Congenital malformations of the fetus are not as common as we have already said - approximately every 30 pregnancies have clinically significant changes in the fetus, although small deviations or features in the development of one or another organ in the fetus are much more common.
It is the fact of the relative rarity of fetal pathology that causes carelessness among expectant mothers, and their motivation is the simplest - my husband and I are healthy, and, therefore, our children are also healthy! Alas, not everything is so rosy and simple!
A fairly common pathology (5 per 1000 births), but rarely diagnosed during pregnancy, and almost never diagnosed before the 20th week of pregnancy, is agenesis of the corpus callosum (CAC) . Among all fetal malformations, this pathology accounts for 2-3%.
— What is the corpus callosum, and why did it appear in the brain, where could the calluses come from? – you ask indignantly.
- This is a small but important part of the brain that ensures the exchange of information between the right and left hemispheres of the brain. Without it, the right and left hemispheres live on their own, and the two halves of the brain have independent capabilities to participate in the processes of consciousness, memory accumulation, communication and regulation of motor activity.
A precedent that has become a parable is created when “the right hand does not know what the left hand is doing” - and, therefore, with agenesis of the corpus callosum, a significant intellectual deficit is expected in a person’s neurological development. In addition, seizures, large head sizes, giant brain cysts and cerebral palsy (up to 30%) are also consequences of AMT.
What conclusions should you draw:
- Diagnosis of fetal malformations is a responsible matter that does not tolerate haste and a superficial approach to research.
- in each trimester of pregnancy, new pathologies unique to this period of fetal development may be discovered. Don't miss screening deadlines
- The experience of a doctor-researcher + high-quality equipment is the key not only to timely diagnosis of fetal malformations, including agenesis of the corpus callosum, but also the key to a rational choice of further obstetric tactics.
Examination of the fetus and placenta for congenital malformations incompatible with life
Congenital malformations of the fetus are considered the most important medical and social problem, since they occupy a leading place in the structure of causes of perinatal, neonatal and infant morbidity, mortality and disability [1]. Also relevant is the problem of late termination of pregnancy for medical reasons from the fetus, since it accounts for about 20% of the total number of abortions, and the number of complications increases 3-4 times when terminating a pregnancy in the second trimester compared to the first [ 2]. According to WHO, congenital malformation occurs in 4–6% of children. In Russia, more than 50,000 children are born with congenital malformation every year; the number of patients with congenital malformation exceeds 1.5 million people. If the fetus has congenital malformations incompatible with life, or combined defects with an unfavorable prognosis for life and health, with congenital malformations leading to persistent loss of function due to the severity and extent of the lesion in the absence of effective treatment methods, the woman is provided with information about the possibility of artificial termination of pregnancy for medical reasons. indications [3]. If a woman refuses to terminate her pregnancy due to the presence of congenital malformations incompatible with life, or other combined defects, the pregnancy is carried out in accordance with Section I of this procedure. The high costs of treatment, care and rehabilitation of children with congenital malformation necessitate the development and improvement of not only methods for monitoring, diagnosing and preventing congenital malformation in children, but also studying the pathomorphology of the fetus and placenta [4].
In recent decades, numerous antenatal factors leading to damage to the fetal nervous system have been intensively studied - intrauterine infections, genetic defects, problems of Rh conflict, exposure to drugs on the fetus and a number of other factors. Often the causes of congenital malformations of the fetus and placenta are infectious causes: infectious fetopathies are formed from the 16th week, when the infection in the fetus is generalized, as a result of which malformations such as endocardial fibroelastosis, polycystic pulmonary disease, micro- and hydrocephalus (early fetopathies) can occur ) [5].
A large number of works are devoted to methods of late pregnancy termination for medical reasons from the fetus - congenital malformations of the fetus, rehabilitation of women after fetal elimination [6–11]. At the same time, the results of pathological examination of the fetus and placenta for congenital defects incompatible with life are not sufficiently described. Our study focuses on termination of pregnancy in the second trimester for medical reasons from the fetus. This publication is devoted to the issues of pathological examination of the fetus and placenta.
The purpose of this study was to identify the structure of congenital malformations of the fetus, incompatible with life, leading to termination of pregnancy for medical reasons, their combination with structural changes in the placenta.
Materials and research methods
The study was approved by the local ethics committee of the Federal State Budgetary Educational Institution of Higher Education Omsk State Medical University of the Ministry of Health of the Russian Federation, Omsk (No. 63 of 10/09/2014) and was carried out on the basis of the BUZOO GKPTS, Omsk. Termination of pregnancy in the second trimester for medical reasons was carried out in accordance with Order of the Ministry of Health of the Omsk Region No. 308-r dated September 17, 2013 in the specified institution, where a center for abortion of second trimester pregnancy was created and the woman was given a conclusion from a perinatal consultation by specialists (obstetrician-gynecologist, perinatologist, neonatologist, etc.). Histological examination of eliminated fetuses and placentas was carried out according to the recommendations of A.P. Milovanov and was carried out in the pathological department of the BUZOO ODKB, Omsk.
The main indication for termination of pregnancy at all stages was congenital malformations of the fetus incompatible with life. If the fetus has congenital malformation incompatible with life, or the presence of combined defects with an unfavorable prognosis for life and health, with congenital malformation leading to persistent loss of function due to the severity and extent of the lesion in the absence of effective treatment methods, information was provided on the possibility of artificial termination of pregnancy for medical reasons. indications. Artificial termination of pregnancy was carried out with the informed voluntary consent of the woman.
At the first retrospective stage (before the introduction of regulatory documents into practice [3, 12]), an analysis of the histological examination of placentas after termination of pregnancy was carried out in 150 women, who, depending on the method of termination, were divided into two groups: group A consisted of 75 women who underwent termination late pregnancy using transvaginal transcervical amniocentesis: amnioinfusion with 10% sodium chloride solution. Group B consisted of 75 women who, in order to terminate pregnancy in late stages, used dinoprostone gel for endocervical administration to induce and stimulate labor. Methods of abortion, their effectiveness and outcomes are described in more detail in our previous publications [13–15]. The criteria for inclusion of patients in groups A and B were the following: gestational age 18–21 weeks 6 days, the possibility of vaginal delivery and the absence of contraindications to the use of hypertonic sodium chloride solution (10% NaCl) and prostaglandins. The patients of both groups were identical in age, characteristics of menstrual function, the presence of extragenital and gynecological diseases, and parity. All patients were consulted in the medical genetic department.
At the second stage, 195 pregnant women were prospectively observed, divided into two groups. The main group consisted of 98 women who underwent late termination of pregnancy using the following combined method: oral mifepristone and injection of kelp into the cervical canal. The comparison group included 97 women whose pregnancy was terminated according to the WHO scheme. Criteria for inclusion in the groups: patients who have been given a conclusion by a council of doctors for termination of pregnancy for medical reasons from the fetus during the gestation period of 18–21 weeks according to orders of the Ministry of Health of the Russian Federation No. 736 dated December 3, 2007 [16] and No. 572n dated November 1, 2012 [3].
At the prospective stage of the study, the material for study was the results of a pathomorphological examination of fetuses (autopsy material) and placenta (macroscopic and microscopic). Anthropometric, organometric, and histological methods were used in the work. In order to clarify the gestational age of the fetus and additional hidden developmental anomalies, anthropometric and organometric studies were used in accordance with existing standards [17–20]. Histological studies of fetal organs, membranes, umbilical cord and placenta were carried out on paraffin sections prepared according to standard methods and stained with hematoxylin and eosin, and also selectively with picrofuchsin using the Van Gieson method. For histological examination, the material was first fixed in 10% neutral formalin, and after washing and standard processing, it was embedded in paraffin. Paraffin sections 3–5 µm thick were stained with hematoxylin and eosin. Elements of connective tissue were determined by picrofuchsin using the Van Gieson method. The methods of histological examination were carried out according to the instructions set out in the classical manuals on histological techniques and histochemistry. The examination of eliminated fetuses included a thorough visual assessment of existing stigmata of embryogenesis and congenital defects. For histological examination, organ fragments were selected to study their histoarchitecture [17].
The method of statistical processing of the results using the Student's t-table test was used, which allows one to calculate the degree of reliability of differences with a small number of observations. Before each calculation of the reliability of differences between quantitative characteristics, as well as to select a correlation criterion, the normality of their distribution was assessed using the Kolmogorov–Smirnov criterion. In case of non-normal distribution of quantitative characteristics or inequality of variances, the Mann–Whitney U test was used. For factors with a binomial distribution, 95% confidence intervals were additionally calculated.
Research results
Patients of all groups were identical in age, characteristics of menstrual function, the presence of extragenital and gynecological diseases, and parity. The effectiveness of late pregnancy termination using amniocentesis was 93.3%, with the use of prostaglandins - 92%, at the prospective stage there were no significant differences and was 99.0% in the main group and 96.9% in the comparison group.
In the structure of identified congenital malformations of the fetus, congenital malformations of the cardiovascular system were in first place in the main group (34 observations - 34.7%), in second place were defects of the central nervous system (CNS) (29 observations - 29.6%), in third — multiple malformations (13–13.3%), fourth — defects of the urinary system (9–9.2%) (Table 1). In the remaining observations, congenital malformations of the musculoskeletal system (7–7.1%) and others (6–6.1%) were identified: skin and muscles, gastrointestinal tract, lungs, neck and face, and others. In the comparison group, congenital malformations of the cardiovascular system were also in first place (32 observations - 33.0%), in second place were defects of the central nervous system (30 observations - 30.9%), in third place were multiple malformations (15–15, 5%), in fourth place are defects of the urinary system (10–10.3%). In the remaining observations, congenital malformations of the musculoskeletal system (8–8.2%) and others (2–2.1%) were identified: skin and muscles, gastrointestinal tract, lungs, neck and face, and others.
Among the defects of the cardiovascular system in both groups, transposition of the great vessels, defects of the interventricular and interatrial septa, common arteriovenous canal, tetralogy of Fallot, combined heart defects, Ebstein's anomalies, hypoplasia of the left side, and other congenital defects of the cardiovascular system were more often observed.
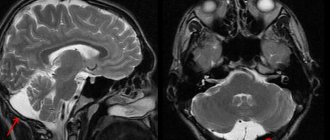
In the structure of CNS defects, hydrocephalus, anencephaly, Arnold–Chiari and Dandy–Walker syndrome, microcephaly, agenesis of the corpus callosum, acrania, spina bifida (spina bifida) were more often observed. Hydrocephalus is a disease characterized by excessive accumulation of cerebrospinal fluid in the ventricles and intrathecal spaces of the brain, accompanied by their expansion and atrophy of the brain matter.
During a retrospective assessment of the study of placenta in group A, in the vast majority of cases (78.7%) serous-purulent and purulent-necrotic deciduitis were determined, and only in a small percentage of cases (21.3%) serous deciduitis was observed. Also in this group, the presence of dyscirculatory disorders was noted (severe edema of the villous stroma, thrombosis of the intervillous space, retroplacental hematomas). In group B, serous parietal deciduitis was detected in most cases (54.7%), inflammatory changes were not detected in 38.7% of cases, serous-purulent parietal deciduitis was detected in 6.6% of cases.
At the retrospective stage, when examining the placenta, the pathological structure and malformations of the umbilical cord were found to a greater extent than in the placenta. Thus, in the first place among the signs of the pathological structure of the umbilical cord was a thin umbilical cord: 19 observations in the main group (19.4%) and 21 (21.6%) in the comparison group (Table 2). In second place were false umbilical cord nodes: 16 (16.3%) and 17 (17.5%), respectively, in the study groups, in third place were true umbilical cord nodes: 14 (14.2%) and 15 (15.5%) . Often in the structure of pathological variants of the umbilical cord structure there was a membrane attachment of the umbilical cord: 12 (12.2%) and 9 (9.3%), respectively. Hypo- and hyper-twisted umbilical cords were detected less frequently: 8 (8.2%) and 7 (7.2%), respectively, in the study groups; single umbilical cord artery: 6 (6.1%) and 4 (4.1%); umbilical cord hematoma: 1 (1.0%) in the main group and 2 (2.1%) in the comparison group. In total, during the study, abnormalities in the structure of the umbilical cord were identified in 76 cases of the main group and in 75 cases of the comparison group, in general in the study - in 77.4% of cases.
Histological examination of the placenta revealed relative preservation of the amniotic epithelium, vascular congestion and minor inflammatory changes (23 observations - 23.5% in the main group and 29–30.0% in the comparison group). Serous parietal deciduitis was detected in 17.3% of cases in the main group and 16.5% in the comparison group. Such scant changes in the placenta, revealed during the study, indicate that congenital malformations of the fetus, incompatible with life, are more often combined with pathology of the umbilical cord structure than with structural disorders and malformations of the placenta. Also, the relative preservation of the amniotic epithelium, vascular congestion and minor inflammatory changes indicate that the termination of pregnancy was carried out using a modern medical method, which imitates the spontaneous contractile activity of the uterus and does not cause gross changes in the placenta.
Thus, in the structure of identified fetal congenital malformations incompatible with life in the study groups, congenital malformations of the cardiovascular system were in first place, central nervous system defects were in second place, multiple malformations were in third place, and defects of the urinary system were in fourth place. In the remaining observations, congenital malformations of the musculoskeletal system and others were identified: the gastrointestinal tract, respiratory system, neck and face, and others.
In a histological examination of the placenta at the retrospective stage (before the introduction of modern methods of producing late induced abortion into obstetric practice), serous-purulent and purulent-necrotic membranitis were determined in the overwhelming majority during amnioinfusion with a hypertonic solution; when using dinoprostone, serous parietal deciduitis was more often observed. After the implementation of the regulatory Order 572n into the work of the obstetric and gynecological service, a histological examination of the placenta in second-stage patients of both groups revealed relative preservation of the amniotic epithelium, vascular congestion and minor inflammatory changes.
When examining the placenta, malformations of the umbilical cord were more common than those of the placenta. In the first place among the signs of the pathological structure of the umbilical cord was a thin umbilical cord, in second place were false umbilical cord nodes, and in third place were true nodes. Less commonly, the membrane attachment of the umbilical cord was determined. Much less frequently, a hypo- and hyper-tortuous umbilical cord and a single umbilical artery were identified; umbilical cord hematoma. Histological examination of the placenta revealed relative preservation of the amniotic epithelium, vascular congestion and minor inflammatory changes. The meager changes in the placenta (compared to changes in the umbilical cord) revealed during the study indicate that congenital malformations of the fetus, incompatible with life, are more often combined with pathology of the umbilical cord structure than with placental defects. Also, the relative preservation of the amniotic epithelium, vascular congestion and minor inflammatory changes indicate that the termination of pregnancy was carried out using a modern medical method, which imitates the spontaneous contractile activity of the uterus and does not cause gross changes in the placenta.
Literature
- Filippov O. S., Tokova Z. Z., Gata A. S., Kuzemin A. A., Gudimova V. V. Abortion: features of statistics in the Federal districts of Russia // Gynecology. 2021. Vol. 18. No. 1. pp. 92–96.
- Krasnopolsky V.K., Melnik T.N., Serova O.F. Safe abortion. M.: GEOTAR-Media, 2009. 48 p.
- Order of the Ministry of Health of Russia dated November 12, 2012 No. 572 n “On approval of the Procedure for the provision of medical care in the field of obstetrics and gynecology (except for the use of assisted reproductive technologies).”
- Obstetrics. National leadership / Ed. E.K. Ailamazyan et al. M.: GEOTAR-Media, 2015. 1197 p.
- Kuzmin V.N., Arslanyan K.N., Kharchenko E.I. Modern view on the problem of intrauterine infection // Attending Physician. 2021. No. 3. P. 44.
- Dicke G. B., Khamoshina M. B. Contraversions of safe and unsafe abortion // Doctor.Ru. 2014. T. 8. No. 96. pp. 73–77.
- Kravchenko E. N., Colombet E. V. Rehabilitation of women after late induced abortion with congenital malformations of the fetus // Treating Doctor. 2021. No. 8. P. 60.
- Radzinsky V. E. Medical abortion at different stages of pregnancy. Guide to outpatient care in obstetrics and gynecology / Ed. V. E. Radzinsky, 2nd ed., revised. and additional M.: GEOTAR-Media, 2014.
- American College of Obstetricians and Gynecologists (ACOG). A clinician's guide to medical and surgical abortion. NAF's textbook; 2012. Available at: https://www.prochoice.org.
- Royal College of Obstetricians and Gynecologists (RCOG). The care of women requesting induced abortion. London (England): Royal College of Obstetricians and Gynecologists (RCOG); 2011 Nov. 130 p. (Evidence-based Clinical Guideline; no. 7). Available at: https://www.rcog.org.uk.
- Safe abortion: technical and policy guidance for health systems. 2nd ed. World Health Organization, Department of Reproductive Health and Research; 2012. Available at: https://www.who.int/.
- Medical termination of pregnancy. Clinical recommendations of the Ministry of Health of the Russian Federation (treatment protocol) No. 15–4/10/2–6120 dated October 15, 2015, 34 p.
- Kolombet E. V., Kravchenko E. N., Sabitova N. L., Tsygankova O. Yu., Beznoshchenko A. B., Yaminova D. M., Andryushkiv V. B. Method of terminating pregnancy in late stages of pregnancy according to medical indications. Patent for invention No. 2580165 dated April 3, 2015. Published: April 10, 2016. Bulletin No. 10.
- Kravchenko E. N., Kolombet E. V. The effectiveness of modern methods of late pregnancy termination // Russian Bulletin of Obstetrician-Gynecologist. 2021. 3. pp. 64–68.
- Kravchenko E. N., Colombet E. V. Late induced abortion with congenital malformations of the fetus incompatible with life // Gynecology. 2021. T. 18. No. 5. pp. 44–49.
- Order of the Ministry of Health and Social Development of the Russian Federation of December 3, 2007 No. 736 “On approval of the list of medical indications for artificial termination of pregnancy.”
- Milovanov A.P. Pathology of the mother-placenta-fetus system: a guide for doctors. M.: Medicine, 1999. 447 p.
- Gagaev Ch. Pathology of the umbilical cord / Ed. V. E. Radzinsky. M.: GEOTAR, 2011, 96 p.
- Causes and differentiated treatment of early miscarriage (a guide for doctors) / Ed. A. P. Milovanova, O. F. Serova. M.: Studio MDV. 2011. 216 p.
- Extraembryonic and amniotic structures during normal and complicated pregnancy during normal and complicated pregnancy / Ed. V. E. Radzinsky, A. P. Milovanov. M.: MIA, 2004. 393 p.
E. N. Kravchenko*, 1, Doctor of Medical Sciences, Professor E. V. Colombet* A. E. Lyubavina**, Candidate of Medical Sciences
* Federal State Budgetary Educational Institution of Higher Education Omsk State Medical University of the Ministry of Health of the Russian Federation, Omsk ** BUZOO CSTO, Omsk
1 Contact information
On photographic materials from Dr. R. Shukhnin’s own practice:
Ultrasound, 26 weeks of pregnancy. Fetal head. Coronary section. Clear visualization of the corpus callosum (arrows)
Ultrasound, 29 weeks of pregnancy. Fetal head. Coronary section. Symptoms of agenesis of the corpus callosum of the brain are distinct (expansion of the occipital horns of the lateral ventricles, expansion of the 3rd ventricle of the brain, radial departure of the convolutions from its roof)
The same fruit. Facial profile with signs of pathological abnormalities: shortening of the bony dorsum of the nose.
Neurosonography. Patient 2 months Hydrocephalus. Clear visualization of the corpus callosum in coronal section.
Copying and distributing information without the consent of the author is prohibited!
fetal developmental anomalies hydrocephalus prenatal diagnostics in Pyatigorsk ultrasound of the fetal brain