Congenital defects, anomalies, defects in brain development
Numerous developmental defects in children arise due to disruption of intrauterine embryogenesis.
Congenital anomalies in the fetus and newborn child are detected immediately by the appearance of the skull or several years after the onset of neurological disorders. Depending on the location, migration disorders of cerebral tissue cause certain clinical symptoms. The acute course of the pathology will allow neurologists to make a diagnosis in a timely manner. Chronic development with cycles of exacerbations and remissions is not a specific sign of nosology.
Genetic diagnosis of central nervous system disorders at NEARMEDIC
In the genetic departments of the multidisciplinary medical network NEARMEDIC, effective genetic examination is carried out in preparation for conception and prenatal screening - during different periods of pregnancy, which makes it possible to accurately identify defects in the development of organs and systems of the fetus.
Indications for consultation with a geneticist are:
- cases of malformations and stillbirths in the couple or in the birth history;
- the presence of relatives suffering from degenerative diseases of the central nervous system;
- the age of the expectant mother is over 35 years;
- close relationship of the couple;
- viral infections suffered before conception or in early pregnancy (toxoplasmosis, rubella, hepatitis B and C, etc.);
- unregulated ionizing radiation of either spouse before conception.
Central and regional genetic departments and laboratories of the network provide patients with a full cycle of hardware examination and laboratory molecular genetic research.
Brain dysplasia - what is it?
Limited cerebral damage in a limited area provokes a variety of clinical manifestations. Epileptic seizures are combined with impaired consciousness and cortical disorders.
Initial signs of nosology using electroencephalography. Minor cerebral changes can be treated with anticonvulsants.
Types of focal dysplasia:
- The first type is a local change in cortical architectonics;
- The second type is focal cytoarchitectonic changes;
- The third type is pathology of architectonics in secondary diseases (temporal sclerosis, cerebral malformation, Rasmussen's encephalitis, ischemia).
Methods of radiation neuroimaging MRI of the brain in St. Petersburg help verify the stage of nosology.
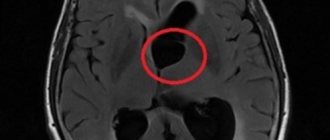
Polycystic dysplasia of the brain is characterized by the presence of many cystic growths within the cerebral tissue.
To diagnose defects, the results of CT and MRI are compared
Exogenous factor
The most influential cause of brain malformations is considered to be an exogenous factor. Many chemical compounds, along with radioactive contamination and certain biological factors, have teratogenic properties. An important role is played by the problem of environmental pollution, in which toxic chemicals enter the body of pregnant women. In addition, embryotoxic effects may be associated with the lifestyle of a pregnant woman, for example, alcoholism, smoking or drug addiction.
Anomalies of brain stem development - causes
Depending on the morphological changes, groups of brain abnormalities are distinguished:
- Regulations;
- Quantities;
- Size and shape;
- Structures (buildings).
The first group of nosologies arises due to underdevelopment of the rudiment of the cerebral structure or the complete absence of the embryonic rudiment. If the baby is born normal, the prognosis is poor due to the absence of part of the brain.
Positional anomalies include the doubling of an organ, the merging of several parts together at the same time.
Defects in the position of cerebral structures
All nosological forms of the group are determined by three factors:
- Inversion displacement of the organ relative to its own axis, median position;
- Dystopia is an unusual localization of embryonic structures;
- Heterotopia is a pathology of organ anlage.
The degree of displacement is determined by the severity of clinical symptoms and a person’s life expectancy.
Defects in brain size and shape
The list of nosologies in this category is determined by a number of morphological changes:
- Synostosis of several organs;
- Hyperplasia - an increase in the number of tissues and sizes of cerebral tissues;
- Dysplastic hypoplasia – reduction in the size of the structure;
- Simple hypoplasia - no changes in morphology.
Defects in brain structure
The nosology is accompanied by anomalies in the natural formation of the hole and morphological features of the structure. Heteroplasia develops at the stage of intrauterine development. Characterized by atypical tissue formation.
Dysplasia is a pathology of the relationship of articular surfaces.
Hamartria is the abnormal development of tissue structures. Stenotic narrowing of the canal or duct can be congenital or acquired.
A dysontogenetic cyst is accompanied by a significant narrowing of the compensatory capabilities of the organ.
Classification of embryonic developmental defects:
- Fetopathies;
- Embryopathies;
- Blastopathy;
- Gametopathies.
Depending on the time of occurrence of defects in embryonic development, a certain type of disorder occurs.
Based on the extent of damage, the following types of cerebral defects are distinguished:
- Multiple – affects several brain areas at once;
- Systemic – localized within one area;
- Isolated - cause damage to one organ.
Congenital anomalies of the central nervous system can be provoked by infectious agents:
- Toxoplasma;
- Cytomegalovirus;
- Coxsackie virus.
Alcohol abnormalities occur if a pregnant woman drank alcohol during pregnancy. The pathology is provoked by chromosomal aberrations and genetic mutations during the formation of the neural tube (third or fourth week of pregnancy).
Causes of vices
Failure can occur at different stages of brain formation. If malformations of the brain (ICD 10 - Q04) occur in the first six months of pregnancy, they can lead to a decrease in the number of formed neurons, and, in addition, to certain disturbances in the differentiation of departments. In later stages, damage and death of the cerebral substance is possible. The most significant reasons for such a failure are the effects on the fetus and the pregnant woman’s body of various harmful factors that have a teratogenic effect. The occurrence of defects against the background of monogenic inheritance occurs only in one percent of cases.
Main types of brain defects
Defects in shape, size, and location of individual anatomical structures are identified. Let's consider the main types of congenital anomalies of brain development.
What is encephalocele
Penetration of cerebral tissue through skull defects causes various neurological symptoms, depending on the characteristics of the site of prolapse. Mild anencephaly resembles a cephalohematoma, but skull radiography reveals midline cleft and asymmetrical areas.
With the help of surgical intervention, it is possible to eliminate the pathology, but large lesions cannot be eliminated by ectopic protrusion. Encephalocele is verified by radiation neuroimaging methods - MRI and CT.
Features of anencephaly
The pathology is characterized by the absence of individual bones of the skull. The sites of destruction are overgrown with connective tissue, which does not allow optimal regulation of intracranial pressure.
Most nosological forms are incompatible with life. Death occurs immediately after birth, when the lungs open and the supply of oxygen to the cerebral parenchyma begins.
Manifestations of microcephaly
Underdevelopment of cerebral tissue occurs in one child out of five thousand newborns. The nosology is determined by a decrease in the size of the cranium, a violation of the relationship between the brain and the facial part of the skull.
Microcephaly (Giacomini syndrome) develops in utero in women with infections and parasitic diseases.
Causes of primary microcephaly:
- Genetic abnormalities with autosomal recessive transmission;
- Toxoplasmosis, cytomegalovirus encephalitis, rubella.
Etiological factors of secondary microcephaly:
- Cerebral cysts;
- Calcifications and hemorrhages inside the brain parenchyma.
A decrease in the size of the skull is characterized by about ten percent of oligophrenia. From an early age, the child exhibits developmental delays and closed developmental defects. Mental retardation is accompanied by convulsive syndrome. Muscle twitching is accompanied by improper development of the brain part of the skull.
What is macrocephaly characterized by?
Enlargement of the cranium allows diagnosing pathology. The nosology is characterized by hypertrophy of one hemisphere, disproportionate development of one half. Mental retardation is the most common manifestation. Seizures occur in approximately nine to ten percent of patients.
The clinic of nosology appears during the first years of life, which allows timely verification of pathology. Brain migration disorders are too severe for effective treatment of the disease.
Symptoms of holoprosencephaly
Holoprosencephaly is a disease accompanied by a defect in the development of the hemispheres. The lack of separation between the cerebral halves causes changes in the activity of functional centers.
Severe dysplasia leads to ventricular anomalies, asymmetry of the facial and brain parts. Severe defects lead to necrosis of the cerebral parenchyma with a high probability of death in the first days after the birth of the child.
The formation of a single hemisphere is a congenital defect due to a genetic abnormality of the thirteenth to fifteenth chromosomes. Nosology is often combined with other developmental defects:
- Cyclopia;
- Ethmocephaly;
- Cebocephaly.
The disease is accompanied by stillbirth. The ability to survive is minimal. The prognosis is unfavorable.
Clinic of cerebral cystic dysplasia
Multiple cystic cavities cause migration disorders. Developmental defects are accompanied by abnormalities in the distribution of cerebrospinal fluid. Numerous cysts cannot be removed. Often provoke muscle cramps. Low effectiveness of anticonvulsant treatment leads to progression of symptoms.
Single cysts may not pose a danger. Subclinical symptoms may occur due to increased intracranial hypertension.
How does agyria manifest itself?
Lissencephaly is a defect in the formation of the architectonics of the cerebral cortex. Severe convulsions are caused by underdevelopment of the cerebral convolutions. Nosology shapes motor and mental manifestations. Neurological signs of the disease – Lennox-Gastaut syndrome, Vesta.
The coherence of the brain provokes paralysis, paresis, and polymorphic convulsions. Signs of nosology develop in the first year of life. The baby lives for approximately this period of time.
Clinical signs of pachygyria
The developmental defect is due to the lack of formation of the secondary and tertiary gyri. Straightening the grooves of the second type disrupts the cerebral architecture.
The pathology of the layered structure of the cortex is characterized by heterotopia of nerve cells. MRI shows pachygyria well.
Clinical symptoms of craniostenosis
The disease is characterized by a narrowing of the skull with compression of the brain between the bones. Depending on the progression, decompensated and compensated variants of the nosology are distinguished.
According to the characteristics of the course, stable and progressive forms of the disease are distinguished. More often, the causes are due to early healing of the coronal or sagittal sutures. Pathology without timely treatment leads to death, as brain infringement occurs. Clinical symptoms depend on the predominant localization of the zone of compression of the white matter and parenchyma.
Neurological symptoms are characterized by numerous disorders against the background of increased intracranial pressure.
A child with craniostenosis has a severe headache, so the baby is restless, irritable, and whiny. Memory loss and impaired concentration occur when the condition persists for a long time. The prognosis of the pathology is unfavorable.
Indicators of agenesis of the corpus callosum
Nosology is characterized by underdevelopment of the corpus callosum. Concomitant pathology is underdevelopment of the third ventricle of the brain. Hypoplasia provokes underdevelopment of muscle muscles, paresis and paralysis, muscle cramps.
Manifestations of Aicardi syndrome occur when underdevelopment of the corpus callosum is combined with chorioretinal defects. The clinical picture is complemented by myoclonic convulsions, the formation of numerous lacunar nodes in the retina and optic nerve head. The nosology is characterized by microphthalmia, pendulum-like eye movements.
Some researchers have identified X chromosome defects in men in patients with agenesis of the corpus callosum.
Micropolygyria Clinic
The disease occurs due to the formation of numerous small convolutions. The normal cerebral cortex has six layers. With an anomaly, four layers can be traced. The abnormal structure leads to clinical symptoms:
- Swallowing disorder;
- Pathology of masticatory and facial muscles;
- Oligophrenia;
- Facial paraplegia.
The onset of the disease is observed in the first year of life.
Clinical manifestations of heterotopia
The nosology arises from neuronal migration. The lack of nerve signal transmission occurs due to heterotopions - pathological accumulations in the form of a ribbon or nodular form.
Due to heterotopia, mental retardation, epileptic syndrome, and various muscle cramps appear.
Description of the disease
Brain malformations are anomalies that consist of a pathological change in the anatomical structure of the cerebral structure. The severity of neurological symptoms that accompany cerebral abnormalities varies. In severe cases, such defects cause fetal death and account for up to seventy-five percent of intrauterine deaths.
In addition, severe congenital malformations of the brain (ICD 10 - Q04) cause about thirty percent of deaths of newborns. The timing of manifestation of clinical symptoms varies. In most situations, cerebral abnormalities manifest themselves in the first months immediately after the birth of the child. But, given that the formation of the brain continues until the age of eight, a number of defects make their clinical debut after the first year of life.
So, let's move on to consider the causes and find out exactly what factors influence the appearance of the disease.
Diagnosis of congenital brain defects
Most nosological forms are detected initially by clinical manifestations. Mild course, hypotonic muscle contractions provoke convulsive syndrome in children of the first year of life.
Instrumental diagnostic methods - ultrasound, neurosonography, MRI and CT - can exclude hypoxic and traumatological manifestations. The procedures are sufficient to identify developmental anomalies, cysts, and heterotopic areas.
Electroencephalography detects areas of increased cerebral activity in the presence of convulsive muscle twitches. Congenital species require genetic diagnostics to study DNA and determine mutations of the chromosomal apparatus.
Treatment
So, can brain developmental defects in children be treated or not?
Treatment of the pathology is predominantly symptomatic. It is carried out by a pediatric neurologist, neonatologist, pediatrician and epileptologist. If a convulsive syndrome is detected, anticonvulsant therapy is carried out using medications in the form of Carbamazepine, Levetiracetam, Valproate, Nitrazepam, Lamotrigine, and so on. Considering that epilepsy in children, which accompanies brain defects, is usually resistant to anticonvulsant treatment, a combination of two drugs at once is often prescribed, for example, Levetiracetam with Lamotrigine.
For hydrocephalus, dehydration treatment is carried out; according to indications, doctors often also resort to shunt surgery. In order to improve the metabolism of properly functioning brain tissue, to some extent compensating for existing birth defects, it is permissible to conduct a course of neurometabolic therapy with the prescription of B vitamins. Nootropic medications are used in treatment only in the absence of episyndrome.
For moderate and relatively mild cerebral anomalies, neuropsychological correction is recommended along with the child’s studies with a psychologist and comprehensive psychological support for the child. Additionally, children's art therapy is prescribed. Older children should be sent to specialized schools. These methods make it possible to instill self-care skills in sick children, thereby reducing the severity of mental retardation. Thanks to these techniques, it is possible to socially adapt children suffering from cerebral defects.
The prognosis for malformations of the brain in children is determined, as a rule, by the severity of cerebral anomalies. Unfavorable symptoms include early onset of epilepsy along with its resistance to treatment. The prognosis is further complicated by the presence of congenital somatic pathologies.
Second type of ancestral anomalies
The next type of anomalies includes those associated with the preservation of the embryonic structure. These include:
- Presence of persistence of the ductus botallus. This duct acts during embryogenesis, directing blood into the aorta from collapsed organs. Immediately after birth, it usually heals within ten weeks. If it remains in adults, it very often leads to heart failure. Among other things, such patients may develop blood congestion in the lungs, and, in addition, there may be an increase in pressure in the pulmonary circulation, which again will lead to heart failure.
- Abnormalities of the left or right aortic arch. With this defect, one of the arches, leaving the heart, captures the esophagus and trachea on the right, and the other runs on the left, after which they come together into the azygos aorta. As a result of such pathological fusion, the esophagus and trachea end up in a kind of ring (hence this defect acquired the name aortic ring). As a person ages, the aortic annulus shrinks, leading to difficulty swallowing.
- Pathology of the right aortic arch. In the presence of this anomaly, the aortic arch leaves the left ventricle, bending to the right, which causes dysfunction in neighboring organs.
- The presence of two hollow superior veins. If they flow into the area of the right atrium, then such an anomaly does not manifest itself clinically, but if it flows into the left atrium, then this can lead to the release of venous blood into the systemic circulation area.
- The presence of ribs that connect to the cervical region of the spine.
- Presence of lateral fistulas of the neck.
- Presence of a homodont dental system. All teeth are identical and have a conical shape; the incisors, as a rule, are not differentiated, as for example in sharks.
- The presence of supernumerary teeth in a row, and sometimes on the hard palate, as happens in amphibians.
- The presence of persistence of the cloaca, against the background of which the genital tract is combined with the rectum. Under conditions of normal development, immediately after the eighth week of the embryogenesis process, the cloaca can completely differentiate into the urinary ducts or rectum.
Third type of ancestral anomalies
Atavistic defects may be associated with a failure in the movement of organs during embryogenesis; because of this, they are located in those areas of the body in which, under normal conditions, they were localized in ancestral forms.
As part of the anomaly, a pelvic position of the kidney may be observed, which is associated with a violation of the movement of this organ during the second month of embryonic development from the pelvic area to the lumbar sector.
Presence of cervical ectopia of the heart. The area of origin and location of the heart in the phylogenetic series in vertebrates, as a rule, should be completely recapitulated in mammals, just like in humans. The heart is usually laid on the twentieth day of the embryogenesis process, first behind the head, and later moves to the mediastinum. In the presence of cervical ectopia, the heart may be delayed in the area of the initial anlage, against the background of which the child dies immediately after birth.