The spread of vascular diseases of the brain in recent years has, unfortunately, an increasing trend.
Among them is the most dangerous manifestation of cerebral vascular insufficiency - cerebral stroke (Latin “insultus” - “attack”).
Stroke is the disease of the century. The frequency of its primary cases during the year ranges in economically developed countries from 1.27 to 7.4 per 1000 population. There is also some rejuvenation of the patient population. In Russia, ischemic stroke ranks second in the structure of overall mortality after coronary heart disease. Mortality rates for men and women are 184.6 and 137.3 per 100,000 population, respectively. Only 13% of patients who have suffered an ischemic stroke return to their previous work activity.
What is a stroke and how does it develop?
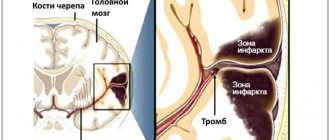
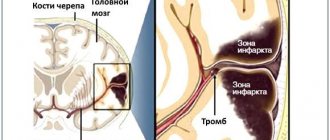
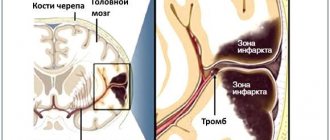
Acute cerebrovascular accident (ACVA, stroke, apoplexy) is an acute disease of the brain caused by blockage (ischemia) or rupture (bleeding - hemorrhage) of a vessel supplying part of the brain, or bleeding into the membranes of the brain.
If you tightly tighten the thigh with a tourniquet (as is sometimes necessary to do when a large vessel is injured in order to stop bleeding), necrosis of the muscles of the lower limb begins in about an hour. The brain is much more sensitive to interruptions in blood flow. Those parts of it that are suddenly deprived of the flow of oxygen and nutrients, and this is the essence of a stroke, can die within a few minutes.
There are two types of strokes: hemorrhagic type (vessel rupture and hemorrhage) and ischemic type (vessel blockage). Most often, stroke, both hemorrhagic and ischemic, develops against the background of hypertension, heart disease (atrial fibrillation, defects, paroxysmal tachycardia), heart failure, and cerebral atherosclerosis. Ischemic brain lesions predominate; the ratio of ischemic and hemorrhagic strokes is on average 5:1.
In
ischemic stroke, the cause of blockage is most often pieces that break off from atherosclerotic plaques in large vessels of the neck or thrombotic deposits on the heart valves;
blood clots that form on large plaques in areas of vasoconstriction, vascular spasms for a long time. In a hemorrhagic stroke, a vessel ruptures when there is high blood pressure, since the artery wall is unevenly thinned due to atherosclerosis. High-pressure blood pushes brain tissue apart and fills the resulting cavity, causing a blood tumor or intracerebral hematoma . Or hemorrhage occurs when a saccular formation on the wall of a vessel ruptures, which is called an aneurysm; such hemorrhage most often occurs in the lining of the brain and is called subarachnoid . Subarachnoid hemorrhage most often occurs before the age of 40 years. A disaster most often occurs after physical exertion (lifting weights, trying to break a stick over the knee), nervous stress, accompanied by a short-term rise in blood pressure.
What does rehabilitation after a stroke include?
There are many ways and methods of rehabilitation after a stroke. The rehabilitation plan depends on the patient’s general condition, motor functions, motivation, and so on.
Physical activity
- Motor skills exercises. These exercises help improve muscle strength and coordination. If necessary, therapy is prescribed to improve swallowing function.
- Mobility training. The patient is trained to use a mobility aid such as a walker, cane, wheelchair, or ankle brace.
- Therapy with restrictions. The unaffected limb is immobilized while the patient learns to move the affected limb to improve its function. This therapy is sometimes called coercive therapy.
- Development of range of motion. Certain exercises and routines can relieve muscle tension (spasticity) and help restore range of motion.
Physical activity using technology
- Functional electrical stimulation. Electricity is applied to weakened muscles, causing them to contract. Electrical stimulation helps restore paretic muscles.
- Robotics. Robotic devices help affected limbs perform repetitive movements, helping them regain strength and function.
- Video games. The use of virtual reality and other computer-based therapies involves interaction with a simulated environment in real time.
Cognitive and emotional activities may include
- Therapy for cognitive disorders. Occupational and speech therapy help restore lost cognitive abilities such as memory, information processing, problem solving, social skills, judgment and safety awareness.
- Therapy for communication disorders. Speech therapy helps restore lost abilities in speaking, listening and writing.
- Psychological assessment and treatment. Emotional adjustment and motivation are key to long-term and successful rehabilitation.
Manifestations of stroke
Subarachnoid hemorrhage manifests itself as a sudden sensation of a blow to the head (sometimes it is compared to a blow from a dagger), severe headache (at the same time the person screams in pain and even loses consciousness), there may be convulsions, but consciousness is usually restored. The patient is drowsy, lethargic, groans in pain, and holds his head with his hands. A severe headache does not allow the patient lying on his back to bend his head and touch his chin to his neck. Vomiting and nausea often occur. But, unlike hemorrhage with the formation of a cerebral hematoma, such a patient does not have paralysis.
With a hemorrhagic stroke in the cerebral hemisphere with the formation of an intracerebral hematoma, the manifestations are violent: against the background of a hypertensive crisis, a headache appears or significantly intensifies, often in one half of the head, then the patient loses consciousness, the face becomes bluish or red, breathing is hoarse, and frequent vomiting occurs. After some time, a convulsive attack may develop with a predominance of convulsions on one half of the body. If the patient regains consciousness, his limbs become paralyzed. Speech disturbances (aphasia) may also appear. Sometimes the patient does not understand the speech of others. He is like a foreigner in a state whose citizens speak a language unfamiliar to him. Often such patients forget how to read and write. Some patients develop pronounced mental abnormalities (does not know how old he is, where he is, does not recognize his loved ones, considers himself completely healthy, etc.). Sometimes vision is upset, coordination of movements and stability when standing and walking, breathing rhythm are impaired, and swallowing becomes difficult. With a hemorrhagic stroke in the brainstem, patients do not live for more than 2 days and die without regaining consciousness.
Manifestations of ischemic stroke are similar, but less clear, increasing gradually or “flickering.”
If symptoms of brain damage last less than 24 hours and then disappear completely, it is not a stroke. Such cerebrovascular accidents are called transient or (foreign term) transient ischemic attacks. Nevertheless, this is a serious signal about the possibility of developing persistent cerebrovascular accidents. But if the focal neurological symptoms are persistent, that is, they persist after a day, we can already talk about a brain catastrophe.
Recognizing an acute cerebrovascular accident is not difficult when there is severe paralysis, disorders of consciousness and speech, it is more difficult with transient disorders, but there should be one tactic - hospitalization by ambulance, if the patient is not very old and not in a coma.
When does rehabilitation begin after a stroke?
The sooner rehabilitation begins after a stroke, the higher the likelihood of regaining lost abilities and skills.
However, the immediate priorities of doctors are:
- Stabilization of condition
- Control of life-threatening conditions
- Preventing another stroke
- Preventing any complications associated with stroke
Stroke rehabilitation usually begins 24 to 48 hours after the stroke, while the patient is still in intensive care.
First aid
If your arms and legs suddenly become weak and numb, your face is distorted, speech and vision are impaired, consciousness is upset, dizziness appears, there is reason to think that a cerebrovascular accident has occurred.
There is no need to wait until the next day to invite a local doctor or family doctor; you need to urgently call an ambulance. The best option is immediate hospitalization.
But even before the ambulance arrives, it is necessary to provide proper care for the patient at home and carry out the first treatment measures.
Create a calm, comfortable position for the patient, preferably lying on his back with a small pillow under his head. The head and shoulders should lie on a pillow to prevent flexion of the neck and deterioration of blood flow through the vertebral arteries. If a person falls as a result of an attack, when lifting and laying him down, try (this is very important) to avoid sudden movements of his head. You feel that you can’t cope alone, don’t rush - it’s better to stay on the floor until help arrives.
Pay attention to the patency of the upper respiratory tract, especially in cases of impaired consciousness. Be sure to remove removable dentures from the mouth. If there is excessive salivation or accumulation of mucus in the oropharynx and nasopharynx, carefully turn the patient’s head to the side. Be sure to open a window or window - fresh air is necessary.
Monitor your blood pressure. Every person, and especially those suffering from hypertension (himself or his close relatives), should know the blood pressure numbers at which he feels comfortable. Then, when neurological symptoms appear, it is not difficult to trace on what blood pressure indicators they developed. If there are elevated blood pressure numbers, it is recommended to give antihypertensive drugs that the patient usually uses (hypertensive patients always have them in their home medicine cabinet). After giving the medicine, measure your blood pressure - it should be 5-10 mm Hg. column higher than the numbers usual for the patient.
A sharp decrease in blood pressure below the patient’s “working” numbers is strictly contraindicated; this will lead to an increase in cerebral ischemia and an increase in the size of the pathological focus.
To reduce high blood pressure before the ambulance arrives, it is recommended to give clonidine under the tongue. Sometimes a hood can help.
In the acute period of a stroke, you should avoid taking so-called peripheral vasodilators - papaverine, nicotinic acid, no-shpa, nicoshpan. They contribute to the development of the “steal” syndrome in the ischemic zone - there is a predominant dilation of unaffected vessels and an increase in cerebral blood flow in non-ischemic areas. But if nothing else is at hand, it is still better to lower blood pressure with these drugs than to leave it high.
The latest clinical and experimental studies have shown that there is a “temporary therapeutic window” within which it is possible not only to influence the functional state of the brain, but even to prevent the formation of its infarction. However, this can be achieved completely only within 6-8 minutes after the appearance of the first clinical symptoms. However, even after 3-6 hours it is possible to ensure significant reversibility of functional changes in the brain. Most drugs that protect tissue from the harmful effects of ischemia (they are called metabolic) are prescribed only by a doctor! They are taken under the control of clinical and laboratory parameters.
However, there are metabolically active drugs that must be given to the patient as quickly as possible before the ambulance arrives. This is glycine, cerebrolysin or nootropil. They are safe, do not produce unwanted side effects, and will not cause harm even when the diagnosis has not been established and the stroke is, say, hemorrhagic in nature, that is, caused by bleeding in the brain.