central part of the nerve and is usually not accompanied by pupil dilation.
Damage to the abducens (VI cranial) nerve causes paralysis of the lateral rectus muscle in combination with inward abduction of the eye; when looking towards the affected muscle, non-crossed diplopia occurs (the image appearing in the abducted eye is projected laterally than the image in the adducted eye).
Lesions at the level of the pons are often accompanied by horizontal gaze paresis or internuclear ophthalmoplegia.
Damage to the trochlear (IV cranial) nerve leads to paralysis of the superior oblique muscle of the eye and is manifested by impaired downward movement of the eyeball; diplopia is most pronounced when looking down and inward and disappears when turning the head to the “healthy” side.
Diagnostics
A sign of paralytic strabismus is also the inequality of the primary angle of strabismus (squinting eye) to the secondary angle of deviation (healthy eye). If you ask the patient to fix a point (for example, look at the center of the ophthalmoscope) with a squinting eye, the healthy eye will deviate to a much larger angle.
In paralytic strabismus, it is necessary to determine the affected extraocular muscles. In preschool children, this is judged by the degree of eye mobility in different directions (determination of the visual field). At older ages, special methods are used - coordimetry and provoked diplopia .
A simplified way to determine the field of view is as follows. The patient sits opposite the doctor at a distance of 50-60 cm, the doctor fixes the patient’s head with his left hand and asks him to alternately watch with each eye (the second eye is covered at this time) the movement of an object (pencil, hand ophthalmoscope, etc.) in 8 directions. Muscle deficiency is judged by the limitation of eye mobility in one direction or another. In this case, special tables are used. Using this method, only severe limitations in eye mobility can be identified.
If there is a visible deviation of one eye vertically, a simple adduction method can be used to identify the paretic muscle. The patient is asked to look at an object, move it to the right and left and observe whether the vertical deviation increases or decreases with extreme gaze aversions. Determination of the affected muscle in this way is also carried out using special tables.
Chess coordimetry is based on dividing the visual fields of the right and left eyes using red and green filters.
To conduct the study, a coordimetric set is used, which includes a graphed screen, red and green flashlights, and red-green glasses. The study is performed in a darkened room, on one of the walls of which there is a screen divided into small squares. The side of each square is equal to three angular degrees. In the central part of the screen there are nine marks placed in the form of a square, the position of which corresponds to the isolated physiological action of the oculomotor movements of the mouse.
A patient wearing red-green glasses sits at a distance of 1 m from the screen. To examine the right eye, a red flashlight is placed in his hand (red glass in front of the right eye). The researcher holds a green flashlight in his hands, the beam of light from which he directs one by one to all nine points and asks the patient to combine the light spot from the red flashlight with the green light spot. When trying to combine both light spots, the examinee usually makes a mistake by some amount. The doctor records the position of the green spot to be fixed and the red spot to be trimmed on a diagram (sheet of graph paper), which is a small copy of the screen. During the examination, the patient's head should be motionless.
Based on the results of a coordimetric study of one eye, it is impossible to judge the state of the oculomotor system; it is necessary to compare the results of coordimetry of both eyes.
The field of view in the diagram drawn up based on the results of the study is shortened in the direction of action of the weakened muscle, while at the same time there is a compensatory increase in the field of view in the healthy eye in the direction of the action of the synergist of the affected muscle of the squinting eye.
The Haab-Lancaster method of studying the oculomotor system in conditions of provoked diplopia is based on assessing the position in space of images belonging to the fixating and deviated eye. Diplopia is caused by placing a red glass on the squinting eye, which allows you to simultaneously determine which of the double images belongs to the right and which to the left eye.
The nine-point study design is similar to that used for coordimetry, but there is one (rather than two). The study is carried out in a dimly lit room. There is a light source at a distance of 1-2 m from the patient. The patient's head should be motionless.
As with coordimetry, the distance between the red and white images in nine gaze positions is recorded. When interpreting the results, it is necessary to use the rule according to which the distance between double images increases when looking in the direction of the action of the affected muscle. If during coordimetry the field of view is recorded (decreases with paresis), then with “provoked diplopia” - the distance between double images, which decreases with paresis.
Diplopia due to paralysis of individual eye muscles
- Paralysis of the lateral rectus muscle of the right eye - the inability to move the right eye to the right. Visual fields: horizontal homonymous diplopia, increasing when looking to the right;
- Paralysis of the medial rectus muscle of the right eye - the inability to move the right eye to the left. Visual fields: horizontal crossed diplopia, increasing when looking to the left;
- Paralysis of the inferior rectus muscle of the right eye is the inability of the right eye to move downward when turning the eyeballs to the right. Visual fields: vertical diplopia (the image in the right eye is located lower), increasing when looking to the right and down;
- Paralysis of the superior rectus muscle of the right eye is the inability to move the right eye upward when turning the eyeballs to the right. Visual fields: vertical diplopia (the image in the right eye is located higher), increasing when looking to the right and up;
- Paralysis of the superior oblique muscle of the right eye - the inability of the right eye to move downward when turning the eyeballs to the left. Visual fields: vertical diplopia (the image in the right eye is located lower), increasing when looking to the left and down;
- Paralysis of the inferior oblique muscle of the right eye is the inability to move the right eye upward when turning the eyeballs to the left. Visual fields: vertical diplopia (the image in the right eye is located above), increasing when looking to the left and up.
Treatment
Treatment of paralytic strabismus consists primarily of eliminating the underlying disease that caused it (infections, tumors, injuries, etc.). If, as a result of the general measures taken, paralytic strabismus does not disappear, the question of surgical intervention may arise.
The issue of indications and timing of surgery can be resolved positively only together with the relevant specialists (neurologists, oncologists, infectious disease specialists, etc.).
Post-traumatic strabismus, as a rule, is corrected surgically after at least 6 months. from the moment of damage, since in this case regeneration of both the muscle and the nerve is possible, and, consequently, partial or complete restoration of function.
Treatment of Bell's palsy
Often no medication is prescribed at all, but each person with Bell's palsy needs special protection for themselves and their open eye. Typically the eye remains open for at least a week and may not produce tears. Eye drops, eye cups and special lotions at night are used. They almost always prevent long-term damage to the surface of the eye (cornea).
Some specialists prescribe the antiviral drug acyclovir if the patient has herpes simplex. Corticosteroids, such as prednisone, are usually prescribed to reduce swelling around the nerve. They are usually taken within 7-10 days. However, there is little evidence that they speed up or improve recovery.
In the past, a surgical technique called seventh nerve decompression was sometimes used. This is now rare, as many experts believe the problem is caused by inflammation rather than nerve compression.
There is no proven way to prevent Bell's palsy.