A fracture of the base of the skull is one of the most severe traumatic brain injuries. This condition is accompanied by damage to one or even several bones that form the base of the skull. Damaged in this case may be:
- occipital bone;
- temporal bone;
- ethmoid bone;
- sphenoid bone.
A fracture of the base of the skull can occur from a variety of serious physical injuries: car accidents;
- when a person falls from a great height;
- when hitting the face in the area of the lower jaw or base of the nose.
In most patients, the base fracture occurs from the arch. Statistics say that the number of such patients reaches 59%.
Causes of skull fracture
All causes of skull fracture are inherently mechanical injuries. In such cases, injury to the bone tissue of the head may occur:
- Falling from a great height or high speed;
- Hit your head hard with a heavy object;
- As a result of a traffic accident (car accident).
All these situations can arise as a result of non-compliance with safety rules on the road and at work, as a result of street fights and aggressive sports in sports clubs, or extreme sports.
When assessing age and social categories, groups at increased risk of skull fracture include children, active teenagers and middle-aged people, as well as people dependent on drugs and alcohol.
Pathogenesis of injury
The mechanism of action on the bones of the skull can be either direct or indirect.
If the bone breaks at the point where the blow occurred, the fracture is called a direct fracture. If the force of the shock wave was transferred from other bones through inertia, we are talking about an indirect mechanism of injury.
A calvarial fracture is usually the result of a direct blow. Bones bend under force.
Fractures of the base of the skull are often indirect. The injury occurs from the impact of a shock wave, which is formed when falling from a great height onto the legs or pelvis and is transmitted through the bones of the spine.
Skull fracture: classification of types
Classification of cranial bone injuries is made according to several criteria. Thus, depending on the appearance and physical condition of the victim’s head, injuries can be divided into open and closed fractures. An open fracture is a condition in which the scalp is damaged. A closed fracture is an injury in which the soft tissue remains intact.
The basic classification of injuries is based on the location of the injury:
- Fracture of bone tissue at the base of the skull;
- Broken bones at the base of the skull.
It is also possible to fracture the vault and base of the skull at the same time.
Depending on the nature of the resulting injuries, damage to the bone tissue of the head can be:
- Interferes. This type of injury is extremely dangerous because with a deep fracture, a cavity is formed in the skull from fragments of broken bone. If ingested, sharp fragments of the skull can damage the meninges, the brain, its arteries and cause a leak of cerebrospinal fluid. More often, such injury is accompanied by intense bleeding in the brain.
- Perforated. The main cause of injury was a gunshot wound to the head. The result of such an injury is almost always the immediate death of the victim.
- Shards. It is most often caused by being hit in the head with a heavy, sharp object or falling onto a protruding piece or hard object. In this case, the bones of the skull split, forming sharp fragments. Skull fragments damage the meninges and blood vessels. In most cases, such injuries end in death even before first aid is provided to the victim.
- Linear. With this type of injury, there is no critical displacement of bone tissue and fragments. The main injury of a broken bone is a shallow fracture. In the case of a linear skull fracture, the damaged portion of the bone may heal on its own over time.
Skull fracture.
Of all types of traumatic brain injury, a linear fracture is the least dangerous. This type of injury is most often diagnosed in children.
Fractures of the base of the skull
This type of injury is extremely dangerous because the integrity of the major components of the skull that protect the brain is compromised. In this case, the main parts of the brain, nerve bundles and the brain stem are damaged. A fracture of the base of the skull can cause an acute inflammatory process in the brain.
Bone fractures are accompanied by a rupture of the protective membrane of the brain and create a high risk of infection. Fractures due to trauma spread from the base of the skull to the bones of the orbit and nose. If the skull is damaged in the middle fossa, the fracture will extend to the ear.
Cranial vault fractures
The cranial vault is the line connecting the bones of the head. In different places the intersection may be as follows: the skull is not only jagged or folded, but also flat. On the sides of the cranial vault there are temporal protrusions that smoothly turn into depressions. In front there is a pronounced protrusion, which represents the frontal bone. On the back there are two parietal tubers and an occipital bulb. Between these areas of the cranial vault is a temple.
When the cranial arch is fractured, the internal bone plate is destroyed. Damages the dura mater when pressed. If a fracture occurs when the damaged bone reaches the vessels of the dura mater, these vessels rupture and bleed. With a closed fracture, hematomas do not have clear boundaries.
Peculiarities
In addition to a fracture in a specific area, adjacent sections are often injured - the temporal, sphenoid and occipital. The formation of cracks in different areas inevitably leads to the displacement of fragments, which in turn penetrate into the body of the brain, limiting its functionality (consequences - mental disorders, loss of connection with the speech apparatus, poor coordination of movements, and others).
Bleeding through the organs of smell, hearing and oral cavity cannot be ruled out. The lack of immediate qualified assistance leads to the addition of an inflammatory infection from the environment, thereby causing new pathologies. When arterial or venous vessels are torn, bruises form under the eyes, the eyes fill with blood, and the skin turns pale.
When the bones of the head are fractured, air sometimes penetrates under the skin, forming peculiar plaques and swellings - these formations are called emphysema. If a patient has at least a few emphysemas, it means he has exactly the type of injury in question. Other consequences after such damage: memory loss, change in character type, clouding of reason, personality disorders.
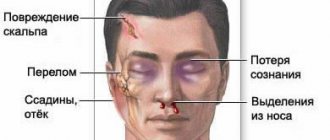
Skull fracture: clinical manifestations
The symptoms of the pathology depend on the nature of the existing injuries. However, there are also common symptoms that indicate a skull fracture. These include:
- Sudden, short-term, partial or complete loss of sensation in certain areas of the head or body;
- Loss of consciousness;
- Coma;
- Paresis;
- Arrhythmia;
- A state of increased excitement or complete immobility;
- Paralysis;
- Involuntary urination;
- Prolonged tension headache; Nausea; Vomit;
- Nausea and vomiting;
- Rhythm disturbance and respiratory arrest;
- Students react sluggishly to external stimuli;
- The circulatory system is disrupted.
Loss of consciousness is one of the possible symptoms of a skull fracture.
Often after a skull fracture, there is periodic loss of balance, as well as confusion in space. The more clearly the symptoms of the pathology appear, the more severe the injury and the more extensive the brain damage.
Symptoms of a basal skull fracture
Depending on the location of the injury, the victim may experience different symptoms of a basal skull fracture. Trauma to the anterior fossa of the skull often causes:
- Intense and prolonged nosebleeds;
- Sometimes there is a leak of cerebrospinal fluid through the nostrils;
- After two or more days, bruises and bruises appear around the eyes and on the whites of the eyes.
- With parallel damage to the hyoid bone, emphysema develops at the site of injury.
With a fracture of the base of the skull in the area of the medial fossa, pathological processes are often observed, such as:
- Bleeding from the ear;
- Disturbances in the functioning of the facial nerves;
- The appearance of hematomas around or behind the ears;
- Intensive leakage of cerebrospinal fluid through the auricle;
- Loss of sensation of individual taste buds;
- Occasional difficulty maintaining balance.
Moreover, these types of injuries are often accompanied by partial or complete hearing loss.
Damage to the base of the skull from the posterior lobe is accompanied by the following unpleasant conditions:
- The appearance of hematomas around the auricle of one or both ears;
- Disturbances in the functioning of nerve endings.
Often such damage leads to the development of paralysis of the stamens. Accompanied by impaired articulation, speech pronunciation and problems with swallowing. In this case, the victim's voice becomes hoarse and nasal, and speech becomes slurred.
Signs of a calvarial fracture
The following symptoms are typical for a skull fracture:
- Bleeding from the patient's nose, ear, or mouth;
- Intermittent exudation of cerebrospinal fluid. The volume of leaked liquid can exceed 200 ml per day. In this case, intracranial pressure is significantly reduced. The pathological process lasts up to 6 days;
- The appearance of late bruises around the eyes and on the whites of the eyes. This symptom appears several days after the injury;
- Hearing impaired.
The occurrence of nosebleeds is one of the possible symptoms of a skull fracture.
Paresis and paralysis of the facial nerve can occur when the bony canal is damaged, ptosis and one or both eyes looking outward or downward can occur due to rupture of the oculomotor nerve.
A significant increase in bleeding occurs when the victim tries to turn his head. Therefore, turning your head with this type of fracture is strictly prohibited.
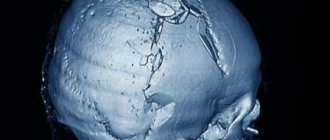
Structure of the base of the skull
It simply doesn’t make sense to analyze the structure of the base of the skull in detail; this detail is best left to doctors. The boundary between the base and the arch is a line passing through specific anatomical formations.
A photograph provides a visual representation of the structure of the base of the skull and its boundaries. Doctors classify such injuries based on location and cranial fossa. There are anterior, middle and posterior cranial fossae with many holes. Vessels and nerves penetrate the cranial cavity through them; the relief almost completely replicates the brain.
First aid
If you notice signs of a skull fracture, seek medical attention immediately. Before arriving, doctors do not want to give the victim anesthesia, since some medications can significantly increase bleeding or breathing problems, as well as provoke the patient into a coma.
Before the ambulance arrives, it is important to provide first aid:
- The patient should be placed on his back on a hard surface, with his head buried in the ground. The pillow should not be placed under the head. If the patient is unconscious, he should also be placed on his back, but in a half-turn position with a roll of clothing on one side. You need to tilt your head slightly so as not to choke when vomiting.
- Treat the head wound with an antiseptic and apply a sterile bandage.
- Remove the victim's dentures, jewelry, watches, and glasses.
- Remove any clothing that may be tight fitting, obstructing blood flow and breathing.
- Bring a cold object wrapped in a clean cloth to your head.
If the victim is not breathing, empty the vomit from the mouth and perform mouth-to-mouth resuscitation using chest compressions. To avoid direct contact with the victim's mucous membranes, use a piece of clean, permeable cloth.
If there are no breathing problems, it is permissible to give the injured person Analgin with diphenhydramine. When transporting a patient to a medical facility, the following activities are performed:
- Glucose, diuretics and cardiac drugs are administered intravenously. However, in case of severe bleeding, diuretics should not be used. Instead, Polyglucin or Getinol is administered. Lasix is most often used as a diuretic, and cordeamine and sulfacamphocaine are the main medications used to support heart muscle function.
- If breathing problems occur, the patient is inhaled through an oxygen mask.
- Convulsions and increased motor activity are suppressed by Suprastin.
Polyglucinum is prescribed for severe bleeding.
The use of narcotic anesthetics is unacceptable. Such drugs can cause respiratory arrest.
Surgical treatment of skull trauma
If conservative treatment methods do not have a positive effect on the process of cerebral fluid leakage, there is a risk of developing recurrent meningitis. In this case, surgical intervention is prescribed, during which the liquor fistulas are eliminated. To determine the exact location of the defect, an MRI is performed with the injection of a contrast agent into the cerebrospinal fluid.
During trepanation of the frontal region, the lumen is closed by suturing the dura mater; in difficult cases, plastic correction of the aponeurosis or fascia is used. The bone defect is corrected by applying a piece of muscle. When liquorrhea is caused by injury to the wall of the sphenoid sinus, tamponade is performed using a muscle or a hemostatic sponge during transnasal intervention.
Violation of the geometry of the skull bones can lead to damage to the optic canal. The nerve suffers from the pressure of the hematoma. The consequences are blurred vision or total blindness. In such conditions, decompression of the optic nerve is indicated; for this, the canal is opened through transcranial intervention.
Extensive comminuted fractures require surgical treatment with cranioplasty. First, the surgeon removes sharp bone fragments from the wound, and the defect in the calvarium is closed with a plate that is attached to the bone. Special fast-hardening plastic is widely used for prostheses. Tantalum plates are also used.
Urgent surgical intervention is required if an intracranial hematoma forms. The accumulated blood is removed and its source is eliminated.
Antibiotics cannot always stop the development of a purulent infection that has entered the skull after an injury. In this case, surgical treatment is also indicated.
The decision on any surgical intervention is made by a neurosurgeon, based on both the diagnosis and the general condition of the patient’s body, and his age.
Subsequently, the patient requires a long rehabilitation process.
Skull fracture: diagnostic methods
Diagnostics is carried out comprehensively and includes the following activities:
- Medical examination and collection of information about the patient’s ailments. During the examination, the doctor assesses the general condition of the victim, the reaction of the pupils, and measures the pulse and blood pressure. The position of the tongue and the symmetry of the patient's jaw are also assessed. Neurological reactions are studied;
- X-rays of the skull are taken in two projections;
- A computed tomography (CT) or magnetic resonance imaging (MRI) scan is performed.
In extremely severe cases, when it is impossible to make a complete diagnosis, treatment of the patient is prescribed based on the external symptoms of the pathology.
Treatment options
Patient treatment methods are selected depending on the type of injury. Therapy can be carried out either surgically or conservatively. For linear skull fractures, conservative methods are mainly used. They are also acceptable for use in mild to moderate injuries where the flow of cerebrospinal fluid can be stopped without surgery.
Conservative treatment includes:
- Strict adherence to the rules of bed rest.
- Perform lumbar punctures 2-3 times a day every day. At the same time, oxygen is introduced into the subarachnoid space of the spinal cord.
- Taking diuretics.
- Daily disinfection of the oral cavity, middle ear and nasopharynx to prevent the development of purulent inflammation.
Surgical intervention is necessary in the following cases:
- Shock fracture of the skull;
- Linear fracture of the skull bones with the formation of a large number of fragments;
- Bone damage that puts pressure on the brain and causes blood vessels and nerve endings to rupture;
- Recurrent purulent inflammation.
In case of a deep skull fracture, intervention is required. surgical
Treatment of linear fractures, as well as other types of fractures during surgery, is carried out by craniotomy. After removing all fragments and purulent formations, the skull bed, previously removed with bone or a special titanium plate, is closed. The most common type is a plate prosthesis.
Mechanisms of damage
Fractures of the bones of the base of the skull are in almost all cases accompanied by rupture of the dura mater of the brain. In this case, communication occurs between the oral cavity, nose, paranasal sinuses, middle ear and orbit with the air of the external environment. It can lead to the entry of microbial agents and infection of brain tissue, the appearance of post-traumatic pneumocephalus and the leakage of cerebrospinal fluid from the ears and nose (auricular and nasal liquorrhea).
With fractures of the anterior cranial fossa, hemorrhage occurs in the tissue of the periorbital tissue (“symptom of glasses” or “raccoon eyes”). When the perforated plate and cells of the ethmoid bone are broken, cerebrospinal fluid may leak through the nose and in some cases subcutaneous emphysema develops.
With some fractures of this part of the skull, damage to the optic, oculomotor and olfactory nerves can occur. Such injuries may be accompanied by concomitant injuries to the diencephalic parts of the brain.
Skull fracture: complications
There are always complications after a skull fracture. With a linear skull fracture, the negative consequences are minimal and may only include occasional nausea and headaches. This type of skull fracture is most common in infants and older children.
Complications after such a fracture in newborns most often appear in adulthood, but already in infancy the pathology can be accompanied by the accumulation of blood at the site of injury.
In general, a fracture of the vault and base of the skull can cause the following pathologies:
- Rapid deterioration of vision and hearing;
- Regular migraines in the head area;
- Frequent loss of consciousness;
- Breathing disorders;
- Jumps in blood pressure, up to hypertensive crisis;
- Loss of spatial orientation;
- Hyperactivity and nervousness;
- Epilepsy;
- Bleeding from the ear and nose.
Survival for fractures of the base of the skull and roof depends on the correctness and timeliness of medical care. For injuries of the cranial vault, in which there are no complications in the form of purulent formations and multiple fragments, the survival rate is more than 65%.
In victims with basal skull fractures, the survival rate is about 50% without significant complications. In contrast, in cases of trauma to the base of the skull with concomitant epileptic seizures and periodic nosebleeds, the chances of survival are 24-50%. However, the final result largely depends on the timeliness and adequacy of treatment.
Consequences
Any damage to the skull is associated with various consequences. Some of them appear almost immediately after the incident, while others will take some time to develop.
- the entry of bacteria into the cerebrospinal fluid can trigger the development of meningitis.
- air ingress can cause pneumoencephaly.
- Fractures sustained in childhood have a significant impact on mental, physical and psycho-emotional development.
- a fracture of the skull, especially its base, can lead to complete paralysis of the body, since it is the base of the skull that connects the spinal cord and brain.
User Rating: 5.00 / 5
Thank You for rating this article.
Rehabilitation
For any skull fracture in an adult or child, in addition to treatment, a long rehabilitation period is required. While the injury is healing and for at least 6 months afterwards, the patient should not undertake any physical activity.
During the recovery period, the patient is advised to periodically use the Chantz collar. It is also possible to participate in sessions of magnetic and acupuncture therapy, massage and electrophoresis. The patient is recommended to attend classes with a psychologist and psychiatrist, and in some cases, classes with a speech therapist are necessary.
Consequences of bone destructive lesions of the skull
Not all bone-destructive complications of traumatic brain injuries are observed in short periods of time. The nature of complications is determined by swelling, purulent lesions, and the severity of accompanying symptoms.
According to the time of occurrence, the consequences are divided into distant and nearby.
Quick symptoms of skull injuries:
- Damage to the membranes of the brain with the development of encephalitis and meningitis;
- Formation of hematomas (epidural, subdural);
- Development of abscesses;
- Hemorrhages.
Short-term effects require emergency medical attention. Without drug treatment, the likelihood of death is high.
Long-term complications develop over time. Some consequences occur after five years or more:
- Defects of mental activity;
- Increased intracranial pressure with strokes;
- Paralysis, paresis of limbs;
- Epileptic convulsions;
- Mental retardation, encephalopathy.
Most long-term complications develop due to inflammation, vascular and nerve ischemia.
Hematomas - consequences of TBI
The limited accumulation of blood causes an increase in intracranial pressure. The brain is covered by three membranes. A subdural hematoma of a chronic, subacute or acute type is formed on top of the external fascia.
In the first type, symptoms are observed several months after the TBI.
Subdural hematoma
A subacute hematoma forms within a few hours. Delayed development causes clinical symptoms and signs that require medical intervention.
Acute hematoma is life threatening. It forms quickly a few minutes after a cranial injury and can accompany fractures of the base and pyramid of the temporal bone. The risk of exacerbation increases in patients after taking anticoagulants, aspirin, and alcoholics.
Epidural hematoma
Extradural location develops after rupture of the vessel. Localization of the formation is between the main bone fragments and the outer shell. The cause is a fracture with rupture of the vessel. The limited accumulation of blood leads to compression of the brain tissue.
In the absence of proper treatment, a hematoma leads to death. The nosology often occurs in adolescents after traffic accidents with a scooter or motorcycle.
Intracerebral hematoma
Excessive accumulation of blood inside the brain is accompanied by numerous complications. Traumatic injuries are caused by neurites, abscesses, meningitis, and microstrokes.
The main reasons for the formation of intracerebral hematoma:
- Sickle cell anemia;
- Hemophilia;
- Administration of drugs to dissolve blood clots;
- Brain neoplasms;
- Cerebral hypertension;
- Aneurysm, arteriovenous malformation;
- Autoimmune diseases with damage to the arterial membrane;
- Liver diseases.
Brain contusion is accompanied by focal symptoms. The blade is determined by the predominant localization of the formation:
- Paralysis of limbs;
- Numbness of the tongue;
- Loss of consciousness;
- Decreased hearing and vision;
- Intellectual impairment;
- Memory loss;
- Intellectual disorders;
- Strabismus;
- Twitching of eyeballs.
The appearance of the described signs after a head injury requires immediate diagnosis of the causes of the pathology.