Intercostal neuralgia is a pain syndrome in the intercostal spaces caused by a pathological condition of the peripheral nerves. Due to the location and nature of the pain, it can be confused with a heart attack, and therefore often leads patients into a state of panic. Intercostal neuralgia occurs in approximately 10% of the adult population.
MedEx offers to make an appointment with a neurologist. If necessary, the clinic can carry out all necessary diagnostic procedures and laboratory tests.
Causes
The causes of intercostal neuralgia may be associated with inflammation of the peripheral nerves. As a rule, it develops as a result of hypothermia or an infectious process of another localization. For example, intercostal neuralgia often occurs as a result of herpetic infection or herpes zoster.
Intercostal neuralgia develops as a result of degenerative changes in the thoracic spine. Diseases that lead to the destruction and reduction of the height of the intervertebral discs provoke compression of the nerves. Bone growths form on the vertebrae, which also irritate the nerves.
Other possible reasons include:
- Physical overexertion. Staying in an uncomfortable position for a long time, sleeping on a hard or too soft mattress, intense exercise, as well as chronic vertebrogenic syndrome can lead to compression of the nerves.
- Injuries. Nerve damage can be caused by broken ribs, bruises, and injuries to the chest and spine.
- Cardiovascular diseases. A number of pathologies lead to hypoxia of the nerve trunks - atherosclerosis, arterial hypertension, rheumatism and anemia.
- Endocrine disorders. Intercostal neuralgia is often diagnosed in women during menopause, patients with thyrotoxicosis, diseases of the adrenal glands, and also after long-term use of hormonal drugs.
This is not a complete list of diseases and pathological conditions that are accompanied by intercostal neuralgia. The risks of developing the syndrome increase with gastric and duodenal ulcers, diabetes mellitus, tumor diseases, gastritis and colitis.
Reasons for the development of neuralgia
The development of neuralgia in certain nerve fibers is due to their anatomical features. Thus, pathological lesions often develop in nerves that pass through narrow channels and openings.
Essential (primary) neuralgia develops for no apparent reason; clinical examination in this case does not reveal other diseases. It is believed that the cause of essential neuralgia may lie in the pressure that is exerted on the nerve fibers by the vascular arteriovenous connections.
Symptomatic (secondary) neuralgia is caused by systemic pathological processes, such as multiple sclerosis. In multiple sclerosis, the myelin sheath surrounding the nerve fiber is destroyed. The myelin sheath ensures the conduction of nerve impulses and protects the nerve fiber. Further destruction of the nerve fiber occurs. Neuralgia can also be caused by a growing tumor compressing the nerve fiber or a traumatic lesion.
Symptoms
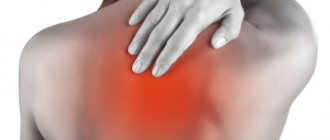
The main symptom of intercostal neuralgia is acute unilateral piercing pain localized in the chest. It is gradually growing. Pain with intercostal neuralgia spreads from the spine to the midline of the abdomen or sternum, becoming encircling in nature.
The pain will increase if:
- cough;
- laugh;
- sneeze;
- take a deep breath;
- start moving quickly.
If certain muscle groups are overstrained, the pain may intensify if you lean forward.
Palpation of the affected area with intercostal neuralgia in adults is painful, since the sensitivity of the nerve fibers is increased. There may be a burning sensation or numbness along the nerves.
Acute intercostal neuralgia is manifested by redness or blanching of the skin, hyperhidrosis due to damage to the sympathetic fibers of the peripheral nerves. Depending on which area is affected, the pain can spread to the right or left, affecting the area under the shoulder blades on the back.
Diagnosis of ganglionitis of the pterygopalatine ganglion
This disease is not easy to diagnose due to its similar clinical picture to other pathologies. For example, similar symptoms are observed in nasociliary nerve syndrome, Sicard syndrome, Charlin syndrome, migraine and temporal arteritis.
It is important to distinguish ganglionitis of the pterygopalatine ganglion from various types of facial neuralgia, in which shooting pain is also observed, but is not accompanied by nausea or vomiting. Changes in the mucous membrane of the paranasal sinuses are very similar to the clinical picture of rhinitis and sinusitis. To exclude these diseases, turundas soaked in a weak solution of cocaine, dicaine or novocaine are introduced into the nasal passages. A change in the nature of pain, its reduction, and partial normalization of autonomic functions can confirm the diagnosis of ganglionitis of the pterygopalatine ganglion.
The difficulty of diagnosing this disease is explained primarily by the fact that the pterygopalatine ganglion is associated with many nerve structures, which, when inflamed or excited, can give a wide variety of symptoms. When diagnosing this disease, the patient needs to consult several doctors, in addition to a neurologist - an otolaryngologist and a dentist.
Expert opinion of a doctor
Intercostal neuralgia on the left side of the heart is often mistaken by patients for a heart attack. It can be distinguished by its characteristic features. If you take a stationary position during intercostal neuralgia, the symptoms will become less pronounced. For cardiovascular diseases - no.
Pain with intercostal neuralgia intensifies due to coughing, laughter, deep breaths, and forced movements. However, it does not change during cardio exercise. With cardiovascular diseases, it's exactly the opposite.
With neuralgia, heart rate and blood pressure do not change, the pain is girdling in nature and intensifies with palpation of the ribs. In cardiovascular diseases, blood pressure and heart rate change, palpation is painless, and the pain syndrome is localized in the projection of the heart or behind the sternum.
Symptoms of occipital neuralgia
Primarily, neuralgia of the greater occipital nerve is characterized by headache. Her character is very specific:
- pain is concentrated behind the ears, in the occipital region, lower part of the neck, as well as in the eye area or above them;
- attacks occur unexpectedly when turning the head or touching the area of innervation, often when touching the skin of the head;
- painful sensations are localized on one side, although bilateral damage occasionally occurs;
- the pain looks like “lumbago” and disappears as suddenly as it begins;
- bright light causes pain in the eyes.
Diagnostics
Diagnosis of intercostal neuralgia begins with an initial examination. First of all, the doctor pays attention to the position of the patient’s body. As a rule, it is tilted to the opposite side - so as not to provoke a second attack. If several nerve branches are affected, sensitivity in a certain area may be impaired.
To clarify the diagnosis, additional studies and procedures may be required:
- ECG;
- X-rays of light;
- MRI of the spine;
- Ultrasound of the abdominal organs;
- electroneurography.
Additional research is needed to differentiate intercostal neuralgia from cardiovascular diseases, infections, diseases of the musculoskeletal system and digestive tract. In this regard, you may need additional consultation with a specialized specialist - a cardiologist, gastroenterologist, chiropractor.
Research is also carried out to clarify the nature and location of the disease. Thus, electroneurography helps determine the structure and functionality of nerve fibers and determine the causes of their irritation.
Important! The information is posted on the website for informational purposes. Don't self-diagnose - consult a specialist!
Causes of ganglionitis of the pterygopalatine ganglion
The pterygopalatine node can be affected due to inflammatory processes in the sinuses of the upper or lower jaw (osteomyelitis), the ethmoid labyrinth of the paranasal sinuses. The causes of this disease can also be toxic effects from tonsillitis, local damage (for example, foreign damage to the nose or its mucous membrane), the harmful effects of caries, and purulent otitis.
Any infectious foci in the oral cavity can become serious provocateurs of this disease. Provocateurs for the excitation of the disease are overwork or lack of sleep, loud annoying sounds of a constant nature, stress, alcohol abuse or smoking.
Inflammation of the pterygopalatine node can also be caused by maxillary tumors, both benign and malignant.
Treatment
Treatment is selected taking into account the root cause of the pathological process, as well as the current condition of the patient.
To relieve acute pain during an attack of intercostal neuralgia, painkillers are used. If the pain is very severe, they give injections - injections with solutions of lidocaine and novocaine.
In the acute stage of the pathological process, the patient is prescribed bed rest and rest. Drugs and methods are selected aimed at normalizing the functioning of the nervous and muscular systems:
- B vitamins;
- analgesics;
- muscle relaxants;
- sedatives;
- NSAIDs.
If there is severe swelling of the tissues, diuretics are prescribed to the patient.
If the pathological process is caused by a herpes infection, antiviral and antihistamines are prescribed. If it is not possible to check for infection, they are prescribed for preventive purposes.
The rehabilitation period can last several weeks or even months. How long it lasts depends on the patient's condition. The doctor selects a set of measures aimed at restoring the nervous system:
- exercise therapy;
- massotherapy;
- osteopathy;
- drug therapy.
In the period between exacerbations, mud therapy, as well as radon, sodium chloride, and sulfide baths can be used. Manual therapy, kinesiotaping and acupuncture are used to relax the fascia of the chest and back, improve the functioning of nerve fibers and overall well-being.
How exactly to treat intercostal neuralgia is determined by a neurologist. Self-medication for this disease is unacceptable.
Treatment of ganglionitis of the pterygopalatine ganglion
- The first task of a neurologist in treating this disease will be to eliminate the inflammatory process in the nose, its paranasal sinuses, the oral cavity, and teeth. For this purpose, anti-inflammatory, ganglion blocking agents are used. This is 1 ml of a 2.5% benzohexonium solution intramuscularly, 5% pentamine. Injections are given three times a day for a month.
- After pain syndromes are eliminated, medications are prescribed to generally strengthen the patient’s body, for example, vitamins B1, B6, B12, aloe, vitreous (immunotherapy). Sedatives are also required.
- To relieve severe pain, if conservative therapy is ineffective, the anesthetics trimecaine or lycocaine are used. In this case, the injection is made directly into the palatine canal. If parasympathetic symptoms are observed in the clinical picture, platifilin and spasmolitin are prescribed. In some cases, the use of glucocorticoids or hydrocortisone phonophoresis is prescribed (physiotherapeutic treatment options).
- If the disease develops as a result of inflammatory processes, then anti-infective therapy is used in the form of antibiotics or sulfonamides. The background of treatment is desensitizing drugs (diphenhydramine, pipolfen).
- To improve the patient’s general well-being, vasodilating antisclerotic drugs are prescribed, and injections are given to improve cerebral and general circulation.
- In severe cases of the disease, radical treatment is used in the form of direct destruction of the pterygopalatine node.
This can be done in one of two ways:
- Puncture of the pterygopalatine canal from the oral cavity. This method is difficult to perform and can have serious consequences for the patient;
- Puncture of the pterygopalatine node in the pterygopalatine fossa with access from under the zygomatic arch. With this method, a solution of phenol in glycerin and a concentrated alcohol solution (96%) are injected into the pterygopalatine node.
Relapses of the disease do not always disappear as a result of treatment, but the clinical picture changes significantly. Many symptoms disappear or appear much less frequently. Treatment must be comprehensive, adequate and timely, only in this case a positive result is possible.
Prevention
Prevention is a simple and affordable way to reduce the risk of intercostal neuralgia in adulthood. It includes moderate physical activity, selected in accordance with the general well-being of the patients. Loads should be dosed and regular, preferably daily.
It is important to monitor your posture. If you are predisposed to disorders, perform a set of exercises aimed at strengthening the muscle corset. To maintain immunity, you should avoid excessive stress and stress, eat well, and avoid hypothermia.
Treatment of occipital neuralgia
Sympathetic blockade
- Cost: 8,200 rub.
- Duration: 15-30 minutes
- Hospitalization: 2 hours in hospital
More details
At the CELT Pain Clinic, medical and surgical treatment methods are used to treat occipital neuralgia:
Drug treatment
Drug treatment methods are aimed at reducing pain. For this purpose, anticonvulsants and muscle relaxants are prescribed. In addition, massage and rest are prescribed.
A procedure called nerve block has proven itself well in our Pain Clinic. It consists of injecting the drug directly into the affected area, thereby achieving a long-lasting pain relief effect.
Surgery
If pain lasts a long time, is pronounced, or if conservative treatment does not bring the desired result, our specialists will recommend the following:
- pulsed radiofrequency ablation of the occipital nerves;
- stimulation of the occipital nerves - involves conducting electrical impulses through the nerves that block pain;
- microvascular decompression - involves the use of microsurgical techniques that eliminate compression of the nerves, and therefore the pain itself.
It is worth noting that occipital nerve stimulation is a minimally invasive method that does not have similar effects and is absolutely painless.
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions
Neuropathic pain: causes and symptoms
Contents Causes of occurrence
Component or disease
Stages of pain
Nerve restoration after damage
Neuropathic pain is a companion to many diseases. The cause of its appearance may be damage to various parts of the nervous system.
Such damage affects very different levels: from small nerves located deep in the tissues, to nerve trunks, plexuses, and even individual sections of the spinal cord and brain. Since a person is riddled with nerves, damage to them at any level and site can lead to neuropathic pain.
If you've ever bumped your elbow or had a dentist hit a nerve with a drill while working on your teeth, you understand what neuropathic pain is. People with chronic neuropathic pain experience this feeling on a daily basis. At the first manifestations, patients describe this pain as discomfort, burning, “shooting”.
Causes
Neuropathic pain can be caused by a variety of factors, including fractures, metabolic disorders, and nerve damage during surgery. It can also be caused by a stroke, limb amputation, or spinal cord injury.
Neuropathic pain results from disruption of nerve structure and function. And it’s worth mentioning separately about nerve compression, for example, when a benign neoplasm puts pressure on the walls of nearby organs and brings pain due to overstretching of these walls.
Neuropathic pain: stages of development and diagnosis How to determine the cause of neuropathic pain and in what cases it can be treated
Component or disease
Neuropathic can occur as an independent disease or accompany other diseases, for example, diabetes mellitus or coronary heart disease - then doctors talk about the neuropathic component.
Several types of pain can occur simultaneously. For example, neuropathic and nociceptiveXnociceptiveNociceptive pain is a medical term used to describe pain from physical injury. For example, this is pain from an injury or during a dental procedure. Most often, people experience nociceptive pain. It goes away when the affected part of the body recovers. * together.
If a person breaks his arm, events can develop according to different scenarios. The first case, when a fracture occurs and a sprain of muscles and ligaments occurs nearby, the person feels only typical nociceptive pain, which he describes as sharp, aching and throbbing. Another case is when, during a fracture, the nerve bundle is stretched or the nerve is torn.
Even when the bone heals and the person has no external reasons to worry, he may experience pain from this damaged nerve. If the area of damage was large, it is likely that the nerve will remain damaged forever and the person will deal with chronic neuropathic pain.
Pain terminologyWe explain the main terms and definitions in the topic of pain syndrome
Stages of pain
With damage to the nervous system, pain develops quite slowly and gradually. Typical situation –
the appearance of tunnel syndrome: nerves are compressed in narrow places by tendons, muscles or other structures located nearby. This can happen on the neck, arms, legs due to awkward posture, tight shoes or clothing. Carpal tunnel syndrome often occurs in office workers who work in one position at a computer.
Pain relief by ambulance What to do if the ambulance refuses to go to a person with breakthrough pain
Editorial Board
Anesthesia
Another situation is nerve irritation due to a herniated intervertebral disc, which is usually accompanied by aseptic inflammation and edema. At this stage, the nerve is only irritated or slightly compressed, but these effects do not go unnoticed and can cause severe pain and discomfort.
the second stage occurs . The nerve is compressed so that it ceases to perform its functions. Numbness appears in the area of innervation of the compressed nerve, and the person’s surface sensitivity is impaired.
The third stage is loss of deep sensitivity. Muscle weakness appears; muscles innervated by damaged nerves refuse to work. As a result, muscle atrophy occurs.
You may have heard the phrase “the leg is withered” or “the arm is withered” - this, in fact, is muscle atrophy.
When a doctor observes a deficiency of nerve function in a patient, he understands that emergency release of this nerve is necessary - decompression. The longer a person goes without treatment, the less chance there is of restoring nerve function after decompression. And even if the doctor performs an excellent technical intervention, a person who has endured this pain for a long time may remain with it for life if the nerve is not restored.
“There is no need to endure pain” Branch manager of the First Moscow Hospice named after V.V.
Millionshchikova Arif Ibragimov about what patients should know about pain, painkillers and a pain diary Arif Ibragimov
Anesthesia
Nerve restoration after damage
The nervous system is a very delicate, delicate and complex structure. Its imbalance is quite easy to cause, and self-healing of this structure occurs slowly, if at all. The regenerative capacity of the nervous system is severely limited, and any damage to the nerves is difficult to treat.
Most often, doctors are faced with a situation where a complete cure is impossible, and we are talking only about controlling symptoms, in fact, adapting to neuropathic pain. In this case, the task is to ensure an acceptable quality of life for the person and relieve pain as much as possible so that the person can sleep, communicate, and lead a social life.
Damage to a nerve usually leads to its restructuring. Secondary changes occur around the site of damage itself, and then further and further affect the overlying parts of the nervous system. If this pain in the immediate focus of damage is not dealt with in the early period, then there is a very high risk that the changes will go higher and lead first to peripheral sensitization (a pathological process in the nervous tissue) and then to central sensitization with the formation of a certain level of excitation in the central sensory neurons . Because of this, weak painful and non-painful stimuli begin to be perceived by the brain as severe pain.
If the source of damage affects the structures of the brain, in fact, an autonomous, separate disease develops.
Patients are forced to take medications throughout their lives that affect the regulation of neurotransmitters in the brain. Patients with chronic neuropathic pain may lose 1 cm³ of cerebral cortex per year.
With neuropathic pain, there is a rapid growth of the lesion, and therefore, when the first symptoms appear, you need to consult a doctor, otherwise it is quite difficult to treat it later.
How to treat neuropathic pain Read the article by algologist Alexey Voloshin about the four main methods of treating neuropathic pain, as well as what targeted therapy and neuromodulation are
You might be interested in:
Chronic pain: causes and manifestations
Many people, including some doctors, think that chronic and acute pain differ only in duration: acute pain is a short-term condition, chronic pain is one that does not go away for a long time. Chronic and acute pain are similar in appearance, but they have different principles of origin. Algologist Andrei Danilov explains why chronic pain is difficult to treat.
Simple Ways to Reduce Chronic Pain
Algologist Andrey Danilov on how sleep, positive emotions and meditation affect the perception of pain.
Pain Relief Guide
Answers to the most common questions that arise from patients and their loved ones when prescribing strong analgesics
“Pain is determined by how the nervous system perceives damage.”
Neurologist Maxim Churyukanov on the biopsychosocial model of pain, features of pain scales and shortcomings of the medical education system
Pain and dementia
Why is it important to learn to recognize pain and not ignore it?
Reprinting material on the Internet is possible only if there is an active hyperlink to the original material on the website
Survey
Diagnosis of neuralgia is the competence of a neurologist or therapist.
Neuralgia is not confirmed using laboratory or instrumental research methods. In most cases, characteristic attacks allow a diagnosis to be made. To exclude other diseases and confirm inflammation, the doctor may prescribe:
- ECG, chest X-ray, ultrasound of internal organs - if intercostal nerves, solar plexus are affected;
- general, biochemical blood tests - detect inflammation;
- ENMG (electroneuromyography) - shows the extent of nerve involvement in the process, as well as whether there are disturbances in the conduction of impulses to the muscles.
Osteochondrosis of the chest. Intercostal neuralgia
Osteochondrosis is a degenerative-dystrophic disease of the cartilage tissue of the human body, affecting the most mobile joints. Most often, the cervical and lumbar spine suffer from the disease. treatment of osteochondrosis of the thoracic region is noted by statistics much less frequently, but due to the anatomical specificity of the structure of this segment, in most cases the disease is diagnosed quite late and requires more time and effort to cure the patient.
Features of the structure of the thoracic spine
The thoracic segment of the spine contains 12 vertebrae connected to the ribs and sternum, forming a rather rigid structure designed to protect the internal organs (lungs, heart, liver, digestive system, etc.). Functionally, the chest is inactive, especially when compared with the cervical spine, and does not experience such significant mechanical stress as the lower back. Therefore, the symptoms of osteochondrosis in this area in the early stages of the disease do not cause much discomfort, and therefore practically do not alarm patients with their severity.
Pathology is usually discovered unexpectedly for the patient, during an x-ray or when serious pain has become a signal of the development of complications such as: protrusion or herniation of intervertebral discs, spinal canal stenosis, displacement of vertebral bodies, etc. Provocateurs of damage to the thoracic spine can be youthful postural disorders, such as scoliosis or Scheuermann-Mau kyphosis.
Symptoms of osteochondrosis of the thoracic region
Symptomatic manifestations of the disease can be different and are directly related to the location of the lesion. First of all, these are pain sensations of a chronic, aching nature, especially after prolonged physical exertion, and acute pain with sudden movements (turning, bending, lifting weights, sometimes even when sneezing or coughing). Stiffness and spasms of muscles, limited movements become the body's response to pain.
When the upper vertebrae of the thoracic region are affected, the pain is localized in the shoulder girdle, and tingling occurs between the shoulder blades or in the sternum. Damage to the middle areas usually manifests itself as pain in the heart area (which has nothing to do with diseases of the cardiovascular system) and intercostal space or girdle pain just below the heart (resembling hepatic colic). The appearance of osteochondrosis in the lower part of the chest affects the functioning of internal organs and can radiate pain to the abdominal cavity or lower abdomen.
Spasms of muscle structures and circulatory disorders in the affected area provoke a lack of supply of cartilage tissue with water and nutrients. Gradually, the intervertebral discs dry out, lose mobility and elasticity, and over time, their walls (fibrous rings) crack and the gelatinous substance (nucleus) filling them protrudes outward, forming an intervertebral hernia, the treatment of which requires a more serious approach, and in some cases, surgical intervention .
Depending on the location of the formation of herniated discs, they can cause compression of nerve endings and the manifestation of neurological symptoms, such as decreased sensitivity in the upper girdle of the extremities, slowing down of reflex reactions, radiating pain from the shoulder to the hand, etc. Protrusion of the herniated formation into the spinal canal causes compression of the spinal brain and leads to partial or complete immobility (paresis, paralysis) of the upper half of the body and/or disruption of the functioning of internal organs.
Compression of blood veins or arteries often provokes headaches, surges in blood pressure, interruptions in the blood supply to the brain and other vascular pathologies. Quite often, osteochondrosis is accompanied by treatment for intercostal neuralgia or thoracalgia (these are severe pain caused by compression or irritation of the intercostal nerves).
intercostal neuralgia (thoracalgia)
Thoracalgia is one of the most powerful pain syndromes of an acute, piercing, aching, burning, paroxysmal or periodic nature, with difficulty and limitation of respiratory capabilities. It may be accompanied by increased sweating, pulsation or spasms of muscle tissue, decreased sensitivity, paleness or, conversely, redness of the skin. When palpating the spine in the thoracic area along the intercostal spaces, the patient feels a dull pain.
Tissue numbness is observed directly at the site of compression or nerve damage. The feeling of pain with neuralgia can be felt not only in the heart area, but can be felt under the collarbone, in the lower back, under the shoulder blades. In this case, a neurologist or chiropractor must clearly differentiate clinical symptoms to exclude heart pathologies or peptic ulcers.
The main signs for diagnosing thoracalgia:
- The pain syndrome does not go away for a long time (does not weaken either day or night). With angina, the pain subsides 15-20 minutes after taking nitroglycerin.
- The pain syndrome intensifies with changes in the position of the body, sudden movements, deep inhalations and exhalations, coughing, sneezing, and slight squeezing of the chest or pressing on it. Heart attacks do not give such a reaction to movements of the body in space, but may be accompanied by arrhythmia or surges in blood pressure.
- Pain caused by stomach colic is quickly relieved with antispasmodic drugs, but for neuralgia, such drugs will have no effect.
- The reasons for this condition of the patient are pinching of the nerve roots of the intercostal system at the point of their exit from the spinal column by intervertebral discs damaged or flattened by osteochondrosis, herniated formations, overgrown osteophytes (bone formations on the vertebrae), tumors or injuries of the chest.
- Thoracalgia, as a rule, affects older people, when all the reasons for the progression of the disease intensify against the background of age-related changes (slowdown of metabolic processes, inactivity, accelerated leaching of calcium and other trace elements from the body, changes in the cardiovascular system, etc.). In children and adolescents, intercostal neuralgia is practically not observed.
Treatment of the disease
It should be noted that with both thoracic osteochondrosis and intercostal neuralgia, it is necessary to treat osteochondrosis, since neuralgia is only a pain symptom caused by degenerative-dystrophic changes in cartilaginous tissues. As practice has shown, traditional conservative treatment of the spine still remains quite effective.
During the acute period of the disease, the patient is prescribed complete rest, a maximum reduction in physical activity in combination with medications. Medicines used for neuralgia:
- analgesics - orally, intramuscularly, locally (in the form of novocaine or lidocaine blockades);
- non-steroidal anti-inflammatory substances - to relieve inflammation and swelling of soft tissues;
- muscle relaxants - to eliminate muscle spasms and release nerve roots;
- complexes of microelements and B vitamins - for general strengthening of the body and calming the patient’s nervous system.
When the pain syndrome subsides, you can begin the main therapy. It will consist of physiotherapeutic procedures, special dosed physical activity, exercise therapy, massages, attending manual therapy sessions, and diet.
An important role in the treatment of osteochondrosis of the thoracic spine is played by the patient’s attitude, his desire to recover and return to normal life.
It requires a rethinking of some life habits, awareness of giving up bad habits, increased physical activity, good nutrition, morning exercises, constant monitoring by the attending physician and an annual sanatorium-resort vacation. Author: K.M.N., Academician of the Russian Academy of Medical Sciences M.A. Bobyr