Pyramid system - what is it?
It is a collection of nerve cells (motoneurons) grouped into a complex of pathways that stretch from the cerebral cortex (the center of higher nervous activity) through the anterior horns of the spinal cord to the receptors located in the muscles. Thanks to this transmission of nerve impulses, movement occurs.
The peculiarity is that the transmission of these nerve impulses is voluntary, that is, controlled by consciousness.
What is the extrapyramidal system?
This is a system of neurons and pathways in the brain that makes clear, fast, highly precise movements possible. Although these paths do not intersect with the paths of the pyramidal system, they constantly interact.
The main difference between the pyramidal and extrapyramidal systems is the involuntary functioning of the extrapyramidal pathways. For example, when a desire arises to take a pen, a person voluntarily, consciously reaches for a specific pen (pyramid paths). However, in order to reach it, he does not need to aim, calculate the distance and force, all this happens automatically (extrapyramidal pathways).
Diagnosis and treatment
To diagnose extrapyramidal movement disorders, the clinical picture must meet the diagnostic criteria for the disease. For example, diagnostic criteria for Parkinson's disease:
- for the first time symptoms appear unilaterally;
- tremor at rest;
- the disease gradually progresses;
- the disease lasts more than 10 years;
- symptoms go away when taking L-DOPA.
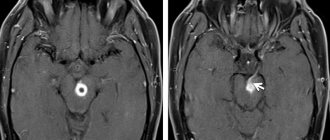
To confirm a disease with extrapyramidal disorder, data from instrumental research methods are needed: magnetic resonance imaging, computed tomography, electroencephalography, electroneuromyography.
Diseases and syndromes with extrapyramidal disorders are treated with the following approaches:
- Neuroprotective therapy. It aims to prevent or slow down the degeneration of brain cells.
- Symptomatic therapy. Aimed at eliminating specific symptoms.
- Pathogenetic therapy. Aimed at restoring chemical processes in the brain, eliminating neurophysiological imbalances.
- Therapy of motor and non-motor complications.
- Psychotherapy.
Didn't find a suitable answer? Find a doctor and ask him a question!
Structure
The extrapyramidal system consists of the gray matter of the brain, that is, a collection of nerve cell bodies. The same gray matter is present in the cerebral cortex. The main structural unit is the basal nucleus or basal ganglion. These are kernels such as:
- The striopalidal system, consisting of the lentiform and caudate nuclei. The lenticular ganglion in turn consists of the putamen and the globus pallidus.
- The striatum is a more phylogenetically ancient component of this part of the basal ganglia; it includes the caudate nucleus and putamen.
- The pallidum is a younger component, represented by the globus pallidus.
- Subthalamic nucleus.
- Red core.
- Substantia nigra located in the midbrain.
In addition to the basal ganglia, the extrapyramidal system of the brain also includes:
- thalamus;
- cerebellum;
- olive and vestibule nuclei in the medulla oblongata;
- reticular formation;
- association centers of the cerebral cortex.
In addition, there is a division of the above structures into two departments:
- Neostriatum - includes the cortex, putamen and caudate nucleus. This system is evolutionarily younger;
- Paleostriatum - consists of the globus pallidus, vestibular nuclei, subthalamic nucleus, midbrain structures (tegmentum and substantia nigra).
Striopallidar system
Perhaps the most significant part of the basal ganglia, which has the largest number of connections with the rest of the central nervous system, is the striopallidal system.
The putamen and caudate nucleus receive information via nerve fibers from the cerebral cortex, thalamus, and midbrain (substantia nigra). From the striatum, fibers are first sent to the pallidum, and then to the rest of the nervous system: the thalamus, hypothalamus, subthalamic nucleus, brainstem (consists of the midbrain, pons and medulla oblongata). Through the thalamus, the striopallidal system also interacts with the cerebellum, the main coordinator of movements and balance.
Classification
Extrapyramidal hyperkinesis is classified according to the system of the Russian neurologist L. Petelin
Taking into account the anatomical and pathophysiological features, Petelin systematized hyperkinesis taking into account the level of damage to the structures that form the brain. There are types of hyperkinesis as a result of damage to the departments:
- Brain stem. Organic tremor, rest tremor of the parkinsonian type, myoclonus (short-term, rapid, rhythmic contraction of a muscle group), stereotypy (persistent aimless repetition of the same type of movements).
- Subcortical layer. Athetosis (slow tonic-type convulsions in the area of the limbs, face, body), chorea, torsion spasm, ballism.
- Subcortical-cortical layer. Myoclonus, manifested in various forms.
Extrapyramidal and movement disorders of sporadic and hereditary origin, unspecified and identified etiology in modern clinical practice are considered as movement disorders. In this case, there are 2 main forms - hypokinesia (deficit of motor activity) and hyperkinesia (pathological excess of motor activity). Hypokinetic disorders include Parkinson's disease, hyperkinetic disorders include tremor, myoclonus, chorea, and dystonia.
Pathways
The structure of the brain, including the extrapyramidal pathways, is truly complex. And to remember it better, it’s worth imagining all the structures through which the path passes. And the best method is to sketch them.
The following pathways of the extrapyramidal system are distinguished:
- reticular-spinal;
- red nucleus spinal;
- vestibulospinal;
- roof-spinal;
- olivospinal.
The reticular-spinal tract originates in the reticular formation in the region of the brain stem. The first neuron is here. The impulse along the nerve fibers spreads down to the second neuron. Its localization is the anterior columns of the spinal cord. Then the impulse travels along the spinal nerves to the striated muscles, where this path ends.
The red nucleus spinal tract begins with the first neuron in the red nuclei located in the midbrain. The processes of this neuron move to the opposite side and then along this side continue their course to the segments of the spinal cord, where they end with an interneuron (interneuron) - in its gray matter. This pathway influences the motor nuclei of the spinal cord, from which the impulse goes further to the skeletal muscles, indirectly - through the interneuron.
The vestibular spinal tract consists of the first neuron located in the vestibular nuclei (lateral - Deiters' nucleus, inferior - Roller's nucleus). Second neurons are also located in the anterior columns of the spinal cord, to which the impulse reaches through the medulla oblongata and the anterior funiculus of the spinal cord. The axons of the second neurons then reach the skeletal muscles.
The roof-spinal tract is considered the youngest of all the tracts that make up the anatomy of the extrapyramidal system. Starting in the superior colliculi of the midbrain, where visual information arrives, it then moves to the opposite side, heading similarly to other pathways to the corresponding segments of the spinal cord.
The olivospinal tract is essential for maintaining muscle tone in the neck and maintaining balance. It begins with the formation of the olive nucleus in the medulla oblongata and reaches the sixth segment of the cervical spinal cord. From there, the processes of motor neurons conduct impulses to the muscles of the neck.
Place of transition to the spinal cord
Resting against the medulla oblongata, the axons intersect. A side beam is formed. The part that did not twist is called the anterior corticospinal tract.
The transition of axons to the other mirror side still occurs, but in the part where innervation occurs. The end of this bundle is located in the sacral region, where it becomes very thin.
Most of the fibers switch not to motor neurons in the spinal cord, but to interneurons. They form synapses in which there are large motor neurons. Their functions are different. Interneurons make contact with sensory and motor nerve cells; they are autonomous. Each segment has its own polysynaptic “relay substation”. It's a kind of motor system. The pyramidal tract and the extrapyramidal pathway for movement regulation are different from each other.
Important What is syringomyelia and how to recognize it?
An extrapyramidal system operating in a completely autonomous mode does not require as many two-way communications because it does not require voluntary control.
Main functions
As noted above, the extrapyramidal system is an important component of the central nervous system, which makes it possible to perform everyday activities. But how does it regulate our movements, making them so precise and accurate?
The main functions of the extrapyramidal system are listed below:
- the orderliness of voluntary movements, initially regulated by the pyramidal system;
- regulation of automatic motor acts of both congenital and acquired nature;
- maintaining balance;
- regulation of muscle tone;
- involuntary contraction of facial muscles;
- regulation of movements that serve as accompanying movements (for example, rapid movement of the arms when running).
Characteristic
The extrapyramidal system regulates motor activity, maintains a certain tone of skeletal muscles, and ensures the creation and maintenance of posture. The system is responsible for the formation of automatic movements that do not require conscious control, for example, maintaining balance when the center of gravity of the body shifts, avoiding a possible damaging factor - a flying stone, a tree branch moving due to the wind.
The pathways for transmission of nerve impulses within the system are formed by descending nerve branches. Extrapyramidal conductive fibers provide interaction with the distal parts of the nervous system. Extrapyramidal disorders occur due to damage to the structures that make up the system.
Extrapyramidal disorders are a disorder of motor activity that occurs in different forms, which determines the different nature of the manifestations. Movements can be excessive, obsessive, involuntary or impossible (in the case of a significant decrease in muscle tone - paresis of skeletal muscles).
The severity of manifestations varies depending on the nature and intensity of damage to the nervous system. Some patients experience short-term myoclonus (short-term, rapid contraction of a muscle group), while others experience constant tremor (shaking), hyperkinesis (involuntary pathological movements resulting from contraction of a muscle group, provoked by an erroneous brain command).
The pyramidal system provides fine motor coordination. With the help of its structures, technically complex, graceful, precise movements are carried out. The structures of the system are formed by special cells - giant pyramidal ones, also known as Betz cells. The pathways are formed by fibers descending from Betz cells to the spinal cord. In this gap there are collaterals with the pathways of the extrapyramidal system.
Important Anankasty personality disorder
On each segment of the spinal cord there are synapses (the place of contact of two neurons) responsible for the motor activity of different parts of the body, for example, the neck, upper limbs, torso, lower limbs. Irritation of the motor cortical areas leads to the occurrence of seizures in the controlled part of the body. For example, irritation of the cortical structures in the area of the upper third part of the anterior gyrus provokes muscle spasms located in the leg area.
Irritation of the middle segment of the same gyrus leads to the occurrence of muscle cramps in the arms, the lower segment - in the half of the face opposite the hemisphere in which the focus of pathological motor activity is located. We are talking about partial seizures, which are also known as Jacksonian (after the name of the neurologist of English origin D. Jackson).
Pyramidal insufficiency is a disorder of motor activity that in adults and children is manifested by paresis (muscle weakness), paralysis (inability to perform voluntary movements) and pathological reactions (reflexes) to an irritating factor, which indicates damage to a part of the pyramidal system. Damage to Betz cells in the cortex or their axons, manifested by paralysis or central paresis, is a sign of pyramidal insufficiency.
Pyramidal syndrome is manifested by increased muscle tone in the extremities (especially in the legs), which is a consequence of excess nerve impulses coming from Betz cells to the peripheral parts of the nervous system. As a result of increased muscle tone, pathological reflexes and constant trembling occur.
Subcortical syndrome is a symptom complex for which hypomimia is typical, which is manifested by weakening or absence of facial expression (facial expressions). Subcortical syndrome is also manifested by other components, including oligobradykinesia (stiffness of movements), acheirokinesis (lack of friendly arm swings when walking), increased tone of skeletal muscles like parkinsonism, which is a reflection of extrapyramidal disorders.
Hyperkinesis
The following types of hyperkinetic disorders of the physiology of the extrapyramidal system are distinguished:
- Chorea is rapid, sudden, erratic, involuntary movements of the arms, legs, and facial muscles. This is manifested by the appearance of grimaces on the face and strange gestures.
- Athetosis - movements of the fingers, can also occur in the muscles of the tongue and face. Manifested by arching, worm-like movements of the fingers, twisting of the tongue.
- Torsion dystonia - sudden turns of the body in different directions, arching of the whole body. They often have a corkscrew appearance. First of all, the neck muscles are damaged.
- Hemibalism is one-sided, sweeping movements, most often of the hands, reminiscent of the flapping of a bird's wing.
- Tics are fast, simple, stereotypical movements of small muscle groups.
- Myoclonus is short twitching of individual muscle fibers at a very fast pace. Often, movements of the limbs are not observed.
Parkinsonism
At first glance, if the extrapyramidal nervous system “manages” unconscious movements, then extrapyramidal disorders should be expressed in motor disorders. When the pyramidal tracts are damaged, paralysis occurs. If it is complete and no movements are possible, it is called plegia, and if the function is partially preserved, neurologists call it paresis. What does “unconscious paralysis” look like? At first glance, this phenomenon is simply impossible to imagine. But it turns out that there is such an extrapyramidal pathology as “shaking paralysis”, or Parkinson’s disease. Probably everyone has heard this neurological diagnosis.
Parkinsonism occurs when neurons in the substantia nigra lose the pigment melanin. As a result, their degeneration occurs and the loss of dopamine begins. The same process occurs in the striatum. Most often, EPS (extrapyramidal symptoms) appears symmetrically and for an unknown reason. This is Parkinson's disease. But sometimes extrapyramidal insufficiency occurs on one side. This happens when, for example, there is a reason: hemorrhage or thrombosis of the corresponding vessels (stroke). As a result, secondary parkinsonism develops, and on the opposite side of the body.
Unfortunately, every third case of parkinsonism is drug-induced and is associated with the abuse of antipsychotic drugs, due to the development of neuroleptic syndrome. This often occurs in drug addicts and substance abusers who use chlorpromazine, haloperidol and other drugs without knowing the consequences.
Clinic
Probably, those people who want to understand what extrapyramidal movement disorders are should show a patient with Parkinson's disease. Of course, he will not dance and jump, as with chorea, his face will not distort with violent laughter, and his fingers will not make bizarre and worm-like movements, as with athetosis. But, based on the totality of clinical signs, it is parkinsonism that students study first. Judge for yourself. Characteristic clinical and neurological signs of parkinsonism are:
- akinesia (impoverishment of all conscious movements, complete absence of gestures);
- propulsion, retropulsion, lateropulsion. The patient begins to move with great difficulty, and once he starts, he cannot finish it. His last steps are respectively directed forward, backward or sideways;
- amimia, hypomimia (mask-like face), on which moving eyes simply “live”. A patient with parkinsonism does not lose the mobility of the extraocular muscles, and the “serration” phenomenon does not occur in them. Therefore, it is easier for such a patient to communicate with his eyes, for example, by pointing to an object, instead of saying words or starting such a painful movement;
- dysarthric and monotonous speech. The speech component is added because rigidity of the tongue and vocal muscles occurs;
- tremor appears, similar to “counting coins”, mainly in the hands, thumbs and index fingers.
Perhaps one of the most striking manifestations of parkinsonism is the “falling head” test. If a patient lying on his back raises his head and sharply removes his hands, then any normal person’s head will hit the couch. Parkinson's does not have this reaction. Due to “toothed” hypertonicity, the head slowly, with barely noticeable jerks, falls onto the couch.
In addition to parkinsonism, which is a classic example of rigidity and hypertension, let's consider its alternative - extrapyramidal hypotonicity syndrome - hyperkinesia.
Parkinson's disease
The classic manifestation of hypokinetic syndrome is Parkinson's disease or parkinsonism syndrome. Their difference lies in the fact that Parkinson's disease occurs with direct damage to the structure of the extrapyramidal system, and parkinsonism syndrome is one of the manifestations of any other diseases not associated with damage to the basal ganglia.
Parkinson's disease develops when the substantia nigra of the midbrain is damaged, which begins to produce less dopamine. Its main function is to reduce the inhibitory effect of the caudate nucleus on motor activity. When this function decreases, the caudate nucleus inhibits motor skills to a greater extent, which leads to the development of hypokinesis.
Diagnostics
Determination of the presence and severity of extrapyramidal disorders occurs in the office of a neurologist during a visual examination and testing. The diagnosis is made based on medical history and the results of instrumental examination. Basic diagnostic methods:
- Neuroimaging (CT, MRI).
- Electroencephalography (study of bioelectrical activity of the brain).
- Electroneuromyography (study of the conduction of nerve impulses in muscles).
In Parkinson's disease, an ultrasound scan of the substantia nigra area is performed. Diagnosis is often based on clinical data. A blood test can determine the concentration of glucose, hormones, tyrosine hydroxylase and dopamine. In Parkinson's disease, a blood test shows a disturbance in the activity of the mitochondrial complex.
Parkinson's disease: symptoms
In addition to stiffness and decreased movement, Parkinson's disease also manifests itself:
- increased muscle tone - in neurology the term “increased tone of the hyperplastic type” is used;
- stiffness of facial expressions;
- stooped posture;
- The supplicant's pose is characteristic - the head is tilted down, the arms are bent at the elbows, the torso is tilted;
- tremors of the limbs (tremor);
- Difficulties at the beginning of the movement and at its completion (braking).
The structure of the brain is truly complex and multifaceted. This is due to the many functions it performs. What is the value of just one extrapyramidal system! In order for us to make a basic movement, we need to simultaneously use many brain structures. It is also interesting that a lot of processes happen in a fraction of a second.
Yes, medicine has come a long way in recent decades. However, neurosurgeons have no idea how many more secrets the brain hides.
ES malfunctions
When the human body is exposed to a number of negative factors or diseases, the functioning of the extrapyramidal system is disrupted. This is accompanied by increased or decreased muscle tone, curvature of posture, and reflex disorders. Such disorders were recorded with long-term use of antipsychotic drugs (they have a direct effect on areas of the brain).
Among the most well-known disorders of the extrapyramidal system are torticollis, dyskinesia, dystonia, etc. For example, with long-term use of antipsychotic drugs, a patient is diagnosed with “rabbit syndrome”. This is a condition that is accompanied by involuntary contractions of the perioral muscles. Treatment of this pathology is very complex and lengthy. A person may also experience involuntary muscle contractions in the face or neck.
It is important to note that disruption of the extrapyramidal system is associated with a person having traumatic brain injuries, brain diseases (encephalitis, mennignitis, etc.), problems with blood vessels in the brain, genetic diseases, trauma to the child during childbirth, the presence of tumors in the brain and others. Parkinson's disease is the result of a violation of the ES. The patient experiences severe tremors of the limbs, speech becomes monotonous, and facial expressions are disrupted.
In the case of damage to the substantia nigra of the ES, the patient's reflex functions significantly increase from the time of taking the initial certain posture. When palladium is affected, the patient is diagnosed with muscle hypertension, which is also called waxy hypertension. In this case, when performing movements, the person’s posture remains unchanged. Such patients are characterized by stiffness in movements, facial expressions are completely absent (the expression resembles a mask). To make a particular movement (for example, straighten an arm) requires a lot of effort.
Treatment of problems associated with ES disorders is long and complex. Elderly people are susceptible to such pathologies; they are prescribed supportive drug therapy.