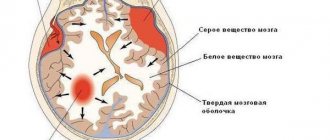
This terrible word "Cyst"
Infrequently, in about 1 in 30 pregnancies, an ultrasound scan of the fetus may reveal a cyst of the choroid plexus of the lateral ventricle of the brain. The word “cyst” usually causes tremors and panic in our population, as it is associated with the need for surgery or cancer.
However, as for the choroid plexus cyst of the brain, there is no need to panic. Typically, this is a benign finding, can be diagnosed from 15 weeks of pregnancy and usually continues to be observed until 28-32 weeks of pregnancy, after which most cases of these cysts resolve on their own.
Why then does the doctor mention these cysts if everything is so simple and safe? Wouldn't it have been easier to remain silent and ignore this discovery? - you ask.
The fact is that a cyst in the choroid plexus of the brain can appear for other reasons - for example, as a result of hemorrhage into this same choroid plexus, or as a consequence of an infectious process in the brain, or as a manifestation of a vascular aneurysm, and even as a manifestation of the cystic component of the tumor brain
That is why, when a choroid plexus cyst of the lateral ventricle of the brain is detected, not complacency should dominate the mood of the doctor and the patient, but alertness, and only a detailed analysis of the state of the brain and blood circulation in it, analysis of systemic indicators of fetal blood circulation, analysis of the results of infectious screening and screening of the state of all systems and fetal organs will be able to give an answer about the degree of danger of the detected cysts.
Choroid plexus cysts can be single or multiple, unilateral or bilateral, and their sizes also vary , but in general the prognosis of these cysts depends on other risk factors for fetal disease combined with them, for example, such as an increase in the thickness of the nuchal translucency or cervical fold , the presence of skeletal dysplasia, other malformations of the brain and heart, kidneys, facial structures of the fetus, etc.
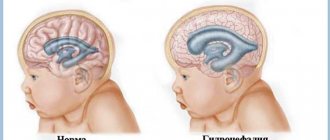
You need to understand that the choroid plexus and the lateral ventricle of the brain are not dimensionless , and when the size of the cyst is more than 9-10 mm, the fetus develops secondary ventriculomegaly (i.e., expansion of the lateral ventricles of the brain), which is accompanied by intracranial liquor hypertension and hydrocephalus.
According to statistics, cysts disappear by 28-30 weeks of pregnancy. This is also not entirely and not always true, and we provide photo examples from our own practice demonstrating choroid plexus cysts in both fetuses and newborns.
The same medical statistics note that in the presence of cysts of the choroid plexus of the lateral ventricles of the brain, such a formidable chromosomal disease of the fetus as trisomy 18, known to us as Edwards syndrome, is more often detected. Much less frequently, in the case of choroid plexus cysts, trisomy 21 (Down's disease) can also be detected. Therefore, the task of the doctor-ultrasound researcher when identifying a cyst of the choroid plexus of the lateral ventricle of the fetal brain is not just to state this fact, but to exclude other probable signs (markers) of these formidable genetic diseases.
And further. In postpartum ultrasound screening, a newborn undergoes a series of ultrasound examinations of the whole body (and in the case of an appointment at our center - ultrasound of the brain (neurosonography), echocardiography (ultrasound of the heart), ultrasound of the stomach, liver, gallbladder, pancreas, spleen, kidneys, ureters, bladder, hip joints, and in an expanded version - additionally the thymus gland, thyroid gland, intestines, reproductive organs (organs of the scrotum or uterus with appendages).
So, when performing neurosonography (ultrasound of the newborn’s brain), brain cysts are often discovered that were not detected during prenatal examinations. The point here, of course, is not the inattention of the ultrasound doctor, who “overlooked” the cysts during the examination of the fetus.
The detection of these cysts indicates trauma or infection suffered by the baby during childbirth, or in the early postpartum period. Cysts can also be found in the choroid plexuses, but their heterogeneous structure indicates the hemorrhagic nature of the cyst.
More often, newborn brain cysts are of a different nature and have a different localization. Thus, periventricular and subepindeminal cysts are found in children who have had cytomegalic or herpes infection, and in children who have had meningoencephalitis, cysts of the brain parenchyma are found due to necrosis (death) of tissues affected by the inflammatory process, as well as in children who have suffered severe ischemic-hypoxic brain damage . And don't forget about the possibility of subarachnoid cysts.
In newborns who have suffered hemorrhages into the brain parenchyma during the birth period due to resorption of hematomas, porencephalic cysts also form. This type of cyst has a periventricular, subcortical localization and does not affect the choroid plexuses of the lateral ventricles of the brain.
Thus, only a thorough ultrasound screening performed by an experienced specialist and using high-quality equipment allows: - to clearly determine the presence of a choroid plexus cyst;
— determine its prognostic value;
- exclude dangerous chromosomal diseases associated with the cyst, primarily disease
Down and Edwards disease;
- exclude hydrocephalic syndrome in the fetus
— trace the dynamics of cysts as pregnancy progresses
- determine delivery tactics
— after the birth of a child, during an ultrasound scan of the brain (neurosonography), a detailed assessment of the anatomy of the brain and the characteristics of blood circulation in it.
Only this approach to the health of the fetus, in the event of detection of choroid plexus cysts in the brain, WILL ENSURE THE BIRTH OF A HEALTHY, DESIRED CHILD.
Good health to everyone! R. Shukhnin.
In the photo from my own practice:
Unchanged choroid plexus of the lateral ventricle of the brain
Pregnancy 16 weeks. Small cyst of the choroid plexus of the right lateral ventricle of the brain
Ultrasound screening 2nd trimester: Cysts of the choroid plexus of the lateral ventricle of the brain at 18 weeks of pregnancy
Ultrasound 21 weeks pregnancy. 2 choroid plexus cysts of the left lateral ventricle of the brain
Pregnancy 28 weeks. Quite a large cyst of the choroid plexus of the left lateral ventricle of the brain
Newborn brain – choroid plexus cyst in the right lateral ventricle of the brain
Newborn brain – 3 small choroid plexus cysts in the right lateral ventricle of the brain
Newborn brain.
Subepindemal cyst of the lateral ventricle Down's disease hydrocephalus brain infections choroid plexus cysts of the brain meningoecephalitis porencephalic cyst screening Pyatigorsk subarachnoid cyst ultrasound pregnancy 4d ultrasound newborns Pyatigorsk
Choroid plexuses of the ventricles of the brain
Sagittal - a section running in the plane of bilateral symmetry of the body. Frontal - an incision running along the anterior-posterior axis of the body perpendicular to the sagittal. Basal (antonym: apical) - located at the base. Distal (antonym: proximal) - distant. Lateral (antonym: medial) - lateral. Medial (antonym: lateral) - middle.
Ticket 1
Anatomy and topography of the fourth ventricle of the brain and its walls. Pathways for the outflow of cerebrospinal fluid
The 4th ventricle is part of the rhombencephalon. Rhombencephalon: medulla oblongata, cerebellum, isthmus of the rhombencephalon. Ventriculus quartus. The bottom of the 4th ventricle is the posterior surface of the pons and medulla oblongata, the roof is in the region of the cerebellum. The bottom of the 4th ventricle is a rhomboid fossa. The rhomboid fossa is the shape of a diamond. Formed by the posterior surface of the pons and the medulla oblongata from below
.
The border
between the upper part of the rhombencephalon and the lower part of the rhomboid fossa is
the medullary striae of the 4th ventricle
.
Inferiorly, the 4th ventricle continues through the central canal of the spinal cord. At the top, through the cerebral aqueduct, it connects with the third ventricle. The roof of the fourth ventricle is formed by the superior medullary velum
.
The superior medullary velum is stretched between the superior cerebellar peduncles and the inferior medullary velum. From the cavity of the fourth ventricle, the vascular base of the fourth ventricle is adjacent to the inferior medullary velum. This vascular framework
is formed by the invagination of the pia mater into the fissure between the inferior surface of the cerebellum above and
the inferior medullary
velum below.
The velum forms an angle that projects somewhat into the cerebellum
.
The bottom of the fourth ventricle is a rhomboid fossa, which is formed by the pons
and
medulla oblongata
. The cerebrospinal fluid that fills the subarachnoid space is produced by the choroid plexuses of the ventricles of the brain. From the lateral ventricles, through the right and left interventricular foramina, cerebrospinal fluid enters the third ventricle, where there is also a choroid plexus. From the third ventricle, through the Sylvian aqueduct of the brain, cerebrospinal fluid enters the fourth ventricle, and from it into the subarachnoid space of the brain and spinal cord. Liquor is reabsorbed into the blood of the venous sinuses and through the granulations of the arachnoid membrane. Functions of cerebrospinal fluid: Protects the brain and spinal cord from mechanical influences, ensures the maintenance of constant intracranial pressure and water-electrolyte homeostasis. Supports trophic and metabolic processes between the blood and the brain, the release of the products of its metabolism.
Ticket 2
Anatomy and topography of the lateral ventricles of the brain and their walls. Choroid plexuses of the ventricles of the brain. Pathways for the outflow of cerebrospinal fluid
The lateral ventricles (ventriculus lateralis) are located in the thickness of the cerebral hemispheres. And they are their cavities. They communicate with the 3rd ventricle through the interventricular foramen ( foramen
interventriculare )
.
There are left and right ventricles (left and right hemispheres
). Parts of the lateral ventricles: central (corresponding to the parietal lobe), anterior horn (corresponding to the frontal lobe), posterior horn (occipital lobe), inferior horn (temporal lobe). 1) Central part (pars centralis) upper wall - corpus callosum bottom - body of the caudate nucleus, partially the dorsal surface of the thalamus and the posterior leg of the fornix; the lateral wall is absent. Contains the choroid plexus 2) Anterior horn medial wall - lamina pellucida lateral wall - head of the caudate nucleus anterior, superior, inferior walls - fibers of the corpus callosum 3) Posterior horn superior lateral wall - fibers of the corpus callosum. The remaining walls are the white matter of the occipital lobe on the lower wall there is a collateral triangle 4) The lower horn is lateral, the upper is the white matter of the temporal lobe, the medial and lower wall is the hippocampus (belongs to the limbic system) contains the lateral eminence - a continuation of the collateral triangle located on the lower wall of the posterior horns
These are structures located in the area of the roof of the third and fourth ventricles, and, in addition, in the region of part of the walls of the lateral ventricles. They are responsible for producing approximately 70-90% of cerebrospinal fluid. It is worth noting that 10-30% is produced by tissues of the central nervous system, and also secretes ependyma outside the choroid plexuses. They are formed by branching protrusions of the pia mater of the brain, which protrude into the lumen of the ventricles
Cerebrospinal fluid from the lateral ventricles of the brain enters the third ventricle, and then through the aqueduct of Sylvius into the fourth ventricle, from there into the cisterns of the base of the brain and onto the convexital surface of the brain. A smaller part of the C. descends into the subarachnoid space of the spinal cord. Circulation of the blood caused by changes in hydrostatic pressure in the cerebrospinal fluid pathways, pulsation of intracranial arteries, changes in venous pressure and body position, etc.
Ticket 3
Corpus callosum, cerebral fornix, anterior commissure, internal capsule place in the functions of the nervous system.
Corpus callosum (white fibers) - located in the telencephalon, visible on the medial section, the groove of the corpus callosum (sulcus corporis calosi) separates it from the cingulate gyrus (gyrus cinguli). There is an elongated middle part, or body (truncus corporis callosi), a rear thickened part, a roller (splenium corporis callosi), and an anterior arched part, the knee (genu corporis callosi), which thins, sharpens and forms a beak (rostrum corporis callosi), and then downwards there is a thin rostral plate (lamina rostralis, BNA). Below the corpus callosum is the septum pellucidum, the fornix of the brain, and the 3rd ventricle. Consists of commissural fibers - connects identical centers of different hemispheres, forming the radiation of the corpus callosum (radiation corporis callosi).
Vault
(fornix) - a strand of white material, there is a body of the arch, a leg and a column. The body is located under the corpus callosum, from above it fuses with the lower edge of the transparent septum and the lower surface of the corpus callosum. It flies from below to the thalamus. Behind the thalamus, the legs diverge and each part of the wall of the lower horn of the lateral ventricle passes into the fimbria of the hippocampus. The anterior sections pass into the columns of the fornix, immersing in the hypothalamus, and end on the mastoid body. Under the corpus callosum there is a white plate - the fornix, consisting of 2 strands, connected in the transverse part by the commissure of the fornix (commissura fornicis). The body of the vault, moving away from the corpus callosum, bends forward and continues into the column of the vault (columna fornicis). The lower part of each column approaches the end plate, then the columns of the arch extend to the lateral sides and downward and posteriorly, ending in the mastoid bodies.
Between the crura of the arch at the back and the term plate at the front there is an anterior commissure
(comissura anterior), which connects both hemispheres. The anterior part of the commissure connects the olfactory triangles, the posterior part connects the cortex of the temporal lobes.
Inner capsule
(capsula interna) is a curved plate of the white body, formed on the lateral side by the lentiform nucleus, and on the medial side by the head of the caudate nucleus (in front) and the thalamus (back). Consists of a front leg, a knee and a back leg. The internal capsule contains projection fibers that connect the cortex with other parts of the central nervous system. In the knee there are fibers of the corticonuclear tract, in the section of the posterior leg - the corticospinal tract, posteriorly - thalamo-parietal fibers, even more posteriorly the temporo-parieto-occipital-pontine fascicle, in the posterior part of the peduncle - the auditory and visual pathways. In the anterior leg there is the frontopontine tract, corona radiata. The corticonuclear pathway is the conscious control of the striated muscles of the face and neck.
Ticket 4
Anatomy and topography of the bridge. Parts, internal structure, position of nuclei, conducting pathways in the bridge.
Pontine, pons: ventral surface and dorsal surface (=upper half of the rhomboid fossa)
Below it is the medulla oblongata, above - the cerebral peduncles. The pons forms the largest middle cerebellar peduncle.
External structure: the basilar groove (sulcus basilaris), in which the artery of the same name lies, runs along the middle of the ventral surface. Dorsal surface (together with prod.m). forms a diamond-shaped fossa.
Internal structure: gray (nuclei of 5,6,7,8 cranial nerves and proper nuclei) and white matter (paths: descending: tractus corticospinalis, ascending from the prod.m. pass there: tractus spinothalamicus and tractus bulba)
A cross-section shows the trapezoidal body, which divides the bridge into a base (basis) and a tire (tegmentum).
At the base: the pons' own nuclei, their processes form the middle cerebellar peduncle; descending pathways from the cortex, which then form pyramids on the medulla oblongata + what is invisible: fibers of the reticular formation, medial and lateral loops
In the tegmentum: posterior longitudinal fasciculus (ascending tracts), nuclei of the CN nerves (5,6,7,8 pairs).
Functions: the bridge connects the overlying and underlying parts of the brain, together with the cerebellum it participates in the coordination of movements.
Ticket 5
Anatomy and topography of the olfactory brain; its central and peripheral sections.
The olfactory brain (rinencephalon) is phylogenetically the most ancient part of the forebrain.
It is part of the limbic system, which is responsible for emotions, homeostasis, long-term memory, and motivation.
The olfactory brain is divided into sections: central and peripheral.
1) Central: vaulted gyrus, hippocampus, dentate gyrus.
The vaulted gyrus is ring-shaped and goes around the corpus callosum on the medial surface of the hemispheres. Consists of the cingulate gyrus (the center of smell and regulation of the function of internal organs), the parahypocampal gyrus, and the isthmus between.
The dentate gyrus is rudimentary.
Hippocampus - club-shaped body in the cavity of the inferior horn
2) Peripheral: olfactory bulb, olfactory tract, olfactory triangle (relates to the olfactory nerve)
Ticket 6
Topography of the medulla oblongata. Position of nuclei and pathways in the medulla oblongata.
Medulla oblongata or bulbus. Cavity – 4th ventricle.
It is bordered above by the pons, below by the spinal cord, the border between the medulla oblongata and the spinal cord is considered to be the foramen magnum or the first pair of spinal nerves or the decussation of the pyramids. Forms the inferior cerebellar peduncle and the inferior triangle of the rhomboid fossa.
It has a ventral (front) and posterior surface.
On the anterior: the anterior median fissure (fissure mediana anterior) on the sides of which there are pyramids (fibers of the pyramidal tracts), on the side of the pyramids there is an olive, separated by the anterior lateral groove (in which the roots of the hypoglossal nerve emerge), dorsal to the olive, the roots of the glossopharyngeal nerve emerge from the posterior lateral groove, vagus and accessory nerves.
pyramids of the medulla oblongata, which form the tractus cortico spinalis (descending spinal tracts) and partially tend in opposite directions (form a cross of the pyramids; these fibers that formed the cross go to the lateral cords of the sp.m., and those that remained on their side - to the anterior cords sp.m.). Lateral to the pyramids lie olive trees, from which Tractus Oliva spinalis begins
The posterior surface is divided by a median groove, on either side of it there are thin and wedge-shaped cords; thin and wedge-shaped beam.
Internal structure: gray and white matter.
Gray: center of respiration and blood circulation, nuclei of the CN (9,10,11,12), reticular formation (belongs to the extrapyramidal system - unconscious, regulates the joint work of muscles, the path of the tractus reticulum spinalis begins), nucleus of the olive (equilibrium), from the olive - olive spinalis
White: short (for communication between nuclei within the prod.m.) and long fibers (ascending: the path of the skin and motor analyzer) and descending (pyramidal paths).
Functions: center of automaticity of the respiratory and cardiovascular systems, centers of unconditioned reflexes (digestive: saliva, swallowing, vomiting, protective: blinking, tears, sneezing). Since it forms the cerebellar peduncle, it takes part in the coordination of movements and balance.
Ticket 7
Anatomy and topography of the diencephalon, its sections, internal structure. Position of nuclei and pathways in the diencephalon
Diencephalon. Hidden from view because it lies under the cerebral hemispheres. Between the midbrain (which lies below and behind) and the telencephalon (which lies in front and above). Cavity – 3rd ventricle.
There are 2 parts: the thalamic brain (thalamus, epithalamus, metathalamus) and the hypothalamus.
Thalamic brain:
1) thalamus = visual thalamus (right and left). Anterior tubercle and pillow. Subcortical intermediate center of all types of sensitivity (from here impulses go to the cortex). Memorization.
Nuclei from the gray region (from 40 to 60, main: anterior, anterolateral, posterior, posterolateral, medial, redistribution of information from the sensory organs to the cortex)
2) epithalamus (epithalamus) - suprathalamic region: (epiphysis) pineal gland - produces serotonin, leashes, adhesions of leashes, triangles of leashes.
3) metathalamus (methatalamus) - post-thalamic region: medial and lateral geniculate bodies: subcortical centers of hearing and vision.
Hypothalamus - makes up the lower parts of the diencephalon, participates in the formation of the bottom of the 3rd ventricle: optic chiasm, optic tract, gray tubercle with the infundibulum and pituitary gland, mammillary bodies (subcortical olfactory centers).
more than 30 cores: regulation of body temperature, sleep and wakefulness, autonomic nervous system.
Its nerve cells are capable of producing neurosecretions: liberins and statins, which are transported through the processes of these cells to the pituitary gland, can inhibit or stimulate the production of its hormones, therefore the hypothalamus controls the activity of the human endocrine system.
Tumors of the 4th ventricle
Neoplasms of the 4th ventricle belong to tumors of the posterior cranial fossa. Up to a quarter of all subtentorial neoplasms are located in the cavity of the 4th ventricle.
The 4th ventricle is part of the ventricular system of the brain, into which cerebrospinal fluid enters through the cerebral aqueduct from the 3rd ventricle, and then flows into the base cisterns through the paired foramina of Luschka and the unpaired median foramen of Majendie. The choroid plexus of the 4th ventricle produces cerebrospinal fluid in small quantities.
The bottom of the 4th ventricle is the brain stem, namely the rhomboid fossa, which contains in a small area a high concentration of nuclear centers in combination with nerve conductors from the cerebral hemispheres to the spinal cord.
The roof of the 4th ventricle is the cerebellum, namely the superior and inferior cerebellar velum. The cerebellar peduncles are located on the sides.
A tumor of the 4th ventricle is a neoplasm that comes from its walls and is located in its cavity.
According to histological type, true tumors of the 4th ventricle include neoplasms of the choroid plexus and ependymomas; also neoplasms of the astrocytic series of varying degrees of malignancy, medulloblastomas growing from the brain stem and cerebellum, but located mainly in the ventricular cavity.
Clinical picture of the disease.
Clinical symptoms of tumors of the 4th ventricle consist of focal signs of damage to the brainstem, cerebellum and hydrocephalic-hypertensive syndrome.
Progressive tumor growth leads to closure of the lumen of the 4th ventricle and causes the development of occlusive hydrocephalus. Signs of intracranial hypertension are headache with nausea and vomiting. A specific symptom of tumors of the 4th ventricle is Bruns syndrome, which is characterized by a sharp attack of headache with nausea and vomiting, autonomic disorders (sweating, fear, palpitations), impaired consciousness that occurs when turning the head and torso. The cause of this symptom is a sharp disruption of the flow of cerebrospinal fluid due to obstruction of the cavity of the 4th ventricle and its openings by the tumor. During the non-attack period in children, it is often possible to identify a forced position of the head; the child sometimes, unnoticeably, begins to tilt his head back or to the side in order to facilitate the flow of cerebrospinal fluid.
If the tumor grows from the bottom of the rhomboid fossa or involves stem structures in the pathological process, a symptom complex of damage to various areas of the brain stem is observed. The child has impaired eye movement, strabismus, twitching of the eyeballs, asymmetry of the facial muscles, hearing impairment, weakness in the limbs, swallowing disorders, speech disorders, and impaired voice sonority. When a tumor affects the cerebellum, symptoms of balance and coordination problems develop. The gait becomes unsteady, trembling appears in the hands, and the accuracy of movements is impaired, which is especially noticeable when performing purposeful actions.
Diagnostics.
The methods of choice for suspected brain tumors, in particular a tumor of the 4th ventricle, are neuroimaging methods: CT, MRI, PET of the brain.
Computed (CT) and magnetic resonance imaging (MRI) clarify the location, size of the tumor, the initial growth of blastomatous tissue (subependymal layer, ventricular wall, choroid plexus), its structure (presence of cysts, calcifications, hemorrhages), relationship with stem structures, vascular collectors. The severity of hydrocephalus is assessed.
For the purpose of differential diagnosis with non-tumor space-occupying processes of the lateral ventricles, assessing the metabolism of the paraventricular medulla, and identifying the degree of malignancy of the tumor, patients undergo positron emission tomography (PET).
In the case of malignant neoplasms (medulloblastoma), to exclude metastasis along the cerebrospinal fluid pathways, patients undergo a tomographic examination of the spinal cord.
Treatment of tumors of the 4th ventricle is surgical. In most cases, a tumor of the 4th ventricle is accompanied by cerebral hydrocele, and therefore requires additional surgical correction in some cases. With severe hydrocephalus in young children, in some cases, even before tumor removal, surgery to eliminate hydrocephalus is required (endoscopic perforation of the floor of the 3rd ventricle or implantation of a cerebrospinal fluid drainage system). If hydrocephalus persists after total removal of the tumor, a liquor shunt operation is performed. Before performing CSF shunt interventions, it is necessary to conduct infusion-stress tests to select the parameters of the implanted shunt systems.
For malignant neoplasms, tumor removal should be combined with additional therapy, which, depending on age, includes radiation and/or chemotherapy. Among the methods of adjuvant therapy, our clinic also uses specific immunotherapy and photodynamic therapy.