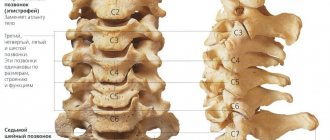
Myotonia is a rare genetic disease characterized by dysfunction of the muscular system. It occurs due to the malfunction of ion channels that transmit nerve impulses to muscle fibers. With myotonia, muscle contraction usually remains normal, but the relaxation phase is significantly prolonged, which leads to the appearance of characteristic symptoms.
The causes of the disease are purely genetic. The structure and functions of ion channels are encoded by specific genes: CNBP, DMPK and CLCN1. The occurrence of mutations in them leads to the development of myotonia.
Clinical manifestations
One of the classic symptoms of myotonia is the “fist” sign. If you ask the patient to quickly clench and unclench his fist, he will not be able to perform the last action. It will take some time to open your fingers. Likewise, the patient cannot quickly raise his eyelids, get out of bed or chair, or open his mouth. Other symptoms may include:
- stiffness,
- muscle hypertrophy,
- decreased muscle strength,
- diseases of the cardiovascular system,
- intellectual development disorder,
- impotence,
- hypersomnia.
There are several types of myotonia, which differ in a certain set of symptoms and the degree of their severity. In order to make an accurate diagnosis, the doctor is guided by the clinical manifestations of the disease, as well as information obtained during the diagnosis.
Etiology and pathogenesis of Thomsen's myotonia
The hereditary disease is caused by a mutation in the CLCN1 gene. Etiopathogenesis includes disturbances in myoneural conductivity and pathology of intracellular membranes caused by a decrease in the permeability of the plasmalemma for chlorine ions into muscle fibers. The defect provokes an ionic imbalance: chlorine ions accumulate on the surface of the microfibril without penetrating inside, which leads to bioelectrical instability in the muscle membrane.
In the muscles of patients with Thomsen's myotonia, the level of acetylcholine is increased, and in the cerebrospinal fluid and blood there is a decrease in the activity of the enzyme involved in the regulation of the excitability and contractility of muscle fibers.
Pathomorphology does not reveal changes in muscle fibers unique to this disease. The tissue defect is typical for various types of myotonia. Light microscopy reveals hypertrophy of individual muscle fibers. Histochemistry determines a decrease in type II muscle tissue. Electron microscopy reveals moderate hypertrophy of the sarcoplasmic reticulum of muscle cells, an increase in the size of mitochondria, and expansion of the telophragm of striated muscles.
Diagnostic criteria
A doctor may suspect Rossolimo-Steinert-Kurshman disease if the patient has a combination of myotonic and dystrophic changes in the muscles against the background of loss of intelligence and the presence of cardiovascular and endocrine pathology.
Polysystemicity almost always indicates the genetic nature of the disease. Such patients are subject to DNA analysis and genealogical analysis to confirm the autosomal dominant inheritance of the pathology. Electrocardiography, electroneuromyography, and hormone tests are used as informative research methods.
Due to the versatility of clinical manifestations, specialists from various branches of medicine are usually involved in the diagnosis process - genetics, cardiology, endocrinology, gynecology, andrology, neurology.
Differential diagnosis is made between dystrophic myotonia and other types of similar diseases. Unlike the others, Rossolimo's disease is characterized by muscle atrophy. Often, to confirm the diagnosis, it is necessary to resort to a biopsy to determine the level of muscle protein, which is increased in the tissues of this pathology.
Antenatal diagnosis is also carried out by examining amniotic fluid.
Symptoms of Thomsen's myotonia
Thomsen's myotonia is a genetic disease, but external clinical signs are not detected immediately after birth. In most cases, the first symptoms appear in childhood (5-8 years) and adolescence (up to 20 years).
A feature of the clinical picture is the myotonic phenomenon, characterized by:
- muscle hypotonia at rest;
- hypertonicity, spasm of muscle fibers at the moment of volitional efforts;
- prolonged muscle relaxation after the start of active movement.
Depending on the area of damage, myotonic attacks can affect the legs, arms, muscles of the neck, shoulders, and face. As a result, muscle spasms are observed when you want to spread your fingers clenched into a fist, when you start walking, when you close your jaws, close your eyes, etc.
If Thomsen's myotonia manifests at an early age, signs of muscle weakness are determined by the difficulty of the child's physical development. The baby does not sit, does not get up, does not walk in the prescribed time, his body becomes uncontrollable.
At a later age, myotonic attacks of skeletal muscles appear when walking, the desire to stand up, maintain balance, that is, with any voluntary movement. The patient, performing the first motor act, feels a sharp muscle spasm and becomes immobilized. Wanting to get up, a person suffering from this disease must lean on something. The first step when moving is given with great difficulty, sometimes the tonic spasms are so strong that the patient falls. When clenching your fingers into a fist, it is impossible to unclench them for 10 seconds or more, even if maximum effort is applied. Subsequent movements are easier and spasms stop.
During vigorous activity, the affected muscles adapt to movement and spasms disappear altogether. However, even after a short rest, muscle hypertonicity manifests itself with the same force.
In adulthood, a patient diagnosed with Thomsen's myotonia may look like an athlete if the disease affects the muscles of the limbs and trunk. Due to constant overexertion, muscle mass increases, the muscles hypertrophy and look large and pumped up.
The patient's muscles react with strong excitement even with weak external stimuli. Thus, a light blow to the affected muscles can lead to their hypertonicity. At the site of the touch, a tense muscle roll appears, which takes time to relax.
A myotonic attack is most often observed in two cases: in the initial phase of voluntary movement, requiring the participation of diseased muscles, and when they are exposed to cold. However, there are other provoking factors: prolonged stay in a static position, a sharp loud sound, an emotional outburst.
1.General information
Leiden-Thomsen disease, or myotonia congenita, is a group of inherited diseases and is rare: the prevalence in the general population is estimated at one case per 200,000 population.
Congenital myotonia is inherited in an autosomal dominant manner, that is, to develop the clinical form it is enough to receive a defective gene from one of the parents. The diagnosis entered the medical nosological paradigm from 1874-1876, when familial cases of the disease were first described.
Among the patients, males predominate.
A must read! Help with treatment and hospitalization!
Diagnosis of Thomsen's myotonia
The clinical picture gives every reason to determine the diagnosis by external signs. An important role is played by a careful collection of family history and features of clinical manifestations.
At the initial appointment, the specialist uses a neurological hammer. By lightly tapping the problem muscle area, the neurologist determines the ability of the muscles to contract and records the time of relaxation after the impact. The formation of a cushion at the site of contact reveals a myotonic symptom.
To confirm myotonia, the patient is asked to clench his fingers into a fist several times and unclench them. If the first movements are difficult, and then motor skills return to normal, then we can talk about the presence of tonic spasms. Some patients experience a myotonic pupil response when the eyes converge.
The totality of neurological symptoms reveals a decrease in the tone of muscle tissue at rest and myotonic signs of tendon reflexes.
The tonic symptom complex is observed not only with Thomsen's myotonia, but also with Eulenburg's paramyotonia, Becker's myotonia, Steiner's myotonia, as well as with other neuromuscular and endocrine disorders. In this regard, differentiation of the diagnosis and designation of a specific type of myotonia presents great difficulty in diagnosis.
Differential diagnosis includes invasive and laboratory tests:
- Muscle biopsy to identify histological changes in fibers that cause muscle cell dysfunction;
- Blood chemistry. There are no specific biochemical markers for this disease. The study is carried out to determine the level of creatine phosphokinase activity in the blood serum.
- DNA test. One of the most informative tests to determine the mutation of the CLCN1 gene. The analysis is carried out to confirm the clinical diagnosis.
- Electromyography (EMG). The invasive examination is carried out using a needle electrode. The instrument is inserted into the relaxed muscle, detecting myotonic discharges and recording motor unit potentials. The muscles are stimulated by electrodes and tapping, which causes them to contract. With repeated stimulation, the strength of myotonic spasms decreases.
- Electroneurography (ENMG). The instrumental technique is carried out to diagnose the functional state of muscle tissue and their ability to contract when stimulated by an electrical impulse. E N M G involves the use of superficial (cutaneous) and intramuscular (needle) electrodes. Graphic recording of motor unit potentials is carried out using needle electrodes. The evoked myotonic discharge is recorded through cutaneous electrodes, which represent the total activity of the muscle.
Differential diagnosis
The essence of the differential diagnosis of myotonia is to determine the form of this disease. To distinguish the congenital form of myotonia from the dystrophic one, an analysis of clinical manifestations will be required. But sometimes with congenital myotonia, mild weakness of the distal muscles of the upper limbs and weak activity on EMG are detected, which is represented by a symptom of dystrophic myotonia. Continuous muscle activity may indicate neuromyotonia; this symptom is also included in the symptom complex of a rigid person. A distinctive feature of rigid person syndrome is a decrease in muscle activity during sleep and after the administration of diazepam.
Treatment of Thomsen's myotonia
You cannot count on a complete cure. The main goal of drug and physiological therapy will be to relieve symptoms and achieve stable remission. For this purpose, the patient is prescribed:
- Mexiletine is a sodium channel blocker that significantly reduces muscle hypertonicity;
- Diakarb - improves membrane permeability;
- Quinine - reduces muscle excitability, increases the refractory period;
- Diphenin is an effective anticonvulsant;
- Diuretics - maintain ionic balance, maintaining magnesium levels and reducing potassium.
Long-term use of medications has negative aspects: all medications have a wide range of side effects.
Non-drug therapy helps improve metabolic processes in muscle tissue and reduce its tonic spasms:
- exercise therapy;
- Electrophoresis;
- Acupuncture;
- Therapeutic swimming.
The main sources of Rossolimo-Steinert-Kurshman myotonia
According to the results of recent testing of the genes of patients with dystrophic disease, it was indicated that the main role in the pathology is played by a defective disorder formed in a specific genome, which is located on the nineteenth chromosome. It is responsible for the synthesis of myotonin-protein kinase. People suffering from this abnormality are diagnosed with a severe increase in the size of certain parts of a gene called DMPK. It should be borne in mind that the degree and type of the disease being described depends on the number of repetitions of this section.
Based on accepted standards, the number of required revolutions fluctuates around 5-37. In the case of an increase above 50-80, it indicates the presence of a weak manifestation of a harmful process; with an increase in indicators in the range of 100-500, the late stage of myotonia begins, and the congenital type develops with a deviation of 500-2000. Many analyzes show that the increase in the level of trinucleotide repeats progresses, often in female cells at the stage of meiosis. That is why during the transmission of the disease from a woman, the maximum severe type of the disease or its congenital form appears.
Prognosis and prevention
The prognosis for life with Thomsen's myotonia is favorable. However, it is impossible to get rid of myotonic attacks forever. But by taking a number of preventive measures, the patient is able to alleviate his condition and live a full life.
An important point is to determine the factors that provoke myotonic attacks. Most importantly, you should not overcool, you must avoid stressful situations, intense physical activity, sudden movements, prolonged stay in one position, and emotional shocks.
Symptoms of the congenital form of Rossolimo-Steinert-Kurshman myotonia
In situations where neurologists diagnose a chronic variant of the disease, the first signs of the presence of an anomaly are pathological processes that arose in the prenatal period. Often, symptoms manifest themselves in a serious decrease in the motor activity of the developing fetus, which is noticed during an ultrasound examination by a doctor in the field of gynecology and obstetrics (during the third trimester of pregnancy). After birth, the child has the following problems:
- Diffuse disorders of muscle tissue - localized at points in the facial, chewing and oculomotor muscle tissues, as well as in the muscles of the distal parts of the limbs.
- Problems with feeding.
- Malfunctions of the breathing apparatus.
- Slow progression of motor skills.
- The appearance of oligophrenia.
Increased child mortality is recorded with increasing symptoms of the disease.
Archives
Short Wiklad
Teruyuki Kurihara Internal Medicine 2005; 44:1027-1032
HISTORY OF THE PROBLEMS
If we wanted to take a short look at the tracking of myotonia, then we can start from the work of Landau 1952 rock, if we first discovered that this state is caused by blockage of neuro-muscular endings, so that it is based on a defect in m 'ulcer membrane. During this exercise, we recorded internal cellular myotonic reactions after suppressing the “wake-up” process by disrupting the t-tubule system with the help of the chloride channel blocker anthracene-9-carboxylic acid on an experimental model of diaphragm. ragmi shura. The main finding of the research was that myotonia arises from the inactivation of neuromuscular synapses and t-tubules, and its causes are traced to the membranes of myocytes. After 1971 Lipicky et al. recorded the internal cellular potentials of meat fibers and found that their membrane supports in congenital myotonia are 2.2 times higher than the norm. Remnants of 80% of the membrane conductivity are mediated by chloride channels, according to the previous authors, the movement of membrane supports in such a pathological state reduces their functions. In 1987, Lehrmann-Horn et al. They investigated congenital paramyotonia and found that it is caused by defects in the inactivation of sodium channels in meat membranes. More extensive research has shown that the pathophysiological mechanisms of myotonic disorders are not the same - congenital myotonia is based on reduced conductivity of chlorine channels, and congenital and paramyotonia - failure to produce before activation of sodium channels.
Another significant success was genetic research into this type of disease. Single point mutations in chloride channels were detected in Thomsen's disease and autosomal recessive generalization of myotonia (Becker type), and multiple point mutations were detected in potential-dependent sodium channels in paramyotonia and with familial hyperkalemia paralysis. These heterogeneous mutations and channelopathies occur during the implementation of pathophysiological mechanisms of various myotonic disorders.
Myotonic dystrophy type 1 (MD1) is the most widespread form of myotonic dystrophy in adults. It was recently discovered that this is the inheritance of an unstable nucleotide repeat of CTG in the untranslated expansion of the protein kinase gene (DMPK) of chromosome 19. Myotonic dystrophy type 2 (MD2) is caused by an unstable CCTG nucleotide repeat in the 1st intron of the zinc fixator gene (ZNF9) of chromosome 3. Many episodes remain in Germany, Italy, Finland and the USA, and the distribution of these two countries is presented in Table 1.
Table 1. Clinical, laboratory and genetic disorders in myotonic dystrophies types 1 (MD1) and 2 (MD2)
| Myotonic dystrophy type 1 | Myotonic dystrophy type 2 (proximal myotonic myopathy) | |
| Myotonia | + | + |
| Cataract | + | + |
| Myazova's weakness | Begins from the distal ends | Begins from the proximal ends |
| Meat pains | – | + |
| Cardiac arrhythmias | ++ | + |
| Increased level of meat enzymes in the blood | + | + |
| Mental disorders | + | + |
| Shrinkage type | Autosomal dominant | Autosomal dominant |
| Chromosome ї її locus obtained | 19q 13.3 | 3q 21.3 |
| Genetic abnormalities | CTG repeat | CCTG repeat |
Both MD1 and MD2 are accompanied by myotonia and cataracts, the only characteristic clinical manifestation that differentiates them, and specific muscle pain in the other condition. In both diseases, the nucleotide repeats expressed on the RNA strands become involved in their functioning by disrupting the splicing of chloride channel genes, which, in turn, triggers myotonia, and the accumulation of triplets and tetraplet repeats in the cell nucleus, the splicing of insulin receptor genes is disrupted, which leads to concomitant diabetes . Whose geneticist can better explain the clinical symptoms of these diseases, the treatment of which may also be based on their fundamental mechanisms.
CLINICAL MANIFESTATIONS OF EXTENSIVE MYOTONIC ROSES
A patient with myotonia can be noticed immediately when you just touch his hand, but after squeezing the veins, you cannot immediately straighten your fingers. If such a sick person is lightly hit with a neurological hammer on the thenar, which will form a fleshy roll and bring out the adduction of the great toe. It is necessary to find out what is missing in the new atrophy and weakness of the muscles. In Thomsen's illness or congenital paramyotonia, these symptoms are not indicated. As with myotonic dystrophy, it is accompanied by atrophy of the muscles of the hands and feet and weakness, which begins from the distal ends and, as the disease progresses, it expands to maximum plots. Such patients are clearly characterized by a thin and thin face with drooping eyelids and cuticles, and sagging lower half of the face. In case of myotonic dystrophies, atrophic changes are also observed in the sternocleidoclavicular muscles, in addition, systemic manifestations such as mucus rash, cataracts and testicular atrophy are avoided. When making a diagnosis, do not forget about them. This is also confirmed by neuromyography (EMG), which confirms the presence of surges in the action potentials resulting from the introduction of the electrode, as well as laboratory investigations, which confirm the presence of hypothyroidism, Insulin resistance and diabetes, hypogonadism and hypothyroidism. Table 2 summarizes the stages of diagnostic testing for myotonia.
Table 2. Diagnostic test for myotonia
| 1. | Clinically, myotonia is characterized by the inability to straighten the fingers after pressing (for example, when attached) and forming the meat roll during percussion |
| 2. | Manifestations of muscle atrophy and weakness: (+) MD1 (plus mucus, characteristic lesion, cataract); (–) Thomsen's disease, autosomal recessive generalized myotonia, paramyotonia, familial hyperkalemia paralysis, fluctuating myotonia (the diagnosis of paramyotonia cannot be made in the presence of myotonic symptoms against a background of cold temperature) |
| 3. | Holchasta EMG: the presence of sparks in the potentials of the action resulting from the introduction of the electrode |
| 4. | Investigations under a light slit lamp: search for cataracts |
| 5. | Genetic research |
With congenital myotonia (Thomsen's disease) and autosomal recessive generalization of myotonia (Becker type), patients are muscular, without atrophy or weakness. With the metering of paramіoton, the holori is the niche -niche pyd diyu cold, the yak rule, the assignment, and the temperaturely illevikh channel ib depolarizasi m'yaziv is explained.
RESULTS OF MYOTONIC ROSES AND CHANALOPATHIES
It is the cause of all diseases, which are accompanied by myotonia: MD1, MD2 (which was previously called proximal myotonic myopathy), native myotonia (Thomsen's disease), autosomal recessive generalized myotonia otonia (Becker type), native paramyotonia, familial hyperkalemia paralysis, chondrodystrophic myotonia (Schwartz syndrome –Jampela) and Pompe disease (glycogenosis type 2). Zagalom її can be described as a travail of awakening and shortening of the muscles, caused by mechanical stimulation. With widespread myotonic disorders, summarized in Table 3, the mechanisms of their development have already been explained, which is due to increased restlessness of the meat membrane, decreased conductivity of chloride channels and defects Inactivation of sodium channels.
Table 3. Classification of myotonic disorders depending on the formation of defective ion channels
| Chlorine channelopathy, meat atrophy (–) | Chlorine channelopathy, meat atrophy (+) | Sodium channelopathy, meat atrophy (–) |
| 1) Thomsen's disease (autosomal dominant) 2) autosomal recessive generalized myotonia (Becker type) | 1) MD1 2) MD2 | 1) congenital paramyotonia 2) familial hyperkalemia paralysis 3) fluctuating myotonia |
And although most myotonias are classified as causative channelopathies, not all of their variants are considered the same. For example, based on electrophysiological studies, Schwartz-Jampel syndrome is a disorder of the neuromuscular synapse; the pathophysiology of myotonic spasms in Pompe disease has not yet been explained.
CLASSIFICATION OF MYOTONIA
The main myotonic disorders are classified as chloride channelopathies with and without weakness and sodium channelopathies. Classical congenital myotonia is divided into Thomsen's disease (autosomal dominant) and autosomal recessive generalized myotonia (Becker type). Myotonic dystrophy has two types, both of which involve muscle weakness. There are three types of sodium channelopathies: congenital paramyotonia, familial hyperkalemia paralysis and fluctuating myotonia. The rest was first described by Ricker et al., it develops within 20–40 weeks after physical exercise, does not respond to cold, and accumulates potassium. The basic classification of myotonic disorders is presented in Table 3.
CELEBRATION OF MYOTONIA
In outpatient clinics, neurologists most often suffer from MD1, and sometimes from Thomsen’s disease or paramyotonia. Today there are no drugs that would be aimed at opening the chloride channels of skeletal muscles, so in case of myotonia, sodium channel blockers are most often used. This group of drugs includes mexiletine, procainamide, phenytoin and carbamazepine, which have been developed for the treatment of cardiac arrhythmias and epilepsy. They are prescribed for the control of this disease, but we still don’t know how adequate the stench is. Sodium channel blockers tend to reduce the potency and potency of the muscles. In case of myotonic disorders without meatal weakness, the side effects of the generic drugs are not excessive, which cannot be said about MD1 and MD2. In such patients, the main problems are caused not so much by myotonia, but by weakness. The ideal pharmacological agent can be differentiated from the manifestation of illness.
Treatment of Thomsen's illness
The fragments of this illness do not blame weakness as such, the main misery of the patient is the subsequent ruin of the inheritance of unworthy meats soon. If you would like to change the ailments, for this purpose it is sufficient to use sodium channel blockers, such as mexiletine or phenytoin, in short courses during the period of intense hearing activity, in other situations This is a trivial, ineffective method.
Treating paramyotonia
Myotonia and muscle weakness with paramyotonia worsen in cold climates, so such patients can also take mexiletine. They are not to blame for the progressive muscle weakness, and the illness lives almost normally against the backdrop of seasonal courses of the named drug.
Treatment of myotonic dystrophy
In MD1 and MD2, there are three main problems: 1) myotonia, 2) muscle weakness and 3) systemic manifestations such as cataracts, cardiovascular diabetes, cardiac arrhythmias, etc. (Table 4).
Table 4. Treatment of myotonic dystrophy type 1
| Treatment of myotonia | Treatment for meat weakness | Elimination of systemic manifestations |
| Prokainamid Mexiletine Phenytoin Carbamazepine Dehydroepiandrosterone sulfate (DHEAS) | There is no effective treatment Pevne polіtsheniya — with the use of creatine and DHEAS | 1. Cataract - surgery and implantation of piece crystals. 2. Ptosis - blepharoplasty. 3. Cardiac arrhythmias - upon consumption, implantation of water rhythm. 4. Blood diabetes is a metaphor. 5. Hypothyroidism - thyroxine. 6. Hypogonadism - hormone therapy must not be carried out |
Nowadays, a variety of sodium channel blockers have been used in healthy myotonia. Proteus with myotonic dystrophy, their side effects as soon as the muscle weakness progresses, becomes a big problem.
There are no selective mediators that reach chlorine channels, and that is why it is so important to develop drugs that replace myotonia, rather than affect the strength of the muscles. The candidate agent in this case is dehydroepiandrosterone sulfate (DHEAS). Sugino et al. This steroid was used at MD1 at a dose of 250 mg/dose internally and myotonic symptoms were changed and the activity of everyday functioning was improved, and muscle strength did not change.
Therapeutic investigations aimed at improving muscle mass in MD
Creatine monohydrate (CM) was studied by Tarnopolsly et al. in 34 patients with MD at a dose of 5 g/day for 4 months in parallel with placebo. The average grip strength in the follow-up group did not change, the functional indicators of the legs were lost without change.
A double-blind, placebo-controlled follow-up study of CM therapy conducted by Schneider-Gold et al. In 20 patients with MD2 over a period of 3 months, there was no significant increase in muscle strength, but in 2 patients, muscle pain changed - a symptom that creates significant discomfort in this population.
CM leakage was assessed in an open-label study of 20 Japanese patients with MD, 14 of whom had small MD1. 12 sicknesses indicated a subjective increase in muscle strength. It is important to remember the side effects of this drug that may occur during severe congestion, including drowsiness, diarrhea, and excessive sweating.
Therapy of systemic manifestations
Treatment of cataracts: post-operative complications cause decreased vision
It is important to evaluate visual impairment after surgical treatment of cataracts in MD1. After a few months, such patients tend to develop postoperative contractures caused by fibrous metaplasia of the epithelial cells of the crystalline from the anterior capsule, so the ophthalmologist must always Please inform about the main diagnosis.
Treatment of myopathic ptosis
Myopathic ptosis is detected in MD1, mitochondrial myopathies and oculopharyngeal myocardial dystrophy. This is achieved through surgical ophthalmology using upper blepharoplasty, in which a physiological constriction is formed between the eyebrow and upper eyelid. Burnstine and Putterman treated 6 patients without any postoperative complications such as lagophthalmos, corneal keratopathy and xerophthalmia.
Treatment of cardiac arrhythmias using the method of preventing rapt death
To identify raptic death due to cardiac conduction defects and arrhythmia in MD, it is important to perform ECG, Holter monitoring and echocardiography. If the ECG shows a shortening of the PR interval, then calculating the HV interval by identifying the intranodal conduction block (with an HV of more than 70 ms) can help in making decisions regarding water implantation I rhythm. Lazarus et al. 49 patients with MD were monitored for 53.5 months and in 41 cases (83.7%) they developed raptoarrhythmia, in 21 cases - continuous atrioventricular block, in 4 cases - sinoatrial block, in 25 cases - before heart, and 13 episodes - Schlunochkova tachyarrhythmia. During the pre-trial period, 10 patients died, of which 4 died from rape. The authors recommend implantation of cardiac aqueous rhythm in MD, when on the ECG the HV interval exceeds 70 ms, in order to avoid rapid death.
Cure treatment for diabetes
In MD, insulin resistance and hyperinsulinism are evident. It is reported that metaformin can control hyperglycemia in MD1, since this agent enhances the removal of glucose from meats.
Soothing supernatural daytime sleepiness
To eliminate excessive daytime sleepiness, modafinil, which causes stagnation in narcolepsy, was administered to patients with MD for 4 days in parallel with the placebo group. This agent realized its effect and was not associated with any cardiac-vascular abnormalities.
Experimental therapeutic studies targeting changes in CTG nucleotide repeats: promising avenues for treating MD1
Furling et al. Victimized gene therapy was used to treat pathological changes in the inheritance of MD myoblasts, stagnant and protylage-directed RNA, expanded in vitro with a similar retrovirus. Nina knows that this illness is due to the inheritance of the CTG nucleotide repeat in the untranslated division of the protein kinase gene. This results in the accumulation of pre-mRNA from partial CUG nucleotide repeats in the cell nucleus and defects in the splicing of pre-mRNA chloride channels, which leads to atypical formation of these channels and, in the brain, myotonia. The early success of this type of gene therapy in the laboratory provides support for its potential to be developed in clinical populations in the future.
The experiment also revealed that in patients with MD1, CTG repeats change under the influence of various chemotherapy agents - ethylmethanesulfonate, mitomycin C, mitoxantrone and doxorubicin. Obviously, in addition to the above-mentioned illness, this approach can cause congestion in 17 other neurological illnesses, including various forms of spinocerebellar degeneration.
Prepared by Yuriy Matvienko