Hydrocephalus is an excessive accumulation of cerebrospinal fluid in the cranial cavity, which results in an increase in the size of the subarachnoid spaces, basal cisterns, and ventricles of the brain. All conditions have been created for the treatment of patients with hydrocephalus at the Yusupov Hospital. The neurology clinic employs candidates and doctors of medical sciences, doctors of the highest category. Neurologists have the knowledge and experience to quickly diagnose the disease and provide adequate therapy.
Causes of hydrocephalus
Hydrocephalus develops due to the accumulation of cerebrospinal fluid in the cerebrospinal fluid system of the brain in the event of the production of an excess amount of cerebrospinal fluid, impaired absorption or disturbance of the circulation of cerebrospinal fluid. In case of exposure to damaging factors on the fetal brain during intrauterine development, congenital hydrocephalus occurs. Acquired hydrocephalus develops under the influence of various pathological mechanisms after the birth of a child.
The following causes of congenital hydrocephalus are known:
- intrauterine infections (hydrocephalus, toxoplasmosis, cytomegaly, syphilis);
- birth injury;
- defects in the development of the cerebrospinal fluid system (atresia of the foramina of Magendie and Luschka, stenosis of the Sylvian aqueduct, structural defects of the subarachnoid space, Dandy-Walker syndrome);
- developmental anomalies of the skull and spine (congenital basilar impression, Chiari malformation).
Acquired hydrocephalus occurs as a result of inflammatory processes of the brain and its membranes, traumatic brain injuries, acute and chronic vascular disorders. Hydrocephalus in adults often develops against the background of a colloid cyst of the third ventricle and intracerebral tumors (germinomas, astrocytomas, ganglioneuromas) growing into the ventricles of the brain or compressing the cerebrospinal fluid tract, disrupting the normal circulation of cerebrospinal fluid and its outflow from the cranial cavity.
Make an appointment
Anatomy and physiology
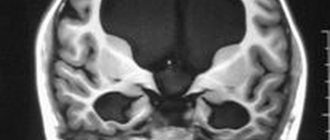
In order to better know and understand the disease, we will give you some information about the anatomy of the skull, the structure of the brain, as well as the process of formation and absorption of cerebrospinal fluid (Fig. 1). The brain occupies most of the cranial cavity. It is penetrated by a large number of blood vessels and is surrounded by cerebrospinal fluid as a buffer. The fluid is located in 4 cavities (ventricles) located inside the brain. The ventricles have delicate structures known as villous plexuses (choroid plexuses). These structures produce a significant amount of CSF - about 500 ml per day. The fluid circulates continuously and contains a large number of substances essential for nutrition and ensuring the normal functioning of the nervous system.
CSF also provides a protective cushion for the brain. CSF circulates in the ventricular system and is removed through 3 holes in the 4th ventricle and then enters the subarachnoid space surrounding the brain and spinal cord.
CSF constantly circulates in the brain and spinal cord, constantly being in the process of a) formation, b) circulation and c) absorption. In a healthy body these processes are balanced. Hydrocephalus develops if CSF is not cleared from the ventricular system through the cerebrospinal fluid tract. Less commonly, hydrocephalus is caused by excess production of CSF, such as with villous plexus papilloma.
Types of hydrocephalus in adults
There are open (communicating), closed (occlusive) and replacement hydrocephalus. Open hydrocephalus of the brain in adults involves free communication of spaces through which cerebrospinal fluid circulates. It develops when there is an imbalance in production and reabsorption of cerebrospinal fluid. There are hyperproductive, aresorptive and mixed forms of hydrocephalus.
Replacement hydrocephalus can be a consequence of physiological aging of the body or develop in pathological conditions of the central nervous system, accompanied by atrophic changes (Alzheimer's disease, Creutzfeldt-Jakob disease). This form of the disease does not refer to true hydrocephalus, caused by impaired cerebrospinal fluid dynamics, but occurs as a result of the filling of “free” spaces inside the skull with cerebrospinal fluid.
In accordance with the location of the expanded cerebrospinal fluid spaces in relation to the brain tissue, the following types of hydrocephalus in adults are distinguished: internal (intraventricular), external (subarachnoid) and mixed. Depending on the level of intracranial hydrocephalus, hypertensive and normotensive hydrocephalus are distinguished. In functional and clinical aspects, progressive (increasing), stabilized (not changing over time) and regressive (decreasing) hydrocephalus are distinguished. Progressive hydrocephalus can be decompensated or subcompensated.
In acute hydrocephalus, no more than three days pass from the moment of the first symptoms of the disease to severe decompensation. Subacute progressive hydrocephalus develops within one month from the onset of the disease, and chronic hydrocephalus develops within a period of 3 weeks to 6 months.
Excessive drainage
Excessive drainage of cerebrospinal fluid occurs when the valve is incorrectly selected according to the pressure parameter. If the valve opening pressure is too low, it can cause excessive drainage, causing the cerebral ventricle to compress and deforming the brain tissue. The patient experiences headaches that are most severe when standing.
In addition, nausea, vomiting, drowsiness and nervous system disorders, in particular double vision, appear. School-age children experience a decline in mental abilities.
Symptoms of hydrocephalus in an adult
The accumulation of an excess amount of cerebrospinal fluid in a limited space of the cranium leads to an increase in intracranial pressure, which causes the most typical signs of hydrocephalus: intense headache that cannot be relieved by analgesics, nausea and vomiting, a feeling of pressure on the eyeballs.
These symptoms of hydrocephalus in an adult patient can occur acutely or increase gradually, having a transient nature at the onset of the disease. Replacement hydrocephalus often occurs without signs of increased intracranial pressure. Neurologists at the Yusupov Hospital detect it only after additional examination of the patient. Hydrocephalus of the brain in an adult in the photo has characteristic signs: an increase in the volume of the head and frontal bone.
In most cases, hydrocephalus in adults is accompanied by neurological symptoms. It is caused both by compression of brain structures by expanded cerebrospinal fluid spaces and by the underlying disease, which is the cause of the development of hydrocephalus. With hydrocephalus, vestibular disorders are observed: gait instability, dizziness, noise in the ears and head, nystagmus. Visual function is impaired: there is a significant decrease in visual acuity and loss of certain areas of the visual field. During ophthalmoscopy, ophthalmologists identify congested optic discs. With prolonged hydrocephalus, atrophy of the optic nerves develops.
Hydrocephalus in adults can occur with disturbances in the motor and sensory spheres:
- paresis and paralysis;
- decrease or complete loss of all types of sensitivity;
- increased tendon reflexes and muscle tone;
- formation of spastic contractures of the limbs.
Occlusive hydrocephalus, caused by impaired circulation of cerebrospinal fluid in the posterior cranial fossa, is characterized by symptoms of cerebellar ataxia: changes in handwriting, large-scale disproportionate movements, impaired gait and coordination.
Patients suffering from hydrocephalus develop mental disorders over time, manifested by disorders of the emotional-volitional sphere: neurasthenia, emotional instability, causeless euphoria with a rapid transition to a state of apathy. With a sharp increase in liquor pressure, patients begin to behave aggressively.
Blockage
The main type of complication is blockage of the system. Blockages can occur at any level of drainage. The holes in the ventricular catheter may become clogged with brain tissue or villous plexus tissue. It can also be blocked due to excessive contraction of the ventricular cavity due to too intense drainage of fluid from the ventricular cavity (constricted ventricle syndrome). Intestinal loops or necrotic tissue may adhere to the peritoneal catheter. Shunts inserted into a ventricle of the heart can become blocked by blood clots, pieces of brain matter, or tumor cells.
The shunt system may also be disconnected by disconnection of various elements of the shunt or by changes in the position of the catheter caused by the growth of the child. X-rays are necessary to check the integrity of the shunt.
Partial blockage of the system parts provokes the appearance of symptoms of increased intracranial pressure. Episodic headaches, nausea, apathy and decreased sensory functions may occur. Decreased performance at school or at work is the most common phenomenon in these conditions.
In case of complete blockage, symptoms develop more quickly (headaches, nausea, vomiting, blurred vision, loss of coordination and confusion). The patient falls into a stupor or coma. In such cases, urgent hospitalization is necessary for observation and appropriate treatment.
The surgeon performs a series of tests to locate and determine the extent of drainage blockage. Sometimes it is necessary to remove and replace part or all of the system.
Diagnosis of hydrocephalus
Neurologists at the Yusupov Hospital conduct a comprehensive examination of patients with hydrocephalus. Computed tomography currently occupies a dominant position among methods for diagnosing hydrocephalus. The procedure is carried out to determine the size and shape of the ventricles, identify developmental anomalies and neoplasms, cysts.
Magnetic resonance imaging allows you to determine the shape and severity of hydrocephalus. Using this diagnostic method, the cause of cerebral hydrocele is determined. Neurosonography helps assess the degree of expansion of the ventricles of the brain. The procedure is used only when diagnosing the disease in children with an open fontanelle, since the skull blocks ultrasound. Neurosonography is used to diagnose hydrocephalus in utero.
Cisternography is a research method in which a radioactive substance is injected into the cerebrospinal fluid. It is used to clarify the type of hydrocephalus and determine the direction of cerebrospinal fluid flow. During an angiography, a contrast agent is injected into the arteries that supply blood to the brain. After some time, anomalies at the level of blood vessels and pathological processes are detected. Doctors at the Yusupov Hospital use innovative methods for diagnosing cerebral vascular diseases - magnetic resonance angiography, which does not require the administration of contrast agents. A neuropsychological examination involves conducting a survey to identify abnormalities in the functioning of the brain.
Treatment of hydrocephalus
Neurologists at the Yusupov Hospital take a differentiated approach to treating patients with hydrocephalus. In case of a regressed form of the disease, drug therapy is not used. To reduce cerebrospinal fluid pressure, patients are prescribed diuretics: Diacarb, mannitol, Lasix. Nootropics, venotonics and angioprotectors improve the functional activity of the brain.
For progressive hydrocephalus, neurosurgeons at partner clinics of the Yusupov Hospital perform shunt operations. If there is an obstacle to the outflow of cerebrospinal fluid, the space-occupying lesion is removed or the adhesions are cut. If a hematoma is present, it is removed surgically.
An innovative method of treating hydrocephalus is endoscopic surgery:
- endoscopic ventriculocisternostomy of the bottom of the third ventricle;
- endoscopic installation of a shunt system;
- septostomy;
- aqueductoplasty;
- ventriculocystocysternostomy;
- endoscopic removal of intraventricular brain tumor.
Endoscopic operations have a number of advantages compared to bypass interventions: they restore the physiological flow of cerebrospinal fluid, are less traumatic, and improve the patient’s quality of life.
Treatment with endoscopic methods
Endoscopic treatment of hydrocephalus, or dropsy of the brain, is a priority in neurosurgery, since this disease is common among both children and adults. Hydrocephalus of the brain occurs due to impaired absorption of cerebrospinal fluid into the venous system.
Endoscopic surgery
Endoscopic interventions for hydrocephalus of the brain are used to reduce intracranial pressure. Surgeries for dropsy are most effective in comparison with drug therapies, which help slow the progression of the disease, but do not eliminate it. Endoscopic surgery for hydrocephalus, the cost of treatment of which is determined by the severity of the disease, is divided into several types:
- Septostomy;
- Ventriculocisternostomy of the floor of the third ventricle;
- Ventriculocisternostomy;
- Installation of the shunt system endoscopically;
- Removal of intraventricular tumors endoscopically;
- Aqueductoplasty.
The most widely used is endoscopic ventriculocisternostomy of the bottom of the third ventricle. The main task of the surgeon with this technique is to create pathways for the outflow of cerebrospinal fluid from the ventricles into the cisterns of the brain, through which the cerebrospinal fluid is absorbed into the vascular walls, as in a healthy person.
Advantages of endoscopic operations
Endoscopic surgery can only be effective if it is performed by a good specialist. One wrong move by the surgeon during brain surgery can lead to irreparable, severe consequences. When shunts are installed, they are often blocked by blood clots, tumor cells, etc. During endoscopy, no foreign objects remain in the body, and accordingly, the development of such complications is excluded.
In severe cases, patients are given brain drains. Such an event is very dangerous, since the infection can easily penetrate the brain through the drainage. With endoscopic intervention this complication does not occur.
Bypass surgery
Many people who have been diagnosed with the disease wonder where to treat hydrocephalus: in a public medical institution or a modern clinic. Yusupov Hospital is equipped with the latest equipment. Doctors regularly improve their skills and master new treatment methods. The clinic staff ensures a comfortable stay for patients.
Shunt surgery for hydrocephalus in adults, the price of which varies depending on the characteristics of the disease, is performed safely and efficiently at the Yusupov Hospital. Installation of a shunt system ensures the removal of cerebrospinal fluid. The procedure lasts about 90 minutes and is performed under general anesthesia for patients of any age.
Bypass surgery is a safe intervention, but there are certain risks when using it, which the neurologist informs the patient about. For example, a reaction to anesthesia or bleeding may develop. Shunt surgery allows the patient to restore normal brain function.
Surgery and hospitalization
Implantation of the shunt system is carried out by a neurosurgeon under sterile operating room conditions. In preparation for surgery, the hair is shaved to achieve maximum cleanliness. The operation is performed under general anesthesia, usually not for a very long time. The neurosurgeon drills a small hole in the skull bone, then makes a small incision in the dura mater that protects the brain and inserts a ventricular catheter into the lateral ventricle. To implant the rest of the bypass system, another incision is made and a tunnel is created subcutaneously to implant a peritoneal or cardiac catheter. The end of the catheter is carefully inserted either into the abdominal cavity or into the jugular vein leading to the ventricle of the heart. Catheters are connected to the valve using connectors on the valve itself. All parts of the shunt are thus connected into a single drainage system. At the end of the operation, small sterile dressings are applied to each incision.
Immediately after the operation, the patient is taken to the postoperative department. The patient is here from 1 hour to 1 day under close observation, then he is transferred to the ward. Most patients are discharged 7-10 days after clinical rehabilitation.