MRI for asymmetry of the lateral ventricles
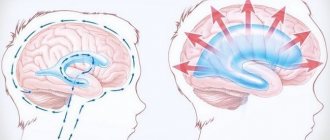
The ventricles of the brain are designed to regulate the pressure of cerebrospinal fluid (CSF) inside the brain. Tanks have a certain space that can increase in size.
The largest are the lateral ventricles. Through the interventricular foramina the cavities are connected to the third ventricle. Anatomical connections ensure the flow of cerebrospinal fluid when intracerebral pressure changes.
The fourth ventricle is located between the medulla oblongata and the cerebellum. This anatomical formation has a diamond shape.
In a healthy person, a constant relationship between the described structures is ensured. Blockage of one of the ventricles leads to an increase in the amount of cerebrospinal fluid with a subsequent increase in pressure. MRI detects ventricular asymmetry early, before clinical symptoms occur. Without signs, it is difficult to determine indications for referral to magnetic resonance therapy. MRI of the brain clearly shows ventricular asymmetry.
MRI asymmetry of the lateral ventricles
Causes of enlargement of the cerebral ventricles
Throughout life, there is a gradual increase in the spaces containing cerebrospinal fluid. Some pathological conditions lead to compression of the ventricular structures:
- Hydrocephalus - accumulation of fluid inside the brain with the development of dropsy;
- Birth injury;
- Long-term inflammation of the meninges with the formation of adhesions;
- Hemorrhagic hemorrhages;
- Strokes, hemorrhages.
There is a fundamental difference between the concepts of asymmetry and ventricular dilatation. The second nosology is an independent disease. It is formed under the influence of intrauterine infections and acquired pathology. Asymmetry is caused by additional cerebral formations (tumors, limited accumulation of blood). Immediately after birth, the condition is detected by ultrasound through open fontanelles. After healing of the cranial sutures, soft tissue components are shown by MRI.
The clinical picture of the asymmetrical arrangement of cerebral structures depends on the location and degree of compression. Small imbalances in the accumulation of cerebrospinal fluid are compensated by the reverse absorption of cerebrospinal fluid.
The cause of dilation may be overproduction of cerebrospinal fluid. In most cases, the etiological factor of the nosology is a violation of oxygen supply (hypoxia). The condition provokes increased formation of cerebrospinal fluid in order to improve the supply of nutrients and vitamins to the brain formations.
Treatment
The increased size of the lateral ventricles themselves does not require therapy. Treatment is prescribed in the presence of clinical symptoms . It is aimed at the underlying disease that led to the formation of dilatation, and at eliminating signs of impaired liquor dynamics. For this purpose use:
- diuretics;
- neuroprotectors;
- vasoactive agents;
- nootropics;
- sedatives;
- anti-inflammatory drugs;
- antibacterial therapy (if necessary).
Brain tumors and severe hydrocephalus require neurosurgical intervention with decompression of the cerebrospinal fluid tract. In severe cases, with rapid progression of the condition and no results from basic treatment, they resort to endoscopic ventriculostomy, a high-tech minimally invasive operation. Its essence comes down to the formation of a new connection of the ventricular system, bypassing the obstruction.
In the absence of clinical manifestations of dilatation of the ventricular cavities, treatment is not prescribed.
Enlargement of the lateral ventricles of the brain is a fairly common occurrence in childhood. Lack of timely and competent treatment can lead to the persistence of ventriculoasymmetry in the future. In most cases, such conditions are compensated and do not require treatment. However, an increase in the size of the ventricular cavities can be a consequence of traumatic brain injury, neuroinfections, and cancer. Such a situation requires mandatory supervision.
Symptoms of dilatation of the lateral ventricles
In an adult, clinical symptoms are rarely observed. Symptoms of dilatation in children:
- Dizziness;
- Nausea and vomiting;
- Apathy;
- Feeling of constant anxiety;
- Impaired walking coordination.
The clinical picture is nonspecific, so manifestations vary from person to person. In more rare cases, pathology of sensitivity, muscle paresis, cognitive disorders, and problems with head tilt occur.
Manifestations in newborns
The clinical picture in newborns is determined by the severity of the pathology. Immediately after birth, a number of external signs are noted:
- Frequent regurgitation;
- Tendency to throw the head back;
- Low muscle tone;
- Tremor;
- Paralysis;
- Nervous excitability;
- Decreased peripheral sensitivity;
- Constant crying;
- Refusal to eat.
Identification of any symptom requires an ultrasound scan of the brain. Ultrasound rays penetrate well through unclosed fontanelles.
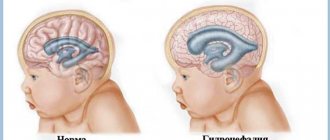
Hydrocephalus in a baby is determined by the appearance of the skull. The increase in head size is caused by excess accumulation of cerebrospinal fluid. Liquor causes dilatation (expansion) of the ventricles (lateral, third, fourth).
A high frequency of pathology formation is observed with cysts, intracranial hemorrhages, hematomas, and neoplasms.
Inflammatory processes in the cerebral parenchyma provoke bacterial and viral infections that newborns contract in utero (syphilis, chlamydia, mycoplasma, cytomegalovirus, herpes).
Diagnostics
Symptoms of the pathology do not provide reliable information about ventricular asymmetry, so objective studies are used to make a diagnosis.
- Monthly measurement of baby's head growth. This procedure is carried out by a local pediatrician. The essence of the method is to measure the size of the head. The indicators indicate normal growth, or excessive growth, which indicates a violation of the formation of the GM due to the expansion of the ventricles.
- Magnetic resonance or computed tomography. These neuroimaging methods allow the structure of the brain to be assessed using layer-by-layer images. The data indicate the volume and dynamics of changes in the volume of the lateral ventricles.
- Ultrasound. The method shows volumetric changes in structures, changes in the ratio of the ventricles, the presence of cysts and neoplasms.
- Echoencephaloscopy is an ultrasound method that allows you to assess the presence of volumetric structures (tumors). This procedure provides indirect evidence of changes in ventricular symmetry.
- Cerebrospinal fluid puncture. One of its parameters (the pressure under which cerebrospinal fluid flows out) can indicate a reduction in cavities. If the pressure is high, the ventricle is reduced, if the pressure is low, its size is increased. The remaining parameters (pH, glucose level, color and density) do not matter.
What is the MRI normal for the lateral ventricles in an adult?
The dimensions depend on the cause of the pathology. An asymmetrical arrangement of cerebral structures is observed in neoplasms, intracranial hypertension, and hydrocephalus. Some differences in the measured values depend on the type of examination - native or contrast magnetic resonance imaging.
Tomographic indicators of the cerebral ventricles
MRI of the head shows the lateral ventricles as anechoic zones (density below surrounding structures). Three-dimensional modeling allows us to distinguish the anatomical structures of the lesion:
- Triangle (atrium);
- Body;
- inferior temporal horn;
- Occipital (back) part;
- Frontal (front) zone
The size of the ventricular spaces increases with age. In the gestational period, the value is several tenths of a millimeter. In a mature child, the ventricular spaces are slit-like. MRI determines the width of the space in the area of the foramen of Monroe, where the norm is 2 mm.
The expansion in adults begins posteriorly, so any examination requires clear visualization of the occipital structures.
Pathological dilatation is diagnosed when the diameter of the anterior horns, determined on coronal sections, increases over five millimeters.
Magnetic resonance scanning can accurately determine when the lateral ventricles are dilated and when disposition occurs.
Provoking diseases
The main disease causing this pathology is hydrocephalus. It can interfere with the absorption of cerebrospinal fluid. This leads to its accumulation in the lateral ventricles.
Excessive formation of cerebrospinal fluid is also observed with serious lesions of the central nervous system. Poor circulation is also associated with the formation of cysts, tumors and other neoplasms.
A common cause of hydrocephalus is a defect of the Sylvian aqueduct. If this defect was discovered during the prenatal period, termination of pregnancy is recommended. At the birth of a child, complex systematic treatment will be required.
Another cause is aneurysm of the vein of Galev and Arnold-Chiari syndrome. However, in children, the disease can be caused by rickets or due to the specific structure of the skull, so observation by a specialist is important if there is a predisposition to the disease.
Material and research methods
A study of patients with paroxysmal schizophrenia was conducted using MRI using the vascular mode. All patients underwent inpatient treatment at the Mental Health Clinic in 2009–2011. Clinical diagnosis of schizophrenia was carried out according to the criteria of the taxonomy of mental disorders adopted by the National Center for Mental Health of the Russian Academy of Medical Sciences and according to ICD-10. Of the 62 patients examined, 30 (1st group) had an attack-like-progressive (fur-like) form of the disease (F20.01, F20.02) with a stable or increasing defect and the persistence of residual hallucinatory-delusional disorders in remission.
In 32 patients (group 2), a recurrent (F20.03) form with remissions without residual psychotic symptoms and deficit disorders was identified. The age of the patients varied from 18 to 58 years, with the majority of patients aged from 18 to 39 years (57 people). The average duration of the disease from the moment of its manifest manifestations in most cases (47) did not exceed 9 years and in the 1st and 2nd groups of patients was 8.9 years and 4.9 years, respectively. 18 patients were admitted to a psychiatric hospital for the first time and practically did not take psychotropic drugs. 33 people took psychotropic drugs irregularly during interictal periods, and refused to take them before admission to the hospital. Syndromic psychopathological assessment of the condition of patients of groups 1 and 2 at the time of examination is reflected in Table. 1. None of the studied patients had severe somatic diseases, organic diseases of the central nervous system, or alcohol and drug addiction.
Table 1. Characteristics of the examined sample of patients with schizophrenia.
| Forms of schizophrenia | fur-like | recurrent | Total | ||
| Number of patients examined | 30 | 32 | 62 | ||
| Gender distribution | m | 15 | 14 | 29 | |
| and | 15 | 18 | 33 | ||
| Age range at the time of examination | 18-58 | 18-51 | 18 — 58 | ||
| Average age at the time of examination | 31,5 ± 9 | 29,6 ± 8,85 | 30,5 ± 9,3 | ||
| Average duration of illness | 8,9 | 4,9 ± 5 | 7 ± 7,7 | ||
| Leading syndrome | Catatonic-paranoid | 8 | 2 | 10 | |
| Hallucinatory-delusional | 15 | 3 | 18 | ||
| Affectively delusional | 7 | 26 | 33 | ||
The severity of the condition in the studied groups of patients with schizophrenia practically did not differ. In both forms, patients were hospitalized due to a rapid increase in psychotic symptoms, reaching a similar degree of severity (the average value on the Brief Psychiatric Scale BPRS for the paroxysmal-progressive form was 40.5 ± 6.8 points, and for the recurrent form – 40.7 ± 6, 3 points). Intergroup differences were noted only in the syndromic structure of psychosis: in the paroxysmal-progressive form, catatonic-paranoid and hallucinatory disorders had a greater share than in the recurrent form, with similar severity of affective disorders (Table 1).
The MRI examination was carried out on a 1.5T tomograph from Siemens (Germany) using the vascular mode without contrast. The tomograms were evaluated by an experienced neuroradiologist. The frequency of abnormalities in the condition of the cerebral ventricles (lateral, 3rd), subarachnoid spaces, fissures, as well as the condition of perivascular spaces, venous sinuses, including sigmoid and transverse sinuses, disorders of venous circulation in general, and anomalies in the structure of arteries was calculated. The significance of intergroup differences was calculated by Fisher's angular transformation. The intergroup difference was considered significant when the calculated Phi value was more than 1.64.