Subarachnoid hemorrhage is a condition caused by cerebral bleeding, in which blood accumulates in the subarachnoid space of the cerebral membranes. It is characterized by intense and sharp headache, short-term loss of consciousness and confusion in combination with hyperthermia and meningeal symptom complex. Diagnosed by CT and cerebral angiography; if they are unavailable, by the presence of blood in the cerebrospinal fluid. The basis of treatment is basic therapy, relief of vasospasm and surgical exclusion of the cerebral aneurysm from the bloodstream.
ICD-10
I60 Subarachnoid hemorrhage
- Causes Risk factors
- Pre-hemorrhagic period
- Basic and specific therapy
General information
Subarachnoid hemorrhage (SAH) is a separate type of hemorrhagic stroke in which blood leaks into the subarachnoid (subarachnoid) space. The latter is located between the arachnoid (arachnoid) and soft cerebral membranes and contains cerebrospinal fluid. Blood poured into the subarachnoid space increases the volume of fluid contained in it, which leads to an increase in intracranial pressure. Irritation of the soft cerebral membrane occurs with the development of aseptic meningitis.
Vasospasm that occurs in response to bleeding can cause ischemia of certain areas of the brain with the occurrence of ischemic stroke or TIA. Subarachnoid hemorrhage accounts for about 10% of all strokes. Its frequency of occurrence per year varies from 6 to 20 cases per 100 thousand population. As a rule, SAH is diagnosed in people over 20 years of age, most often (up to 80% of cases) in the age range from 40 to 65 years.
Subarachnoid hemorrhage
Causes
Most often, subarachnoid bleeding is a complication of cerebrovascular diseases and head injuries.
- Rupture of a vascular aneurysm. It causes subarachnoid hemorrhage in 70-85% of cases. If you have a cerebral aneurysm, the chance of it rupturing ranges from 1% to 5% per year and from 10% to 30% throughout your life. Diseases often accompanied by the presence of a cerebral aneurysm include: Ehlers-Danlos syndrome, phakomatoses, Marfan syndrome, anomalies of the circle of Willis, coarctation of the aorta, congenital hemorrhagic telangiectasia, polycystic kidney disease and other congenital diseases. Cerebral AVMs usually lead to hemorrhage into the cerebral ventricles or parenchymal-subarachnoid hemorrhage and are rarely the etiological factor of isolated SAH.
- Head injuries. Subarachnoid hemorrhage of traumatic origin occurs during TBI and is caused by injury to blood vessels due to a skull fracture, brain contusion or compression. An example of such SAH is subarachnoid hemorrhage caused by birth trauma of the newborn. Risk factors for SAH in a newborn are a narrow pelvis in a woman in labor, rapid labor, post-term pregnancy, intrauterine infections, a large fetus, fetal developmental abnormalities, and prematurity.
- Pathology of ectracranial arteries. Subarachnoid hemorrhage can occur due to dissection of the vertebral or carotid artery. In the vast majority of cases, we are talking about dissection of the extracranial sections of the vertebral artery, spreading into its intradural section.
- Rare factors. In some cases, the cause of SAH is cardiac myxoma, cerebral tumor, vasculitis, angiopathy due to amyloidosis, sickle cell anemia, various coagulopathies, and anticoagulant treatment.
Risk factors
Along with the direct causes of SAH, contributing factors are identified: arterial hypertension, alcoholism, atherosclerosis and hypercholesterolemia, smoking. In 15-20% of SAH, the cause of hemorrhage cannot be determined. In such cases, they talk about the cryptogenic nature of SAH. Such variants include nonaneurysmal perimesencephalic benign subarachnoid hemorrhage, in which bleeding occurs in the cisterns surrounding the midbrain.
Neurology Center in Moscow
Hemorrhagic stroke. Kinds:
- Parenchymal hemorrhage
- Subarachnoid hemorrhage
- Parenchymal-subarachnoid hemorrhage
- Intraventricular hemorrhage
- Stroke hematomas - non-traumatic subdural and epidural hemorrhages
Parenchymal hemorrhage
Parenchymal hemorrhage is one of the forms of acute cerebrovascular accident of the hemorrhagic type. Manifested by the appearance of focal symptoms. This is paralysis in the leg and arm, speech disorder of the dysarthria type, and blindness may suddenly develop. The nature of the symptoms depends on the location and volume of the hemorrhage.
Usually the condition is accompanied by general cerebral symptoms - headache, nausea, vomiting, depression of consciousness. These phenomena persist for more than a day.
Clinical picture of cerebral hemorrhage
Brain dysfunctions of vascular origin occur. This is the result of rupture of pathologically altered arteries of the brain. This usually occurs against a background of high blood pressure, chronic arterial hypertension, or cerebral amyloid angiopathy.
The consequence of a ruptured vessel is hemorrhage into the cranial cavity. The blood that spills out damages the brain parenchyma, and the products of its breakdown also have a toxic effect on it. This leads to swelling of the brain, compression and displacement of structures within the brain.
Diagnosis of cerebral hemorrhage
Reliable diagnostic methods are computed tomography and magnetic tomography.
If neuroimaging is not available, the diagnosis becomes less reliable.
Then it is recommended to analyze the clinical picture, spinal puncture data, and echoencephaloscopy.
Treatment methods for parenchymal hemorrhage
Carrying out basic therapy. The goals of basic therapy are to maintain normal blood pressure and eliminate cerebral edema.
Hematoma with parenchymal hemorrhage
Foci of hemorrhage range from very small to large. A large hematoma can destroy almost the entire hemisphere. Sometimes the simultaneous development of two or more lesions is possible. At various distances from the main focus, pinpoint hemorrhages can be seen. Foci of hemorrhage can be of the hematoma type and the hemorrhagic impregnation type.
Hematoma
The hematoma has a spherical shape, its edges are uneven. In the area of the hematoma there is blood that resembles a gelatinous mass; there may also be clots there. A zone of hemorrhagic infiltration is localized along the edges of the hematoma. Its width is 3-5 millimeters. This zone is followed by the zone of cerebral edema.
Brain edema provokes an increase in intracranial pressure and a disorder of venous circulation. If the hemorrhage has the form of hemorrhagic impregnation, then it does not have clear boundaries.
Symptoms of hematoma with parenchymal hemorrhage
Physical or emotional stress is a cause of hemorrhage. Usually the disease begins acutely, in the first half of the day, there are no warning signs.
It is possible to develop a comatose state - loss of consciousness, no active movements, no reaction to external stimuli, and vital functions are disrupted. When examining the patient, hemiplegia is revealed; paralyzed muscles have low tone.
If you lift a paralyzed limb, it falls like a whip. On the side of paralysis, the foot is rotated outward. Deep reflexes are not evoked. The pupils narrow or dilate and do not respond to light. On the affected side, the nasolabial fold is smoothed out, and the corner of the mouth is lowered.
Breathing with wheezing, exhalation or inhalation may be difficult. There is a slowing or increased heart rate. Pneumonia is likely to develop within 2-3 days.
Bedsores may appear in the area of the heels, buttocks, and sacrum. Severe vegetative symptoms are observed with hemorrhages in the ventricles of the brain.
When the first signs of cerebral hemorrhage occur, urgent medical attention is needed. The therapeutic department of the Neurology Center will provide highly qualified assistance in the diagnosis and treatment of cerebral hemorrhage.
Sign up for the Neurology Center:
- by phone: +7 925 191 50 55
- fill out the form: APPLICATION FOR TREATMENT
- Get advice by email [email protected]
- Clinic address: Moscow, Nagornaya st., 17 to 6
+7 (495) 506 61 01 –
REQUEST TO THE CLINIC
Classification
In accordance with the etiofactor, subarachnoid hemorrhage is classified into post-traumatic and spontaneous. Traumatologists are often faced with the first option, and specialists in the field of neurology with the second. Depending on the area of hemorrhage, isolated and combined SAH are distinguished. The latter, in turn, is divided into subarachnoid-ventricular, subarachnoid-parenchymatous and subarachnoid-parenchymatous-ventricular.
In world medicine, the Fisher classification is widely used, based on the prevalence of SAH according to the results of CT scans of the brain. In accordance with it, they distinguish:
- class 1 - no blood
- class 2 - SAC less than 1 mm thick without clots
- class 3 - SAC more than 1 mm thick or with clots
- class 4 - predominantly parenchymal or ventricular hemorrhage.
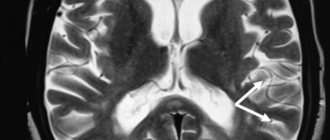
CT scan of the brain. Blood in the subarachnoid cerebrospinal fluid spaces on the right. (photo by V.N. Vishnyakov)
Symptoms of subarachnoid hemorrhage
Pre-hemorrhagic period
Precursors of SAH are observed in 10-15% of patients. They are caused by the presence of an aneurysm with thinned walls through which the liquid part of the blood leaks. The time of occurrence of precursors varies from a day to 2 weeks before SAH. Some authors distinguish it as the pre-hemorrhagic period. At this time, patients note transient cephalgia, dizziness, nausea, transient focal symptoms (damage to the trigeminal nerve, oculomotor disorders, paresis, visual impairment, aphasia, etc.). In the presence of a giant aneurysm, the clinic of the pre-hemorrhagic period has a tumor-like character in the form of progressive cerebral and focal symptoms.
Acute period
Subarachnoid hemorrhage manifests itself with acute, intense headache and disturbances of consciousness. With aneurysmal SAH, unusually strong, rapidly growing cephalalgia is observed. With arterial dissection, the headache is biphasic. Short-term loss of consciousness and confusion lasting up to 5-10 days are typical. Possible psychomotor agitation. Prolonged loss of consciousness and the development of severe disturbances (coma) indicate severe bleeding with bleeding into the cerebral ventricles.
The pathognomonic sign of SAH is the meningeal symptom complex: vomiting, neck stiffness, hyperesthesia, photophobia, meningeal symptoms of Kernig and Brudzinski. It appears and progresses on the first day of hemorrhage, can have varying severity and persist from several days to a month. The addition of focal neurological symptoms on the first day speaks in favor of combined parenchymal-subarachnoid hemorrhage. The later appearance of focal symptoms may be a consequence of secondary ischemic damage to brain tissue, which is observed in 25% of SAH.
Typically, subarachnoid hemorrhage occurs with a rise in temperature to febrility and viscero-vegetative disorders: bradycardia, arterial hypertension, and in severe cases, respiratory and cardiac dysfunction. Hyperthermia can be delayed and occurs as a consequence of the chemical action of blood breakdown products on the cerebral membranes and the thermoregulatory center. In 10% of cases epileptic seizures occur.
Atypical forms of SAH
In a third of patients, subarachnoid hemorrhage has an atypical course, masquerading as a paroxysm of migraine, acute psychosis, meningitis, hypertensive crisis, and cervical radiculitis.
- Migraine form. Occurs with the sudden onset of cephalgia without loss of consciousness. The meningeal symptom complex appears 3-7 days later as the patient’s condition worsens.
- False hypertensive form. Often regarded as a hypertensive crisis. Because cephalalgia manifests itself against the background of high blood pressure numbers. Subarachnoid hemorrhage is diagnosed during further examination of the patient if the condition worsens or rebleeds.
- The false inflammatory form imitates meningitis. Cephalgia, febrility, and severe meningeal symptoms are noted.
- The false psychotic form is characterized by a predominance of psychosymptomatics: disorientation, delirium, severe psychomotor agitation. It is observed when an aneurysm of the anterior cerebral artery, which supplies blood to the frontal lobes, ruptures.
Hemorrhagic stroke
Hemorrhagic stroke - hemorrhage in the brain and/or subarachnoid space, occurs four to five times less often than ischemic stroke
- Etiology of hemorrhagic stroke
The main etiological factors of hemorrhagic stroke are hypertension, arterial hypertension, congenital and acquired arterial and arteriovenous aneurysms. Subdural and epidural hematomas are usually of traumatic origin. Less commonly, the cause of hemorrhagic stroke can be hemorrhagic diathesis, the use of anticoagulants, amyloid angiopathies, mycoses, tumors, and encephalitis.
The predominant localization of hematomas is the cerebral hemispheres (about 90% of parenchymal hemorrhages); in 10% of cases, damage to the brain stem or cerebellum is detected. In most cases, there is a rupture of the vessel, much less often - diapedetic hemorrhages.
The clinic of parenchymal hemorrhages has general cerebral and focal symptoms. The clinical picture of subarachnoid hemorrhages includes two main groups of symptoms: cerebral and meningeal. In the presence of these and focal symptoms, we are talking about subarachnoid-parenchymal hemorrhage. Features of the clinical picture of parenchymal hemorrhages depend on the location of the hematoma.
- Hemorrhagic Stroke Clinic
Parenchymal hemorrhages. Hemorrhage into the putamen occurs with severe impairment of consciousness and a neurological defect in the form of contralateral hemiplegia, hemianesthesia, aphasia (with damage to the dominant hemisphere) or spatial hemiagnosia and anosognosia (with damage to the non-dominant hemisphere). The clinical picture is similar to that of middle cerebral artery occlusion.
With hemorrhages in the thalamus, as well as with hemorrhages in the putamen, herniation and coma are possible. Important signs of thalamic damage are greater severity of sensory disorders than motor ones, and unusual oculomotor disorders, often in the form of limited gaze, strabismus.
Table 1. HUNT Scale (Henry JM Barnett, Stroke, 1986) | |
| Degree | Characteristic |
| 0 | Unruptured aneurysm |
| I | Asymptomatic or minimal headache and mild neck stiffness |
| I.A. | Absence of meningeal or cerebral symptoms, but presence of persistent neurological deficit |
| II | Moderate to severe headache, stiff neck; no neurological deficit other than cranial nerve palsy |
| III | Drowsiness, confusion (disorientation in time and space), or mild local deficits |
| IV | Stupor, moderate to profound hemiparesis, possible early decerebrate rigidity and autonomic disturbances |
| V | Deep coma, decerebrate rigidity and signs of agony |
Hemorrhage into the pons is usually characterized by early development of coma, pinpoint pupils that do not respond to light, and bilateral decerebrate rigidity.
Hemorrhage into the cerebellum is characterized by sudden dizziness, vomiting in combination with severe ataxia, abasia, aesthesia and gaze paresis. Consciousness is not impaired, but compression of the trunk can lead to death.
Subarachnoid hemorrhage. Aneurysm rupture. Subarachnoid hemorrhage (SAH) is most often caused by the rupture of a saccular aneurysm, a defect in the internal elastic membrane of the arterial wall, usually occurring at the site of a bifurcation or branch of an artery. In most cases, the gap occurs between the ages of 35-65 years. There may be associated anomalies such as polycystic kidney disease or coarctation of the aorta. Sudden, unexplained headache of any location should raise suspicion of SAH and a computed tomography (CT) scan should be performed. For aneurysms larger than 7 mm, microsurgical obliteration is justified.
Another type of aneurysm is located along the internal carotid, vertebral or basilar artery; Depending on their structure, they are divided into fusiform, spherical and diffuse. Such aneurysms become clinically apparent when they put pressure on adjacent structures or due to thrombosis, but rarely rupture.
Table 2. Classes of social and everyday activity(Schmidt E.V., Makinsky T.A., Research Institute of Neurology, 1979) | |
| I | Return to work and complete independence from others |
| II | Return to work with limitations, independence in activities of daily living, walking without assistance |
| III | Limitation of previous household duties, partial dependence on others in everyday life, walking around the apartment without assistance, walking down the street with assistance |
| IV | The impossibility of returning patients who previously worked and suffered a stroke to work; for those who were engaged in housework, there is a significant limitation in the range of household duties or a complete inability to perform them, significant dependence on others in everyday life. Walking around the apartment with assistance. Sick people don't walk down the street |
| V | Complete loss of any productive activity. Complete dependence on others in everyday life |
A ruptured aneurysm is characterized by a sudden, intense headache. The patient usually says that he has never experienced such a severe headache before. Possible loss of consciousness; sometimes it turns into a coma, but more often consciousness is restored, although stupor remains. In some cases, loss of consciousness occurs suddenly, before the headache appears. SAH often occurs during exercise. When an aneurysm ruptures, the diagnosis is usually simple, but sometimes at an early stage there are no objective symptoms, so if there is a sudden headache, the doctor must think about subarachnoid hemorrhage.
Meningeal symptoms and low-grade fever are often present. Ophthalmoscopy often reveals subhyaloid hemorrhages.
Hemorrhage may be limited to the subarachnoid space or spread to the brain, causing focal symptoms. Sometimes, soon after hemorrhage, an ischemic stroke develops due to impaired blood flow or thrombosis in the arteries affected by the aneurysm.
It is not easy to determine the location of an aneurysm clinically, although it is sometimes possible. Thus, pain in the depths of the orbit and damage to the II-VI cranial nerves indicate an aneurysm of the cavernous part of the carotid artery; hemiplegia, aphasia and a number of other symptoms - for an aneurysm of the middle cerebral artery; damage to the third cranial nerve - an aneurysm at the junction of the posterior communicating and internal carotid arteries; abulia and weakness in the leg - due to an aneurysm of the anterior communicating artery; damage to the lower cranial nerves - an aneurysm of the basilar or vertebral artery.
A transient or persistent focal neurological defect that develops several days after a stroke is usually caused by a spasm of cerebral vessels that occurs in response to blood entering the subarachnoid space. Both an early and late complication of SAH can be hydrocephalus, which sometimes requires ventricular bypass.
Arteriovenous malformations. Arteriovenous malformations usually manifest as epileptic seizures or hemorrhage, but with large lesions, ischemia of adjacent areas of the brain may occur due to large blood flow. Most often this is a combined parenchymal-subarachnoid hemorrhage. People usually suffer from arteriovenous malformations in childhood and adolescence. That is why, for persistent headaches at this age, listening in the area of the orbit, carotid artery, and mastoid process is necessary.
The presence of vascular murmurs in these areas is pathognomonic. In doubtful cases, as well as for the purpose of differential diagnosis of telangiectasia and other angiomas, a CT scan can be done.
- Diagnosis of hemorrhagic stroke
CT is the method of choice. It allows not only to confirm the diagnosis, but also to determine the extent of the lesion in intracerebral parenchymal hemorrhages. CT is the best method for diagnosing SAH, and in most cases reveals blood in the subarachnoid space. This method also makes it possible to diagnose cerebral edema, parenchymal and intraventricular hemorrhage, and hydrocephalus. It is possible to identify the localization of the source in intrathecal hemorrhage.
Magnetic resonance imaging (MRI) compared to CT is more reliable in diagnosing small hematomas localized in the pons and medulla oblongata, as well as hematomas in which the X-ray density of blood clots inside is equal to the density of brain tissue. MRI also makes it possible to identify arteriovenous malformations that are accessible to surgical intervention, which are very difficult to diagnose with CT, especially without contrast enhancement.
Cerebrospinal fluid examination is indicated only in cases where computed tomography is not available. Blood in the cerebrospinal fluid is detected in all cases of SAH, as well as with hemorrhages in the cerebellum and pons; with minor hemorrhages in the putamen and thalamus, red blood cells may appear in the cerebrospinal fluid only after 2-3 days.
X-ray of the skull reveals calcified malformations and aneurysms. As a rule, it is not carried out.
Cerebral angiography is usually performed immediately before surgery to clarify the location and anatomical nature of the aneurysm, as well as to confirm the presence or absence of focal cerebral vagospasm. In severe cases, angiography is best performed only when the diagnosis is unclear and especially when surgical decompression is indicated.
- Differential diagnosis of strokes
Cerebral crises precede cerebral hemorrhage; the disease begins violently, suddenly, often during the day due to physical stress or excitement. Precursors are characteristic (flushing to the face, headache, seeing objects in red); prolonged comatose states develop (sometimes several days); the face is hyperemic; temperature rises; breathing is bubbling, hoarse; pulse intense, rare; accent of the second tone at the top; blood pressure is increased; miosis or mydriasis on the side of the lesion; focal symptoms are identified in the form of rapid development of hemiplegia with a decrease in muscle tone, reflexes, and skin temperature; sometimes epileptiform seizures or early contractures (tonic spasms, protective hyperreflexia) occur; pronounced meningeal phenomena, brainstem disorders (breathing disorders, vomiting, floating movements of the eyeballs); pseudobulbar reflexes are rarely detected, urinary retention or incontinence is observed; retinal hemorrhages are visible in the fundus; cerebrospinal fluid is hemorrhagic, xanthochromic, pressure is increased; leukocytosis in the blood, prothrombin is not increased; in the urine there are red blood cells, sometimes sugar and protein.
Ischemic thrombotic stroke is preceded by transient cerebrovascular accidents. The disease develops gradually, more often at night, in the morning or during sleep; there are warning signs (dizziness, short-term disturbances of consciousness); characterized by incomplete or short-term loss of consciousness; the patient's face is pale, the temperature usually does not rise; slow breathing, weak pulse; heart sounds are muffled; blood pressure is not elevated; the size of the pupils most often does not change; focal symptoms appear in the form of hemiplegia or monoplegia with low muscle tone, one-sided Babinski reflex; hemiplegia develops gradually and is unstable; epileptiform seizures are not typical; there are no meningeal phenomena; stem phenomena are rarely observed (with extensive foci); with repeated strokes, pseudobulbar reflexes occur; sometimes there is urinary incontinence; narrowing and unevenness of blood vessels are visible in the fundus; the cerebrospinal fluid is clear, the pressure is normal; hypercoagulation is detected in the blood; urine specific gravity is low.
Non-thrombotic ischemic stroke is preceded by crises, angina, myocardial infarction, etc.; the disease develops suddenly during the day, more often after physical activity; often without warning; characterized by short-term loss of consciousness, stupor; the face is pale; the temperature is elevated; weakened, slow breathing; pulse is arrhythmic, weakened; muffled heart sounds, sometimes atrial fibrillation; blood pressure is low, pupils are constricted; transient hemiplegia develops with mildly increased muscle tone and a one-sided Babinski reflex; epileptiform seizures are rare; meningeal and stem phenomena are rare; pseudobulbar reflexes are often detected; there is urinary incontinence; sclerosis and narrowing of retinal vessels are visible in the fundus; cerebrospinal fluid is clear, its pressure is sometimes increased; Prothrombin is increased in the blood, traces of protein are detected in the urine.
- Treatment of hemorrhagic stroke
General principles. Along with differentiated therapy for hemorrhagic stroke, basic therapy aimed at maintaining vital body functions plays an important role. The more severe the course of the stroke, the more necessary is multilateral and complex basic therapy, which is carried out individually, under the control of laboratory parameters and the functions of all organs and systems.
In connection with modern pathogenetic concepts, early diagnosis of cerebral stroke, clarification of its nature and organization of emergency medical care at the prehospital and hospital stages are of particular importance. The effectiveness of treatment measures depends on the timeliness of their initiation and on the continuity of therapy in all periods of the disease.
The continuity of treatment measures is determined by the general tactics of patient management and is associated with solving organizational problems: rapid transportation of the patient, clear organization of the work of the emergency department; early clarification of the diagnosis and resolution of the issue of referral to the appropriate department; smooth operation of all levels of assistance.
Neurosurgical intervention. The problem of hemorrhagic stroke, according to most researchers, is largely neurosurgical. If ischemic stroke is a process of development of hemodynamic and metabolic changes, ending mainly a few days after an acute cerebrovascular accident, then hemorrhagic stroke is a fait accompli of hemorrhage, and its pathogenesis involves secondary phenomena of already shed blood.
Removal of a hematoma after an intracerebral hemorrhage, if it is localized in an accessible area of the brain (for example, in the cerebellum, putamen, thalamus, or temporal lobe), can save the patient's life. The operation is indicated as early as possible (24-48 hours) for aneurysm ruptures, if the patient’s condition does not improve and signs of herniation appear. The main operation is clipping the neck of the aneurysm; wrapping the aneurysm with muscle or, less commonly, extracranial occlusion of the internal carotid artery is also performed.
Patients whose condition corresponds to grade 0 - III on the Hunt scale have no contraindications on this scale for hospitalization in the neurosurgical department (Table 1).
Differentiated conservative therapy. Conservative therapeutic interventions for hemorrhagic stroke should be aimed at rapid correction of blood pressure to optimal values for a particular patient; to combat developing cerebral edema and to carry out hemostatic and vascular wall-strengthening therapy.
Correction and control of blood pressure. If possible, blood pressure (BP) should be avoided. They try to keep the blood pressure within normal limits using antihypertensive drugs (beta blockers, calcium antagonists, antispasmodics, ACE inhibitors). To prevent emotional reactions, sedative therapy (diazepam, elenium) is prescribed. Sometimes phenobarbital is prescribed for prophylactic purposes (30 mg orally three times a day), since it also has an anticonvulsant effect.
To avoid straining, laxatives (regulax, glaxena, senade, etc.) are prescribed. It is necessary to create conditions for “protective inhibition”; protect from light and noise.
Hemostatic therapy and therapy aimed at strengthening the vascular wall. Prescribe dicinone (sodium ethmazilate) intravenously or intramuscularly (250 mg four times a day); antiprotease drugs for 5-10 days: gordox (100 thousand units four times a day intravenously) or contrical (30 thousand units immediately, and then 10 thousand units twice a day intravenously).
Calcium preparations (calcium pantothenate, berrocca, calcium gluconate - i.m., calcium chloride - i.v.), rutin, vikasol, ascorbic acid strengthen the vascular wall well.
Antifibrinolytic therapy in the form of gamma-aminocaproic acid up to 30 g per day (100-150 ml of a 5% solution intravenously, then orally) is of great importance. It can be administered with small doses of rheopolyglucin, which improves microcirculation.
Fighting cerebral edema. If lethargy or signs of herniation appear, it is better to prescribe osmotic diuretics mannitol (0.5 - 1.5 g/kg of the patient’s body weight, IV) or glycerin (1 g/kg orally). Less commonly prescribed corticosteroids are dexazone according to the scheme (8+4+4+4 mg IV). More effective are Lasix (20 mg IV twice a day) and/or Reogluman (200 ml IV drip twice a day).
Treatment of spasm of cerebral vessels. Signs of cerebral vasospasm (drowsiness, focal symptoms) appear after two to three days and most often on the seventh day after a hemorrhagic stroke. It is believed to be caused by the release of serotonin, catecholamines, peptides and other vasoactive substances. Prescribed for spasms, and even better for preventive purposes in advance. Calcium antagonists - nimoton (10 mg IV drip) - 10-14 days or nimodipine (30-60 mg orally every four hours). In this case, correction of antihypertensive therapy is necessary, since calcium antagonists affect blood pressure.
Rehabilitation treatment. Rehabilitation therapy is carried out over a long period of time and at all stages of treatment, but it is especially important after the acute period of a stroke. Physiotherapy exercises are combined with physiotherapy, acupressure and classical massage, acupuncture, electrical stimulation, and magnetotherapy.
Occupational therapy is required - training in self-care skills, work on training stands and work simulators. Psychotherapy is effective: individual, group, family; Autogenic, adaptive training, etc. are recommended. Speech therapy classes are required for persons with speech impairments.
The patient needs treatment for a total of at least three to four months. For severe strokes, depending on the patient’s condition, this period can be extended to six months or more. Patients are registered at the dispensary. With a prolonged period of restoration of functions, patients are transferred to disability.
- Work ability examination
Currently, there are five classes of social and everyday activity (Table 2).
The disability group is determined according to the severity of dysfunction and profession. Patients with paralysis of the limbs and aphasia need care from outsiders and are recognized as group I disabled people. In case of deep paresis, when the ability to self-care remains, but the ability to work is lost, disability group II is assigned. Group II patients adapt to working from home: typing, assembling parts, doing dispatch activities on the phone, etc.
Literature
1. Bogolepov N.K. Clinical lectures on neurology, 1971. 2. Internal diseases. Ed. Harrison T. R., vol. 10, 1997. 3. Gusev E. I., Skvortsova V. I., Chekneva N. S. et al. Treatment of acute cerebral stroke (diagnostic and therapeutic algorithms), M., 1997. 4. Allen GS, et al. Cerebral arterial spasm: A controlled trial of nimodipine in patients with subarachnoid hemorrage. //N. Engl. J. Med. 308:619, 1983. 5. Cerebral embolism study group. Brain hemorrhage and management options. Stroke 15:779, 1984. 6. Curling OD et al. An analysis of natural history of cavernosus angiomas. J Neurosurgery 75:702, 1991. 7. Henry JM, Barnett. Stroke: Pathophysiology, Diagnosis, Management. 1986. 8. Manual of Neurologic Therapeutics. Edited by Martin A. Samuels, MD 1995. 9. Nibbelink DW, Torner JC, Henderson WG Interactional aneurysms and subarachnoid hemorrage: A cooperative study. Antifibrinolytic therapy in recent onset subarachnoid hemorrhage. Stroke 6:662, 1975. 10. Origitano TC et al. Sustained increased cerebral blood flow with prophylactic hypertensive hypervolemic hemodilution (“Triple-H Therapy”) after subarachnoid hemorrage. Neurosurgery 27:729, 1990. 11. Wilkins RH Natural History of Intracranial Vascular Information: A review. Neurosurg 16:421, 1985.
Complications of SAH
Analysis of the results of transcranial Doppler sonography showed that subarachnoid hemorrhage is almost always complicated by spasm of cerebral vessels. However, clinically significant spasm is observed, according to various sources, in 30-60% of patients. Cerebral vasospasm usually develops within 3-5 days. SAH and reaches a maximum on days 7-14. Its degree directly correlates with the volume of blood shed. In 20% of cases, primary subarachnoid hemorrhage is complicated by ischemic stroke. With repeated SAH, the incidence of cerebral infarction is 2 times higher. Complications of SAH also include concomitant hemorrhage into the brain parenchyma and breakthrough of blood into the ventricles.
In approximately 18% of cases, subarachnoid hemorrhage is complicated by acute hydrocephalus, which occurs when the outflow of cerebrospinal fluid is blocked by the resulting blood clots. In turn, hydrocephalus can lead to swelling of the brain and dislocation of its structures. Somatic complications include dehydration, hyponatremia, neurogenic pulmonary edema, aspiration or congestive pneumonia, arrhythmia, myocardial infarction, decompensation of existing heart failure, pulmonary embolism, cystitis, pyelonephritis, stress ulcer, and GI bleeding.
Classification of hemorrhages in the ventricles of the brain
Hemorrhages in the ventricles of the brain are divided into:
- Primary. They are observed very rarely (about one case out of three hundred).
- Secondary. They make up the bulk of hemorrhages of this type.
Parenchymal type hemorrhage is divided into 3 types:
- Hemorrhage into the lateral ventricles. With this type of hemorrhage, the anterior and posterior parts of the ventricles are affected, less often the central one. In this case, a syndrome of increased intracranial pressure and compression of the brain stem with blood may occur. If the bleeding is extensive, then the rush of blood usually occurs through the optic tubercle or caudate compartment. Next, the blood enters the third ventricle through the foramen of Monroy and the lateral ventricle of the adjacent hemisphere. The foramen of Luschka then passes through the aqueduct of Sylvius and enters the subarachnoid space of the spinal cord and brain.
- Hemorrhage into the third ventricle. Occur through the optic thalamus. Sometimes a rush of blood is observed in several parts of the ventricular system at once.
- Hemorrhage into the fourth ventricle.
There are several options for hemorrhage into the ventricles of the brain.
- Massive hemorrhages that destroy the walls of the third ventricle. In such cases, a very large volume of blood is poured out, which fills the entire ventricular system in a relatively short time. Extensive necrosis occurs in the brain. If surgery is performed, it is flattened. This type of hemorrhage leads to the death of the patient within about 24 hours.
- A rush of blood moves from the parenchyma to the lateral ventricle and fills several horns of the cavity of this ventricle or its entire space at once. Next, the blood fills the third ventricle and the lateral ventricle of the opposite hemisphere and enters the ventricle through the aqueduct of Sylvius. With a large volume of blood spilled, the volume of the brain also increases, this causes bilateral symptoms. The course of the pathology is about five days. There is a rupture of the gray matter under the corpus callosum, thus blood penetrates from the region of the basal ganglia into the lateral ventricle. In this case, the difference in the density of white and gray matter plays a big role.
- Hemorrhage into the third ventricle can be caused by parenchymal lesions medial to the optic thalamus. Symptoms increase quickly, which leads to rapid death. Surgical intervention in such cases is performed extremely rarely due to the inaccessibility of the lesion. Lateral lesions have a more favorable prognosis and make it possible to perform surgical intervention. In such cases, a rush of blood fills the anterior or posterior horn of the lateral ventricles and provokes hemorrhage into the intrathecal spaces.
- As a result of hemorrhage, the lateral ventricle is partially filled with blood when hemorrhaging into the brain parenchyma. The hemorrhage does not spread to other ventricles. Such pathologies most often have a long course.
- There are also extensive parenchymal hemorrhages, in which the lateral ventricle is completely filled with blood and a significant displacement of the oral part of the brain stem occurs. As a result of compression, the passage into the foramen of Monroe narrows and is completely blocked, so blood does not penetrate further into the third ventricle. In this regard, the cavity of the lateral ventricle in the adjacent hemisphere of the brain expands significantly. Thus, contralateral hydrocephalus occurs.
- Hemorrhage into the third ventricle. Basically, blood gets there from the parenchyma after hemorrhage in the area of the visual thalamus. In rare cases, the blood flow originates in the choroid plexuses.
- Blood enters the gastric system from the cerebellum. There are frequent cases of blood entering the third ventricle, and the ventricular cavity fills quickly and completely. This type of hemorrhage leads to the rapid death of the patient.
There are different options for classifying this type of pathology.
According to one of them, there are four stages of hemorrhage in the ventricles of the brain:
- Grade 1 - a small amount of blood accumulates around the vessels. This type of hemorrhage is called subependymal. It is not life-threatening and most often goes away on its own after some time without any consequences.
- 2nd degree - blood enters the ventricular cavity, but has little effect on the patient’s life. In most cases, it resolves on its own, often without consequences.
- Stage 3 - a blood clot enters the ventricular passage and blocks it, thereby causing the volume of the ventricle to expand as it fills with blood. Sometimes the elimination of such pathology occurs spontaneously, by itself. But in some cases, surgical intervention is still necessary, in which a shunt is installed to unblock the ventricular passage and prevent the development of hydrocephalus. Neurological symptoms are often observed.
- 4th degree - blood enters both the ventricles of the brain and its parenchyma. This pathology poses a threat to the patient’s life and is accompanied by severe neurological symptoms (frequent seizures, development of anemia, etc.).
According to another classification, there are three stages of hemorrhage in the ventricles of the brain:
- Subepindeminal - hemorrhage under the layer of tissue lining the internal cavity of the ventricle. It occurs in premature babies and is characterized by the absence of neurological symptoms.
- Subepindamal-intraventricular hemorrhage into the ventricular cavity. It occurs in premature babies and is accompanied by a state of shock, respiratory tract pathology (the child cannot breathe independently), increased intracranial pressure, convulsions, and in some cases coma.
- Subepindeminal-intraventricular-periventricular is a hemorrhage in which not only the ventricle is saturated with blood, but also the tissue that surrounds it. It is observed in premature babies. This stage is characterized by shock, convulsions, respiratory tract pathologies, increased intracranial pressure, and dysfunction of the brain stem.
Diagnostics
A typical clinical picture allows a neurologist to suspect subarachnoid hemorrhage. In the case of atypical forms, early diagnosis of SAH seems very difficult. All patients with suspected subarachnoid hemorrhage undergo a CT scan of the brain. The method makes it possible to reliably establish a diagnosis in 95% of SAH; identify hydrocephalus, bleeding into the ventricles, foci of cerebral ischemia, cerebral edema.
- Visualization techniques. Detection of blood under the arachnoid membrane is an indication for cerebral angiography to determine the source of bleeding. Modern non-invasive CT or MRI angiography is performed. In patients with the most severe degree of SAH, angiography is performed after their condition has stabilized. If the source of bleeding cannot be determined, repeat angiography is recommended after 3-4 weeks.
CT scan of the brain. Hyperdense blood in the subarachnoid liquor spaces
- Lumbar puncture. If subarachnoid hemorrhage is suspected, it is performed in the absence of CT and in cases where, in the presence of a classic clinical picture of SAH, it is not diagnosed by CT. Detection of blood or xanthochromia in the cerebrospinal fluid is an indication for angiography. In the absence of such changes in the cerebrospinal fluid, another cause for the patient’s condition should be sought.
- Ultrasound methods. Transcranial Doppler Doppler Doppler Doppler and Doppler Doppler Doppler Doppler (USD) of cerebral vessels make it possible to detect vasospasm in the early stages of SAH and monitor the state of cerebral circulation over time.
During diagnosis, subarachnoid hemorrhage should be differentiated from other forms of stroke (hemorrhagic stroke, TIA), meningitis, meningoencephalitis, occlusive hydrocephalus, traumatic brain injury, migraine paroxysm, pheochromocytoma.
Symptoms of hemorrhage in the ventricles of the brain
One of the very first symptoms is the rapid development of a coma. If the rush of blood into the ventricles occurs quickly, then a rapid loss of consciousness is observed. If the ventricular system is filled with blood gradually, then consciousness is not lost immediately, but after some time.
As the volume of blood in the ventricles increases and swelling occurs, the loss of consciousness becomes deeper, respiratory distress, changes in pulse, vasomotor disorders in the face, limbs and in the torso itself, and cyanosis are observed. Damage to the brain causes hemipreparalysis of gaze in the opposite direction. Jumps in body temperature may be observed - initially the temperature drops below normal, but during the day it may rise significantly (up to 40), and if blood enters the third ventricle, the temperature can reach critical levels - 42 degrees.
Laboratory tests show an increase in leukocytes in the blood, sometimes protein and sugar are present.
Early contracture can also be considered a sign of hemorrhage in the ventricles of the brain. Periodic tonic spasms are observed, occurring spontaneously or during respiratory movements. Tonic spasm is a condition during which the head is thrown back, the legs are convulsively extended, and the arms are bent and clenched in the fingers.
If hemorrhage occurs in the lateral ventricles, then the following clinical picture is observed:
- the comatose state develops rapidly;
- vomit;
- the frequency and rhythm of breathing is disrupted;
- change in heart rate - first it slows down and then increases;
- facial hyperemia;
- profuse sweating;
- severe increase in body temperature;
- pendulum-like movements of the eyeballs when the body is in a horizontal position;
- tonic convulsions during breathing;
- increased tendon reflexes and at the same time decreased skin reflexes.
Hemorrhages into the ventricle most often lead to rapid death, since the spilled blood affects vital centers.
Treatment of subarachnoid hemorrhage
Basic and specific therapy
Basic therapy for SAH consists of measures to normalize cardiovascular and respiratory functions and correct basic biochemical constants. In order to reduce hydrocephalus as it increases and relieve cerebral edema, diuretic therapy (glycerol or mannitol) is prescribed. If conservative therapy is ineffective and cerebral edema progresses with the threat of dislocation syndrome, decompressive craniotomy and external ventricular drainage are indicated.
Basic therapy also includes symptomatic treatment. If subarachnoid hemorrhage is accompanied by convulsions, anticonvulsants are included (lorazepam, diazepam, valproic acid); for psychomotor agitation - sedatives (diazepam, droperidol, sodium thiopental); for repeated vomiting - metoclopramide, domperidone, perphenazine. At the same time, therapy and prevention of somatic complications are carried out.
So far, subarachnoid hemorrhage does not have effective conservative methods of specific treatment that can stop bleeding or limit the amount of bleeding. In accordance with the pathogenesis, specific therapy for SAH is aimed at minimizing vasospasm, preventing and treating cerebral ischemia. The standard of therapy is the use of nimodipine and ZN therapy. The latter allows you to maintain hypervolemia, controlled hypertension and hemodilution, as a result of which the rheological properties of blood and microcirculation are optimized.
Surgery
Surgical treatment of SAH is optimal in the first 72 hours. It is performed by a neurosurgeon and is aimed at excluding the ruptured aneurysm from the bloodstream. The operation may consist of clipping the neck of the aneurysm or endovascular insertion of a balloon-catheter to fill its cavity. Endovascular occlusion is preferable in case of unstable patient condition, high risk of complications of open surgery, early vasospasm. With decompensation of cerebral vasospasm, stenting or angioplasty of the spasmed vessel is possible.
Treatment and prevention of hemorrhage in the ventricles of the brain
Even if this type of pathology is suspected, the patient requires urgent hospitalization and the necessary standard therapy - stabilization of respiratory function, blood pressure, normalization of body temperature, administration of anticonvulsants, and, if necessary, drugs to eliminate cerebral edema. Therapy is aimed at stopping bleeding.
Surgical treatment is carried out on a strictly individual basis, taking into account the patient’s condition and all contraindications. Surgical intervention after the onset of a coma is advisable only in the first 10-12 hours.
Prevention of hemorrhage into the ventricles of the brain includes, first of all, timely treatment of arterial hypertension, responsible use of medications, and treatment of blood clotting diseases.
Prognosis and prevention
In 15% of cases, subarachnoid hemorrhage ends in death even before medical care is provided. Mortality in the first month in patients with SAH reaches 30%. In coma, mortality is about 80%, in repeated SAH - 70%. Patients who survive often have residual neurological deficits. The prognosis is most favorable in cases where angiography fails to identify the source of bleeding. Apparently, in such cases, spontaneous closure of the vascular defect occurs due to its small size.
The probability of repeated hemorrhage every day of the first month remains at 1-2%. Subarachnoid hemorrhage of aneurysmal origin recurs in 17-26% of cases, with AVM - in 5% of cases, with SAH of other etiology - much less frequently. Prevention of SAH involves treatment of cerebrovascular pathologies, TBI and elimination of risk factors.
You can share your medical history of what helped you in the treatment of subarachnoid hemorrhage.