A description is given of the forms of hydrocephalus that can be incidental findings on MRI/CT of the brain - primary hydrocephalus and conditions with which a differential diagnosis must be made. Information about benign intracranial hypertension (BIH), normotensive and replacement hydrocephalus is presented to the extent that is necessary for a neurologist in outpatient practice to make decisions and explain to the patient the essence of his condition. The structure of the document reflects the tasks facing it. You can get acquainted with the question in more detail using the links in the relevant sections of the text. The clinical picture of intracranial hypertension consists of general cerebral and focal symptoms. Intracranial hypertension is characterized by the absence of pathognomonic disorders. In a typical clinical picture, a triad stands out: headache, vomiting, congestion in the fundus. Increased intracranial pressure is often associated with hydrocephalus, a disorder involving the accumulation of excess cerebrospinal fluid (CSF) in the cerebral ventricles and/or subarachnoid spaces, due to an imbalance between secretion and absorption, which is accompanied by dilation of the ventricles and/or subarachnoid spaces. The set of disorders in patients may be similar to the clinical picture of other lesions of the nervous system: - disseminated demyelinating focal lesions of the brain substance and cranial nerves, - focal lesions of the brain stem with involvement of the medial longitudinal fasciculus and the development of disorders of consciousness - space-occupying formations of the brain with general cerebral changes, focal symptoms and symptoms of damage to the cranial nerves, - conditions with diffuse brain damage - encephalopathy. — neuroinfections (congenital syphilis, cytomegalovirus infection, mumps, etc.) — thrombosis of the sinuses and veins of the brain. Asymptomatic cases of intracranial hypertension (ICH) are accompanied by nonspecific complaints - dizziness, fatigue. The variety of variants of the clinical picture, both in severity and in the set of symptoms, is the reason for the overdiagnosis of hypertensive-hydrocephalic syndrome, both in adult and pediatric neurological practice. An additional harmful effect is the high rate of false-positive data on dilation of the ventricular system when using echoencephaloscopy. Doctors can claim that a patient has ICH if rheoencephalography, duplex scanning of the brachiocephalic arteries, or transcranial Doppler sonography reveals venous drainage from the cranial cavity.
Imaging signs of hydrocephalus with increased ICP include: An increase in the size of the inferior horns of the lateral ventricles by more than 2 cm with the absence of visualization of the subarachnoid spaces of the convexital areas, interhemispheric and lateral fissures of the brain; Balloon-shaped dilatation of the anterior horns of the lateral ventricles (Mickey Mouse symptom) and the third ventricle; Periventricular decrease in tissue density seen on CT or increased T2 signal seen on magnetic resonance imaging (MRI) as a result of transependymal infiltration or migration of cerebrospinal fluid. In addition to structural changes, the clinical manifestations of hydrocephalus are taken into account. The last clarification is necessary, since taking into account only structural changes does not allow us to classify disorders of liquorodynamics without changing the configuration of the ventricles as hydrocephalus, for example, benign intracranial hypertension (BIH).
NORMOTENSIVE HYDROCEPHALUS
Normal pressure hydrocephalus (NPH) is associated with impaired CSF absorption, and dilatation of the cerebral ventricles develops in the presence of normal intracranial pressure.
EPIDEMIOLOGY
The prevalence of NG is 1-2 cases per 1,000,000 people. In the practice of a neurologist specializing in patients with extrapyramidal diseases, as a rule, no more than a dozen patients are recorded per year. This type of hydrocephalus is more common in older people. The condition should be excluded in persons over 60 years of age with a combination of cognitive impairment (dementia), pelvic organ dysfunction (usually urinary incontinence) and walking impairment (lower body parkinsonism) - the Hakim-Adams triad. Due to the fact that in a significant proportion of cases, bypass surgery in the early stages leads to improvement in walking, it is important to suspect and confirm this condition in a timely manner.
CLINIC
The structure of cognitive impairment is dominated by frontal-subcortical disorders: decreased activity, apathy, and behavioral disorders. Walking disorders have been described as magnetic gait, gait apraxia, and frontal ataxia. Patients experience the greatest difficulty when starting to walk. The area of support is increased, the length and height of the step is reduced, the smoothness of movements is impaired, and there is a progressive slowdown in walking with each step. Patients always have postural instability; often, upon questioning, you can find out that there have been falls before.
DIFFERENTIAL DIAGNOSIS
However, other diseases with cognitive and motor impairments may have a similar pattern of impairments. When carrying out differential diagnosis, the following are considered: vascular dementia (discirculatory encephalopathy stage III), Parkinson's disease with dementia and dementia with Lewy bodies, Alzheimer's disease. The main diagnostic method is MRI of the brain. The examination reveals the expansion of the lateral ventricles, the rounded shape of their anterior horns, and the smoothness of the relief of the cerebral cortex. It is important to use the Evans ventricular-hemispheric index, which is the ratio of the distance between the most distant points of the anterior horns of the lateral ventricles to the largest internal diameter of the skull. Ventriculomegaly is diagnosed if the index exceeds 0.31. NG is characterized by changes in the periventricular white matter, similar to leukoaraiosis (see above). Their severity correlates with the degree of cognitive impairment].
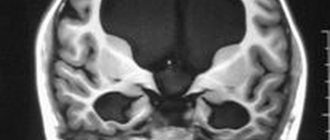
Figure 2 MRI signs of cerebral atrophy (A) in Alzheimer's disease and (B) normal pressure hydrocephalus
At first glance, the images are quite similar, but the image on the right shows the rounded shape of the horns of the lateral ventricles and the smoothness of the sulci of the cerebral hemispheres.
Figure 3 Gliotic and atrophic changes after traumatic brain injury, replacement hydrocephalus
Symptoms and diagnosis of minor external hydrocephalus
Moderate external hydrocephalus at the first stage of the disease may not manifest itself with clinical symptoms. With a small amount of brain matter, the body is able to independently restore fluid circulation. As the disease progresses, pressure on the brain increases and severe external hydrocephalus of the brain occurs. It manifests itself with the following symptoms:
- migraine-like headache;
- nausea and vomiting;
- visual impairment (double vision);
- weakness, increased fatigue.
If the cause of moderate external hydrocephalus of the brain is congenital developmental anomalies, the disease begins to manifest itself immediately after the birth of the child: the volume of the head increases, an enhanced venous pattern is visible on the forehead and face, and the fontanel swells. Children have poor appetite, they lag behind their peers in physical and mental development, and become apathetic and inhibited.
To diagnose moderate external hydrocephalus, neurologists at the Yusupov Hospital use the following diagnostic methods:
- magnetic resonance and computed tomography;
- magnetic resonance angiography;
- ultrasound examination of the brain;
- X-ray of the brain (craniography);
- laboratory tests for the presence of viruses.
The most informative is magnetic resonance imaging. The MR picture of mild internal hydrocephalus is clearly visible, which makes it possible to determine and diagnose the disease. Magnetic resonance imaging makes it possible to distinguish a significant decrease in brain volume and the filling of the resulting space with cerebrospinal fluid, neoplasms, adhesions, and blood clots.
If there are signs of increased intracranial pressure, patients undergo a lumbar puncture and 40 ml of cerebrospinal fluid is collected, which is sent for laboratory testing. If the patient's condition temporarily improves after the procedure, this allows neurosurgeons to assume a good prognosis after surgery.
REPLACEMENT HYDROCEPHALUS
The terms “replacement hydrocephalus” and ex-vacuo hydrocephalus denote expansion of the ventricles of the brain of a secondary nature, due to brain atrophy - a decrease in the volume of brain tissue. Replacement hydrocephalus is not accompanied by disturbances in cerebrospinal fluid dynamics, including increased intracranial pressure. Therefore, the relationship of this condition to hydrocephalus is disputed. Replacement hydrocephalus is more often encountered in elderly patients with chronic vascular and/or toxic damage to the brain, consequences of traumatic brain injury. In the last two cases, a selective decrease in the volume of individual brain regions is possible: atrophy of the cerebellum and frontal lobes, atrophy of brain regions in the projection of the bruise. Replacement hydrocephalus does not have a clear correlation with neurological disorders and does not require special treatment.
Against the background of terminological disagreements on the issue, there are several classifications that do not contradict each other:
- communicating and non-communicating;
- obstructive and aresorptive;
- congenital and acquired;
- genetic or associated with malformations of the central nervous system;
- isolated intraventricular-obstructive and extraventricular simple and complicated.
The term “compensated hydrocephalus” describes conditions without progressive enlargement of the ventricles of the brain; otherwise, uncompensated hydrocephalus is diagnosed. “External hydrocephalus” or “benign enlargement of the subarachnoid spaces” is an excessive accumulation of fluid, a condition quite often associated with familial macrocephaly (the size of the skull is larger than the size of the brain, while there are no disturbances in cerebrospinal fluid dynamics, including increased CSF pressure).
- The term "hydrocephalus" is used to refer to a group of conditions that are distinguishable from each other by CT or MRI of the brain.
- Judging hydrocephalus without CT or MRI data may be erroneous.
- In children, hydrocephalus is usually associated with increased intracranial pressure (ICP). In most cases, it is caused by excess production of CSF, which accumulates in the ventricles of the brain due to disturbances in its circulation (obstructive or non-communicating hydrocephalus). Less commonly, CSF accumulates due to malabsorption (communicating hydrocephalus).
- In adults, unlike children, forms of hydrocephalus without increased ICP are much more common.
- Since hydrocephalus can not only be an isolated condition, but also accompanies certain neurological diseases, the exact prevalence of the syndrome is not known.
- To date, no unified classification has been created that covers the causes of hydrocephalus in patients of different ages.
- Due to the high “stigmatizing” significance of the diagnosis of “hydrocephalus” for patients, before announcing the final diagnosis and prescribing treatment, it is necessary to conduct all the studies necessary to establish the nosological affiliation of the changes identified in the brain.
- The patient must have complete and adequate information about the disease, which is most important in relation to benign and treatable forms.
Reasons for the development of pathology
The human brain consists of soft tissues located in the skull. To protect against damage, cerebrospinal fluid circulates in the cavity - the liquid fills the internal ventricles and grooves. When a person is healthy, the inflow and outflow of cerebrospinal fluid is balanced. The performance of its functions does not affect the patient’s health. If disturbances occur due to the development of tumors, injuries and infections, intracranial pressure increases and the process of cerebrospinal fluid movement is disrupted, causing changes in brain function and neurological manifestations.
Hydrocephalus can develop due to a stroke or tumor development.
Stages of development
External hydrocephalus has 3 stages of development, each of them has its own characteristics:
- Mild - the size of the dropsy is small, the body itself tries to cope with disturbances in the flow of CSF. A person usually feels a headache that is not too intense, he periodically feels dizzy, feels slightly worse, and sometimes gets dark in his eyes;
- Moderate – manifestations become more noticeable, the intensity of headaches increases, especially during physical activity. Possible disturbances in visual function, rapid onset of fatigue, pressure changes, depression and severe irritability;
- Severe - at this stage, hydrocephalus of the brain can cause seizures, apathetic state, fainting, apathy, and also lead to the development of conditions in which a person is no longer capable of self-care.
At the initial stages of development of the pathology, neurological symptoms may be absent. They appear due to organic processes that occur in the cerebral substance, as well as against the background of circulatory disorders and atrophy of some areas.
Pathogenesis
The disease provokes expansion of the cerebral ventricles for various reasons. The main provocateur is a violation of the outflow of cerebrospinal fluid.
The process of cerebrospinal fluid circulation
The choroid plexuses produce approximately 600–700 ml of cerebrospinal fluid per day. It enters the central canal through special openings, washing the brain and then the spinal cord. Reabsorption occurs through the cerebral hemispheres through the venous sinuses.
Brain damage process
Excessive pressure of the cerebrospinal fluid provokes its leakage into the surrounding substance, which causes the development of edema. The dilated ventricles begin to compress the brain tissue.
The white matter takes the brunt of the attack, causing destruction of the myelin sheaths that transmit nerve impulses to the body.
Up to a certain point, such changes are reversible—after timely surgery, it is possible to almost completely restore neurological functions. Otherwise, atrophy of the brain substance develops, causing spastic paralysis, and the person ceases to control the functioning of the pelvic organs.
In infants, under the influence of such excess pressure, there is a rupture of adhesions inside the subarachnoid space, which opens the way for the outflow of cerebrospinal fluid and self-healing. In advanced situations, brain tissue ruptures. Timely treatment can prevent the development of neurological disorders.
Symptoms of the disease in adults
Hydrocephalus in adults manifests itself:
- Headaches for which neither sleep nor painkillers can help;
- Nausea, feeling of approaching vomiting;
- Feeling of constant fatigue;
- Sudden changes in mood, tendency to irritability;
- Changes in behavior;
- Fogging of consciousness, difficulties with memory, the thinking process;
- Balance imbalance;
- Inability to control urination;
- Seizures and convulsions;
- Sleep disorders;
- Problems with appetite;
- Blurred vision, a feeling of double vision, movement of the eyeballs downwards.
Headache with hydrocephalus intensifies when changing a horizontal position to a vertical one. Fluctuations in blood pressure are possible. With normal pressure hydrocephalus, signs of dementia, urinary incontinence, and gait disturbances appear in combination with pronounced dilatation of the cerebral ventricles, but without an increase in CSF pressure.
Hydrocephalus in children
Signs of hydrocephalus are determined by the person’s age and stage of the disease. In children, including newborns, the development of pathology may be indicated by capricious behavior and poor appetite, marbled skin and slow reactions, eyelid retraction and gaze almost always directed downward, as well as swelling of the fontanelle and excessively enlarged head size.
It is the size and shape of a child’s head that often indicates pathological processes. By the age of six months, babies with hydrocephalus have a head circumference greater than the chest, the skull becomes oblong, pear-shaped, and this is noticeable to the naked eye.
With hydrocephalus in children, the normal functioning of the brain is blocked, which leads to a lag in mental, physical, and mental development. The risk of pathology increases in newborns born prematurely with low body weight. The cause may also be intracranial birth injuries or infectious diseases suffered by the mother during pregnancy.
A child with this disease begins to roll over, hold his head up, and sit up later than his peers. In severe forms of the pathology, these skills are not formed, muscle strength in the limbs decreases up to paralysis, and muscle tone increases. After fusion of the fontanelles, a severe headache begins, often in the morning, frequent vomiting, and nosebleeds.
Diagnosis of hydrocephalus
Signs of the disease are often detected while the fetus is still in the womb during ultrasound. Then the disease is diagnosed by a doctor after the baby is born. The main indicator for determining pathology is the large diameter of the skull. In older children, as in adults, the doctor evaluates the patient’s thinking, his gait, the presence of signs of urinary incontinence, and the condition of the ventricles using MRI images.
To verify the presence of congenital hydrocephalus, CT or MRI are used, which allow:
- assess the state of the brain;
- identify excess cerebrospinal fluid volume;
- detect increased cerebrospinal fluid pressure;
- see structural changes in brain tissue.
Normal pressure hydrocephalus is more difficult to identify because its symptoms are largely similar to neurodegenerative processes. This variant of pathology is diagnosed according to the following signs:
- walking disorder;
- mental disorders;
- urinary incontinence;
- excess volume of cerebrospinal fluid.
With any variant of the disease, it is important to make an accurate diagnosis in a timely manner so as not to be late with surgical intervention that will eliminate the severity of symptoms or reduce their intensity.
To find out how effective the operation will be, some additional measures are necessary:
- Lumbar puncture. A small amount of cerebrospinal fluid is removed through a puncture made in the lower back. The cerebrospinal fluid pressure is then measured. The procedure allows you to slightly reduce it in the cerebral ventricles in order to neutralize severe symptoms.
- Lumbar drainage. It is necessary when the previous procedure was ineffective. A catheter is installed between the lumbar vertebrae, through which the cerebrospinal fluid comes out for several days. All this time the patient is observed in the hospital. Antibiotics are administered to prevent infection.
- Infusion test. This is a stress diagnostic option that helps assess how much the brain is able to absorb cerebrospinal fluid.
- ICP measurement. To perform the procedure, a hole is drilled into the skull bone. A sensor in the form of a fiber-optic cable is installed through it. The event is carried out while the patient is in the hospital for at least 24 hours. The sensor detects surges in intracranial pressure, sending values to a recording device.
When an event involves the need to measure ICP, various sensor options are used:
- Intraventricular catheter. This is the most accurate way to measure. The device is brought to the lateral cerebral ventricle through a hole drilled in the skull bone. The instrument helps to simultaneously ensure the drainage of excess fluid.
- Subdural sensor. The device is attached under the dura mater of the brain. It is used if there is an urgent need to check ICP. The method allows you to quickly identify changes in ICP.
- Epidural sensor. The instrument is attached between the dura mater of the brain and the cranial bone, having previously drilled a hole in it. The procedure is less traumatic than others, but has a significant drawback - excess cerebrospinal fluid cannot be drained during the procedure.
When installing sensors, local anesthesia is required. It is also sometimes necessary to additionally inject the patient with sedative medications in order to reduce anxiety and relax the patient as much as possible.
Typically, sensors used to measure ICP are administered to people in intensive care, often in the most critical condition. The necessary indications for such an event are severe trauma to the skull, pathologies of the brain that cause swelling and depression of consciousness up to a coma. In patients who have undergone brain surgery, such a monitoring sensor helps detect increasing swelling.
Drainage of cerebrospinal fluid also helps to reduce high ICP. It is performed by installing a ventricular catheter, intravenous injection of certain medications, and changing the method of ventilation (in a situation where the patient breathes through a tube inserted into the trachea). Normal ICP is 1–20.
Installing sensors is a risky undertaking, as it can cause the following complications if done incorrectly:
- bleeding;
- irreversible damage in a situation with prohibitive ICP values;
- “herniation” of the brain;
- damage to brain tissue during catheter insertion;
- infectious complications;
- inability to accurately determine the location of the ventricle in order to place a catheter to it;
- other risks present during general anesthesia of the patient.
Diagnosis of dropsy of the brain
In infancy, a visual examination is sometimes sufficient to determine the nature of the pathology: the doctor, by examining the baby’s physiological parameters and listening to the parents’ complaints, can make a preliminary diagnosis at the initial appointment.
To clarify the disease in children with an open fontanel, including to identify pathology during intrauterine development, ultrasound is used to assess the degree of enlargement of the ventricles. Additional methods are:
- fluoroscopy;
- computed and magnetic resonance imaging;
- lumbar puncture, necessary for a detailed analysis of the cerebrospinal fluid.
A child with suspected hydrocephalus must be examined by an ophthalmologist or pediatrician; if necessary, concomitant diseases may require consultation with a cardiologist, surgeon, oncologist and other specialists.
What is hydrocephalus?
Nutrition of brain structures is carried out through a direct current of cerebrospinal fluid. Liquor circulates along a certain channel, ensuring continuous cerebral metabolism. Cerebrospinal fluid is needed for:
- protecting brain tissue from mechanical stress;
- ensuring a constant level of electrolytes;
- maintaining the balance of acids and alkalis;
- complete immunobiological protection.
With hydrocephalus, there is a disturbance in the production, outflow and circulation of cerebrospinal fluid in the brain tissues. The disease is characterized by pathological accumulations of cerebrospinal fluid, which increases intracranial pressure. Clinically, hydrocephalus occurs in a severe form, with frequent attacks of the neurological type. A long-term pathological condition leads to the formation of secondary changes in brain tissue, which are usually irreversible. As a result of an uncontrolled course, hydrocephalus becomes the cause of death of the patient. Popularly, the disease has received a second name - dropsy of the brain.
Treatment of hydrocephalus
The option of surgical intervention for hydrocephalus is quite effective. Two types of operations are used: neuroendoscopy or liquor shunting. They are performed by a neurosurgeon, a specialist who can correct problems in the brain or spinal cord, as well as the peripheral nerve ending system.
Bypass surgery
In this type of surgery, a thin tube is inserted into the brain ventricle. Excess cerebrospinal fluid flows through it to another anatomical zone of the body. If the second end of the drainage system is placed in the peritoneum, the shunt is called ventriculoperitoneal. Then the excess cerebrospinal fluid is absorbed by the abdominal cavity and then enters the blood.
When the draining end is directed into the cardiac chamber, the shunt is called ventriculoatrial. This option is practiced during surgery for children, because their increase in height does not affect the functioning of the organ as much, so the drainage does not have to be changed as often as the ventriculoperitoneal system.
Occasionally, lumboperitoneal shunts are also used. With the help of such drainage, cerebrospinal fluid is drained from the lumbar region into the peritoneal cavity.
Any drainage system contains a valve that is set to a certain capacity. It is selected for a specific patient, taking into account the patient’s cerebrospinal fluid pressure. The doctor performing the surgery determines these values in advance by installing a suitable valve, which then looks like a “bump” protruding under the skin on the head.
Currently, neurosurgeons have two types of valves for drainage systems:
- With predefined characteristics that define a specific throughput.
- Adjustable magnetic fixtures. When choosing them, the doctor remotely, using special equipment, without performing additional incisions, changes the pressure in the device to achieve an optimal result. Thanks to this, it is possible to neutralize adverse side effects in the form of insufficient or excessive cerebrospinal fluid pressure.
Bypass surgery is performed under general anesthesia. The procedure lasts 1–2 hours and after it the patient is kept in the hospital for several days. If the outflow through the shunt is disrupted or the patient becomes infected, a repeat procedure is sometimes performed.
Neuroendoscopy
This operation is an excellent alternative to bypass surgery. Without taking steps to install drainage, the neurosurgeon forms a hole directly in the wall of the cerebral ventricle, after which he creates a bypass path from the vessel through which cerebrospinal fluid flows freely to the surface. There it is absorbed by the brain tissue without obstacles.
This procedure is not universal - it cannot be done on all patients, although this method is often used if the natural cerebrospinal fluid pathways are blocked. In this case, the cerebrospinal fluid flows through the created hole, successfully bypassing all blocked vessels.
The endoscopic procedure is done under general anesthesia. First, the neurosurgeon makes a burr hole with a diameter of 1 cm on the skull. Then, using an endoscope, he examines the inside of the cerebral ventricles. Through the internal channel of the instrument, surgical instruments are inserted, which are used to perform an operation inside the brain. When the endoscope reaches the third ventricle, the doctor creates a hole in its lower wall through which the cerebrospinal fluid penetrates into the subarachnoid cavity. After removing the device, first the aponeurosis is sutured, and then the skin on the skull. The duration of the operation is approximately an hour.
The risk of infection with such an intervention is significantly lower than with cerebrospinal fluid bypass. Neuroendoscopy does not have significant advantages over drainage surgery over long periods of patient observation. After such an intervention, hydrocephalus can also develop again after a few years.
Actions for normal pressure hydrocephalus
When normal pressure hydrocephalus (a common occurrence in older people) is diagnosed, the patient's condition can be improved by performing a cerebrospinal fluid shunt. Although surgery is not effective for every patient. Due to the considerable risks that accompany all operations, certain tests are required to assess how much the potential benefit outweighs the risk of negative consequences.
Almost 80% of patients diagnosed with normal pressure hydrocephalus experienced significant improvement after preliminary testing, so ventriculoperitoneal shunting was recommended for them. Significant clinical postoperative improvement occurs after a few weeks, sometimes even months. Only a timely correct diagnosis guarantees successful recovery even with many years of development of hydrocephalus.
Prognosis and prevention
It is quite difficult to predict anything in those who suffer from hydrocephalus, although there is a certain connection between the outcome of the disease and the reasons that caused it. Several factors influence the likelihood of pathology:
- presence of concomitant diseases;
- the period between the appearance of the first signs and the establishment of an accurate diagnosis;
- adequacy of the treatment.
Until now, experts have not been able to figure out by what amount it is necessary to reduce ICP during surgery in order to minimize complications or prevent brain damage. Patients, together with their relatives, must understand that pathology harms both mental and physical development. Although after rehabilitation treatment, most children can be brought to a state where they are able to study educational programs and have a minimum of restrictions regarding the quality of life.
The treatment process, which involves doctors of various specialties, and then effective rehabilitation measures coupled with classes conducted by teachers, are extremely important for achieving a positive result. However, you must always remember that the lack of treatment contributes to the progression of hydrocephalus, which is why the disease can be fatal. Only early diagnosis and then adequate treatment guarantee the child’s recovery.
Signs of hydrocephalus, where the cerebrospinal fluid has normal pressure, often progress with age if not properly treated. But sometimes patients suddenly experience unexpected improvements. The effectiveness of organizing liquor shunting measures is not always guaranteed: it depends on the severity of the pathology, the age of the patient, and the reasons that provoked the development of the disease.
Sometimes, thanks to a complex of timely treatment, it is possible to achieve complete restoration of lost neurological functions. Therefore, the prognosis of how the pathology will proceed further when a shunt system is installed depends only on the patient’s body’s perception of such intervention. The main complications are blockage, infection or disconnection of the system:
- The first complication develops due to the entry of body particles into the drains. Blockage can also be caused by a malfunction of the valve device. Typically, liquor shunt systems operate for 5–10 years. If a blockage occurs, a complete replacement of the drainage is required.
- Infection develops when bacteria enter the tubes. Such a complication is likely during surgery, at the time of installation of the system, and also due to the migration of pathogenic microorganisms. Liqueur bypass systems are made of silicone. This material itself is foreign to the body, which makes it impossible to cure the infection with antibiotics. If such a complication is detected, immediate removal of the shunt system and a further course of therapy are required. Only after complete recovery is a new system implanted. To reduce the risk, it is recommended to use silver-impregnated equipment.
- Disconnection can occur when the seal in the tubes is broken. The cause is the movement of the shunt inside the patient's body, which often occurs in children due to natural growth. When system disconnection occurs, it is necessary to organize immediate surgical intervention, which involves checking the functionality of the shunt system and correcting areas that have lost their tightness.
Complications such as cerebral hemorrhage occur much less frequently (they are likely at the time of catheter installation), as well as disconnection of the catheter, after which it moves into the cavity of the cerebral ventricle. When such an event occurs, it is not always possible to remove the foreign object, so the associated infection becomes the cause of epilepsy or convulsive seizures.
Most patients who have undergone surgery for such an unpleasant reason lead an almost comfortable lifestyle. Almost 10% of them get rid of foreign implanted systems over time.
Nowadays, prevention of pathologies that can provoke hydrocephalus is carried out everywhere. To prevent meningococcal infection, which leads to infectious meningitis, active vaccination is used, and antibacterial agents are prescribed to those who have been in contact with an infected person to minimize the risk of infection. To prevent the possibility of rupture of identified arterial aneurysms in the brain, which cause subarachnoid hemorrhage, surgical interventions are organized to help exclude the aneurysm from the general blood flow.
Classification
Based on the openness of the cerebrospinal fluid outflow pathways, hydrocephalus occurs:
- closed;
- communicating;
- substitutive.
According to the characteristics of the deformation of the outflow tract:
- internal;
- external;
- mixed.
By type of cerebrospinal fluid pressure:
- hypotensive;
- hypertensive;
- normotensive.
By etiology:
- congenital;
- after the inflammatory process;
- tumor;
- vascular;
- idiopathic.
Other types of classification:
- with the flow;
- by compensation phase;
- by activity;
- according to the speed of development.
Symptoms of hydrocephalus
Typically, the manifestations of the problem depend on the age of the patient and the type of hydrocephalus. Newborns have noticeable characteristic appearance features:
- increased head diameter;
- the skin is thin, the veins are visible;
- the fontanel protrudes;
- eyes are directed downwards.
Clinically, this pathology manifests itself:
- frequent vomiting;
- lack of appetite;
- excessive irritability;
- drowsiness;
- decrease or increase in muscle tone of the limbs.
The acquired pathology is manifested by frequent headaches, especially severe after a night's sleep. This is due to the fact that when positioned horizontally, cerebrospinal fluid flows more slowly, it accumulates, bursting the brain tissue. The condition improves after standing up, although this improvement gradually disappears as the disease progresses.
Other manifestations include:
- neck pain;
- drowsiness;
- mental disorders;
- memory impairment;
- the appearance of a “veil” before the eyes;
- lack of coordination;
- nausea;
- walking disorder;
- epilepsy;
- urinary incontinence, sometimes involuntary bowel movements.
Normal pressure hydrocephalus is a disease of older people. It is characterized by the following symptoms:
- walking disorders;
- deterioration of intellectual abilities;
- urinary incontinence.
The first thing to break is gait. It becomes difficult to start moving. As the disease progresses, instability becomes more pronounced and a person may suddenly fall when changing direction. Walking disorder is accompanied by urinary incontinence: first there is a frequent urge that requires immediate emptying, then control of this function is completely lost.
The disease also affects thought processes:
- reaction worsens;
- the patient is not able to quickly respond to changing situations;
- a failure occurs when trying to process the received information.