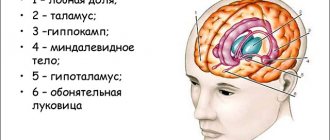
The brain is a vitally important symmetrical organ that controls all functions of the body and is responsible for human behavior. Its weight in infants is no more than 300 g, and with age it can reach 1.3-2 kg. A highly organized organ consists of billions of nerve cells interconnected by neural connections. The network of nerve fibers has an intricate structure and represents one of the most complex formations in the human body.
Anatomy of the human brain
The brain is divided into two cerebral hemispheres, the surface of which is covered with many convolutions. The cerebellum is located posteriorly. Below is the trunk, which passes into the spinal cord. The trunk and spinal cord, using the nervous system, send commands to the muscles and glands. And in the opposite direction they receive signals from external and internal receptors.
The cranium covers the top of the brain, protecting it from external influences. Blood flowing through the carotid arteries supplies the brain with oxygen. If for some reason the functioning of the main organ is disrupted, this leads to the person entering a vegetative (vegetative) state.
Brain structure
The pia mater of the brain consists of loose connective tissue with bundles of collagen fibers forming a complex dense network. It is closely fused with the surface of the brain and penetrates into all cracks and grooves, including large arterial veins that deliver oxygen to the organ.
The arachnoid mater contains cerebrospinal fluid, which performs a shock-absorbing function and is responsible for regulating the extracellular environment between nerve cells. A transparent thin arachnoid layer fills the space between the soft and hard shell.
The dura mater of the brain is a strong, thick plate, consisting of paired sheets and having a fairly dense structure. It is adjacent to the brain with its smooth inner surface, and its upper part fuses with the skull. In the places where the plate is attached to the bones, sinuses are formed - venous sinuses without valves. The dura mater plays an important role in protecting the brain matter from injury.
What are the basal ganglia?
The basal or subcortical ganglia in the brain are small collections of gray matter. The gray mass consists of nerve ganglia (axons, dendrites and auxiliary nervous tissue), which, when connected to each other, form a kind of chain.
The basal ganglia lie in deep brain structures and act as a link for transmitting information between the right and left hemispheres. This connection allows the brain to function as a single mechanism.
Long processes extending from the nerve ganglia (axons) ensure the reception and transmission of impulses to other parts of the central nervous system. The basal ganglia, or “subcortex,” interact closely with the motor control systems (corticospinal and cerebellar).
Inclusions of the gray substance are located in the thickness of the white matter. At the stage of embryogenesis, the basal ganglia are formed from a temporary structure - the ganglion tubercle. It acts as a source of neurons for the formation of mature structures of the central nervous system.
The nuclei are located near the base of the brain, slightly to the side of the optic thalamus. The basal ganglia are anatomically a structural unit of the forebrain.
The functionality of the “subcortex” is combined into two systems:
- Striopallidal - acts as the main transmitter of information between the trunk of the central nervous system and the cortex.
- Limbic - provides communication between structures that are located between the thalamic region.
These systems include different structural units of the “subcortex”.
Divisions of the brain
The large hemispheres are divided into four zones. The picture below shows the location of the lobes of the cerebral cortex:
- The frontal part is indicated in blue.
- Violet – parietal region.
- Red – occipital zone.
- Yellow – temporal lobe.
Table of brain regions
| Department | Where is it located? | Basic structures | What is he responsible for? |
| Front (end) | Frontal lobes of the head | Corpus callosum, gray and white matter; basal ganglia – striatum (caudate nucleus, globus pallidus, putamen), xiphoid body, fence | Behavior control, action planning, movement coordination, skill development |
| Intermediate | Above the midbrain, below the corpus callosum | Thalamus, metolamus, hypothalamus, pituitary gland, epithalamus | Hunger, thirst, pain, pleasure, thermoregulation, sleep, wakefulness |
| Average | Upper part of the brain stem | Quadrigeminal, cerebral peduncles | Regulation of muscle tone, ability to walk and stand |
| Oblong | Continuation of the spinal cord | Cranial nerve nuclei | Metabolism; protective reflexes: sneezing, lacrimation, vomiting, coughing; ventilation, breathing, digestion |
| Rear | Adjacent to the oblongata section | Pons, cerebellum | Vestibular system, perception of heat and cold, coordination of movement |
The table of brain sections presents the main functions of the higher organ. The slightest malfunction of the nervous system leads to serious complications and adversely affects the entire human body. Let's consider the most common pathologies associated with impaired brain activity.
Symptoms of basal ganglia dysfunction
When the basal ganglia are damaged or dysfunctional, symptoms associated with impaired coordination and precision of movements occur. Such phenomena are called the collective concept of “ dyskinesia
,” which, in turn, is divided into two subtypes of pathologies: hyperkinetic and hypokinetic disorders. Symptoms of basal ganglia dysfunction include:
- akinesia;
- impoverishment of movements;
- voluntary movements;
- slow movements;
- increase and decrease in muscle tone;
- muscle tremor in a state of relative rest;
- desynchronization of movements, lack of coordination between them;
- poor facial expressions, scanned language;
- erratic and arrhythmic movements of small muscles of the hand or fingers, the entire limb or part of the whole body;
- pathological postures unusual for the patient.
Most manifestations of the pathological functioning of the basal ganglia are based on disturbances in the normal functioning of the neurotransmitter systems of the brain, in particular the dopaminergic modulating system of the brain. In addition, however, the causes of symptoms are previous infections, mechanical brain injuries or congenital pathologies.
- Consequences of physiological disorders
- Features of the structure of the basal ganglia
- Functions of the basal ganglia
- Syndromes involving the extrapyramidal system
- Pathological states of nuclei
- Functions of the basal ganglia
- Functions associated with this subcortical structure
- Anatomy and physiology of the basal ganglia
- ITEMS
Damage to the basal ganglia
The basal ganglia (ganglia) are separate accumulations of gray matter in the subcortical part of the cerebral hemispheres. One of the main formations is the caudate nucleus (nucleus caudatus). It is separated from the thalamus by a white stripe - the internal capsule. The ganglion consists of the head of the caudate nucleus, body and tail.
The main disorders due to improper functioning of the nuclei:
- violation of movement coordination;
- involuntary trembling of the limbs;
- inability to learn new skills;
- inability to control behavior.
Let us consider the clinical manifestations of damage to the caudate nucleus.
Caudate nucleus
Purposeful action
A review of neuroimaging studies, anatomical studies of caudate connectivity, and behavioral studies reveals a role for the caudate in executive functioning. A study of patients with Parkinson's disease (see below) may also contribute to increasing evidence.
Bilateral neuroimaging approaches (including PET and fMRI) and anatomical studies reveal a strong connection between the caudate and cortical layers associated with executive functioning: "non-invasive measures of anatomical and functional connectivity in humans demonstrate a clear connection between the caudate process." and executive frontal areas." [14]
Meanwhile, behavioral research provides another layer of argument: Recent research suggests that the caudate is fundamental to goal-directed action, that is, “choice of behavior based on changing goal values and knowledge of what actions lead to what results.” . "[14] One such study involved rats with levers that triggered the release of a cinnamon-flavored solution. After the rats learned to press the lever, the researchers varied the outcome value (the rats were taught to dislike the scent, either because they were given too much of the scent or because the rats felt sick after drinking the solution) and effects. were observed. Normal rats were less likely to press the lever, while rats with caudate lesions did not suppress the behavior as effectively. In summary, the study demonstrates a link between caudate and goal-directed behavior; rats with damaged caudate nuclei had difficulty assessing the changing value of the outcome. [14] In a 2003 study of human behavior, a similar process was repeated, but this time the decision was whether to trust another person when money was at stake. [15] Although the choice here was much more complex—subjects were not simply asked to press a lever, but many different factors had to be weighed—the study was still based on behavioral selection based on changing the values of the results.
In short, neuroimaging and anatomical studies support the claim that the caudate plays a role in executive functioning, while behavioral studies are increasing our understanding of how the caudate guides some of our decision-making processes.
Memory
A subcortical loop of the dorsal prefrontal cortex involving the caudate nucleus has been associated with working memory deficits, particularly in patients with schizophrenia. Functional imaging has shown activation of this subcortical loop during working memory tasks in primates and healthy humans. The caudate may also be associated with working memory deficits even before the onset of the disease. Caudate nucleus volume was found to be inversely associated with perseverative errors in spatial working memory tasks. [16] [17]
The tonsils send direct projections to the caudate nucleus. Both the amygdala and the caudate nucleus have direct and indirect projections to the hippocampus. The influence of the amygdala on memory processing in the caudate nucleus was demonstrated by the finding that lesions involving connections between these two structures "blocked the memory-enhancing effects of oxotremorine injected into the caudate nucleus." In a study involving rats undergoing water maze training, the caudate nucleus was found to improve memory of visual cue training after amphetamine was injected into the caudate post-training. [18]
Education
In a 2005 study, subjects were asked to learn to categorize visual stimuli by classifying images and receiving feedback on their responses. Activity associated with successful classification learning (correct categorization) was centered on the body and tail of the caudate, while activity associated with feedback processing (resulting in incorrect categorization) was centered on the head of the caudate. [19]
Sleep
Bilateral lesions in the head of the caudate nucleus in cats were correlated with decreased duration of deep slow-wave sleep during the sleep-wake cycle. As the overall volume of deep slow-wave sleep decreases, the transition from short-term memory to long-term memory can also be negatively affected. [20] However, the effect of caudate nucleus ablation on cats' waking patterns was not consistent. Normalization was found three months after ablation of the caudate nucleus. This finding could be due to the interconnected nature of the roles of the caudate nucleus and frontal cortex in controlling activation levels of the central nervous system. Cats with the caudate end removed, although constantly hyperactive, had a significant reduction in rapid eye movement sleep (REMS) time that lasted only about two months. However, frontal cats showed a consistent decrease in REMS time and only a transient period of hyperactivity. [21]
In contrast to the associations between deep sleep, REM sleep, and the caudate nucleus, a study involving EEG and fMRI measurements during human sleep cycles found that the caudate nucleus exhibits reduced activity during slow-wave sleep across all stages of sleep. [22] Additionally, studies of human caudate nucleus volume in patients with congenital central hypoventilation syndrome (CCHS) have established a correlation between CCHS and significant reductions in left and right caudate nucleus volume. CCHS is a genetic disorder that affects the sleep cycle by reducing the desire to breathe. Thus, the caudate nucleus is hypothesized to play a role in human sleep cycles. [23]
Emotions
The caudate nucleus is involved in the response to visual beauty and is considered one of the "neural correlates of romantic love." [24] [25]
Approach-attachment behavior and affect are also controlled by the caudate nucleus. Cats with bilateral caudate ablation persistently approached and followed objects in an attempt to contact the target while displaying a friendly demeanor, causing forelimb stomping and purring. The magnitude of behavioral responses correlated with the degree of nuclear removal. Reports of human patients with selective damage to the caudate nucleus show unilateral damage to the caudate nucleus leading to loss of instinct, obsessive-compulsive disorder, perseverative stimulus-related behavior, and hyperactivity. Most of these deficits can be classified as related to approach and attachment behaviors, from approaching goals to romantic love. [12]
Language
Neuroimaging studies show that people who can communicate in multiple languages activate the same areas of the brain regardless of language. A 2006 publication explores this phenomenon and identifies the caudate as the center of language control. Perhaps the most significant case was observed in a trilingual subject with a lesion of the caudate nucleus. The patient maintained speech understanding in her three languages, but when asked to produce a language, she involuntarily switched between the three languages. In short, "these and other data obtained with bilingual patients suggest that the left caudate is required for monitoring and controlling lexical and linguistic alternatives in production tasks." [26] [27]
Local deformations in the shape of the medial surface of the caudate correlated with language learning ability in women and the number of persistence errors during working memory tasks of spatial and verbal fluency in men. Specifically, greater caudate volume was associated with better verbal fluency. [16]
A neurological study of glossolalia showed a significant decrease in left caudate activity during glossolalia compared to singing in English. [28]
Threshold control
The brain contains large collections of neurons interconnected by excitatory synapses, forming a large network of positive feedback elements. It is difficult to understand how such a system could operate without some mechanism to prevent explosion. There is some indirect evidence [29] that the caudate may serve this regulatory role by measuring overall cortical activity and monitoring threshold potential.
Hyperkinesis
The disease is caused by uncontrolled spontaneous movements of a muscle group. The disease occurs against the background of damage to the nerve cells of the basal ganglia, in particular the caudate body and the internal capsule. Provoking factors:
- cerebral palsy;
- intoxication;
- stress;
- encephalitis;
- congenital pathologies;
- head injuries;
- diseases of the endocrine system.
General symptoms:
- involuntary muscle contraction;
- tachycardia;
- frequent blinking;
- closing the eyes;
- facial muscle spasms;
- tongue sticking out;
- pain in the lower abdomen.
Complications of hyperkinesis lead to limited joint mobility. The disease is incurable, but with the help of medications and physical therapy, symptoms can be reduced and the person’s condition can be alleviated.
Pathological states of nuclei
The most common pathologies of the basal ganglia are:
Cortical palsy
.
This pathology is formed as a result of damage to the globus pallidus and the striopallidal system as a whole. Paralysis is accompanied by tonic spasms of the legs or arms, torso, and head. A patient with cortical paralysis makes chaotic slow movements with a small scope, stretches out his lips and moves his head. A grimace appears on his face, he twists his mouth. Parkinson's disease
.
This pathology is manifested by muscle rigidity, impoverishment of motor activity, tremor and instability of body position. Modern medicine, unfortunately, has no alternatives other than symptomatic therapy. Drugs only relieve the symptoms of the disease without eliminating its cause. Getington's disease
is a genetically determined pathology of the basal ganglia.
In addition to the physical manifestations of the disease (chaotic movements, involuntary muscle contractions, lack of coordination, spasmodic eye movements), patients also suffer from mental disorders. As the pathology progresses, patients undergo qualitative personality changes, their mental abilities are weakened, and the ability to think abstractly is lost. At the end of the pathology, as a rule, doctors are presented with a depressed, panicky, selfish and aggressive patient with weakened cognitive abilities.
Hypokinesia
Damage to the caudate nucleus of the brain is a common cause of the development of a disease associated with a decrease in human motor function.
Symptoms and consequences:
- hypotension;
- intestinal malabsorption;
- deterioration in the functioning of the senses;
- decreased lung ventilation;
- atrophy of the heart muscle;
- stagnation of blood in the capillaries;
- bradycardia;
- degenerative changes in posture.
A drop in blood pressure leads to a decrease not only in physical activity, but also in mental activity. Against the background of hypokinesia, working capacity is lost, and the person completely drops out of society.
Parkinson's disease
The disease causes degenerative changes in neurons, which leads to loss of control over movements. Cells stop producing dopamine, which is responsible for transmitting impulses between the caudate nucleus and the substantia nigra. The disease is considered incurable and chronic.
Initial symptoms:
- change in handwriting;
- slowness of movements;
- tremor of the limbs;
- depression;
- muscle tension;
- slurred speech;
- disturbance of gait, posture;
- frozen facial expression;
- forgetfulness.
If one of the symptoms appears, you should consult a neurologist.
Consequences of physiological disorders
Deviations in the structure or functioning of the brain nuclei immediately lead to the following symptoms:
- movements become slow and awkward;
- their coordination is disrupted;
- the appearance of voluntary muscle contractions and relaxations;
- tremor;
- involuntary pronunciation of words;
- repetition of monotonous simple movements.
In fact, these symptoms make it clear about the purpose of the nuclei, which is clearly not enough to learn about their true functions. Memory problems are also observed periodically. If you have these symptoms, you should consult a doctor. He will prescribe a set of studies and procedures to conduct a more accurate diagnosis in the form of:
- ultrasound examination of the brain;
- computed tomography;
- taking tests;
- passing special tests.
All these measures will help determine the extent of the lesion, if any, and also prescribe a course of treatment with special drugs. In some situations, treatment can be lifelong.
Such violations include:
- deficiency of ganglia (functional). It appears in children due to genetic incompatibility of their parents (the so-called mixing of blood of different races and peoples) and is often inherited. In the last decade, there have been more and more people with such disabilities. It also occurs in adults and progresses to Parkinson’s or Huntington’s disease, as well as subcortical paralysis;
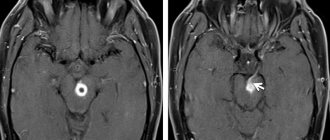
- a basal ganglia cyst is the result of improper metabolism, nutrition, atrophy of brain tissue and inflammatory processes in it. The most severe symptom is cerebral hemorrhage, followed shortly by death. The tumor is clearly visible on MRI, has no tendency to increase, and does not cause inconvenience to the patient.
Huntington's chorea
Chorea is a pathology of the nervous system that is inherited. The disease manifests itself as mental disorders, hyperkinesis and dementia. Impaired motor function is caused by jerky movements that are beyond human control. The disease causes damage to the basal ganglia, including the caudate nucleus. Although scientists have sufficient information about the anatomy of the human brain, chorea is still poorly understood.
Symptoms:
- restlessness;
- sudden movements of the arms;
- decreased muscle tone;
- convulsions;
- memory impairment;
- smacking, sighing;
- involuntary facial expressions;
- hot temper;
- dancing gait.
Complications with chorea:
- inability to self-care;
- pneumonia;
- psychoses;
- heart failure;
- delusional ideas;
- suicidal tendencies;
- panic attacks;
- dementia.
Huntington's chorea is incurable; drug therapy is aimed at alleviating the condition and prolonging the patient's working life. To prevent complications, drugs from the neuroleptic group are used. The earlier the diagnosis is made, the less the disease will manifest itself. Therefore, at the first signs of pathology, you need to consult a specialist.
Functions associated with this subcortical structure
The lenticular nucleus, like the set of structures that make up the basal ganglia, is a structure or set of structures that is essential to the proper functioning of humans. In particular, it was noted that this is of great importance in the following areas.
Motor skills
One of the aspects that has been most researched and known for a long time is the great importance of the lenticular nucleus in motor skills and movement control and coordination. In this sense, its main task is to adapt movement to existing situations and adapt to situational demands.
Maintaining Posture
The lenticular nucleus is not only involved in the implementation of specific movements, but is also related to maintaining posture. Damage to the lenticular nucleus can cause difficulty walking and uncoordinated or uncontrolled walking.
education
The lenticular nucleus influences learning processes. Specifically, it helps generate procedural learning. Additionally, through its various connections, the lenticular nucleus contributes to the creation of categories in organizing and structuring the world.
motivation
Like other areas such as the caudate nucleus, the lenticular nucleus also contributes greatly to linking the rational with the emotional, allowing the integration of both types of information. This means that through their connections we can associate knowledge or stimulus with an emotion that can motivate or demotivate us.
Related article: “Are we rational or emotional beings?”
Tourette's syndrome
Tourette's disease is a psychogenic disorder of the nervous system. The disease is characterized by motor and vocal tics that are uncontrollable.
Causes:
- damage to the brain structure due to oxygen deficiency or during childbirth;
- maternal alcoholism during pregnancy;
- severe toxicosis in the first trimester of pregnancy, which negatively affects the unborn child.
Symptoms
Simple tics are short twitches of one muscle group. These include:
- twisting of the mouth;
- frequent blinking;
- involuntary eye movements;
- sniffling;
- twitching of the head.
Complex tics include a variety of actions performed by several muscle groups:
- pronounced gestures;
- hyperkinesis;
- eccentric gait;
- jumping;
- copying people's movements;
- body rotation;
- sniffing surrounding objects.
Vocal tics:
- coughing;
- shouts;
- barking;
- repetition of phrases;
- grunting.
Before an attack, the patient experiences tension and itching in the body; after the attack, this condition disappears. Drug therapy does not completely cure Tourette's syndrome, but it can reduce symptoms and reduce the frequency of tics.
Fahr's disease
The syndrome is characterized by the accumulation of calcium in the vessels of the brain, which are responsible for providing oxygen to the internal capsule and caudate nucleus. The rare disease manifests itself in adolescence and middle age.
Provoking factors:
- carbon monoxide poisoning;
- dysfunction of the thyroid glands;
- Down syndrome;
- radiation therapy;
- microcephaly;
- tuberous sclerosis;
- disturbance of calcium metabolism.
Symptoms:
- trembling of limbs;
- convulsions;
- facial asymmetry;
- episyndrome;
- slurred speech.
Fahr syndrome is not fully understood and has no specific treatment. Progression of the disease leads to mental retardation, deterioration of motor functions, disability and death.
Features of the structure of the basal ganglia
The basal ganglia are located in the frontal and partially temporal lobes of the telencephalon. These are clusters of neuron bodies that form groups of gray matter. The white matter surrounding them is represented by processes of nerve cells and forms layers that separate the individual basal ganglia and other brain structural and functional elements.
The basal nodes include:
- striatum;
- fence;
- amygdala.
In anatomical sections, the striatum appears as alternating layers of gray and white matter. It consists of caudate and lenticular nuclei. The first is located anterior to the visual thalamus. As the caudate nucleus becomes thinner, it becomes the amygdala. The lenticular nucleus is located lateral to the thalamus optic and the caudate nucleus. It is connected to them by thin bridges of neurons.
The fence is a narrow strip of neurons. It is located between the lenticular nucleus and the insular cortex. It is separated from these structures by thin layers of white matter. The amygdala is shaped like the amygdala and is located in the temporal lobes of the telencephalon. It consists of several independent elements.
Important Bone grafting
This classification is based on the structural features and location of the ganglia on an anatomical section of the brain. There is also a functional classification, according to which scientists classify only the striatum and some ganglia of the diencephalon and mesencephalon as the basal ganglia. These structures collectively provide human motor functions and individual aspects of behavior responsible for motivation.