Discussion
The high sensitivity of germinomas to radiation and chemotherapy limits the surgery of these deep-seated tumors to obtaining biopsy material and operations aimed at eliminating intracranial hypertension.
With timely diagnosis and early treatment, preoperative symptoms may partially or completely regress. This makes early diagnosis of germinomas important. With the “habitual” localization of the tumor in the pineal and suprasellar region, this, as a rule, does not present any difficulty. Germinomas of the subcortical ganglia are rare, so when the tumor is localized in this area, the histological diagnosis is often unexpected.
Typical manifestations of tumors of the subcortical region, including germinomas, are symptoms of damage to the internal capsule and subcortical nuclei (hemiparesis, extrapyramidal syndrome). In all our observations, hemiparesis of varying severity and extrapyramidal symptoms were detected. Moreover, despite the persistent remission of the disease during treatment, the hemiparesis regressed only partially or did not regress at all. This is due to the infiltrative growth of germinomas, often late diagnosis of the disease and late initiation of therapy. In one of our observations, hemiparesis in the initial stage of the disease was transient, which caused a delay in stereotactic biopsy and a further increase in symptoms.
Diabetes insipidus is often the first and only symptom of the disease in germinomas of the suprasellar region, and in some cases it appears before the tumor is visualized on MRI [11, 12]. In our observations, diabetes insipidus in observation 1 was diagnosed 2 years before the onset of hemiparesis, in observation 2 it developed 8 months after the onset of muscle weakness in the extremities, and in observations 3 and 4 it was absent. The presence of diabetes insipidus and loss of other pituitary functions in the first two cases suggested germinoma, despite the uncharacteristic location of the tumor.
The literature describes cases of disease manifestation in the form of pathological hiccups and vomiting without hydrocephalus [10]. The cause of these symptoms is difficult to explain. Perhaps they are caused by hidden dissemination of the tumor into the medulla oblongata.
The disease also often manifests itself as mental disorders [13, 14]. Three of our patients had psychopathological symptoms in the form of disinhibition, foolishness, decreased criticism, and euphoria. This symptomatology is probably due to damage to the nuclei of the thalamus and their connections with the frontal lobes.
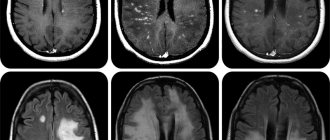
According to the literature, germinomas of the subcortical ganglia are distinguished by a variety of MRI manifestations [8, 9, 14, 15]. Ji Hoon Phi et al. Based on 17 observations and literature data, 4 types of MR patterns of growth of germinomas of the subcortical nodes were identified - from small areas of signal change in the projection of the subcortical nodes that do not accumulate contrast agent, which are often interpreted as a non-tumor lesion (stroke, demyelination), to large space-occupying formations with intense accumulation of contrast and pronounced mass effect [10]. Our observations fully confirm these data. There are also cases of multifocal germinoma lesions involving the subcortical ganglia and other areas of the brain [9, 16–18]. Such a case occurred in one of our observations. Bilateral tumor growth may indicate ependymal spread of germinoma to the opposite side, and may help in the differential diagnosis with glial tumors.
Germinomas of the subcortical ganglia are also characterized by atrophic changes in the brain at the site of the lesion, according to MRI data [15, 19, 20]. In this regard, it should be noted that in one of our observations on a series of repeated MRIs of the brain, a dynamic decrease in the volume of formation of the subcortical nodes was noted, followed by a significant increase. The reason for this phenomenon is unclear, since the patient did not receive hormonal therapy, which could help reduce swelling and partial regression of neurological symptoms. We did not find similar observations in the literature.
Due to the variety of neuroradiological manifestations of subcortical ganglion germinomas, a study of tumor metabolism using C11-methionine PET can provide some assistance in differential diagnosis [7, 10, 21, 22].
Surgical treatment for germinomas of the subcortical ganglia is limited to stereotactic biopsy. In two of our observations, direct neurosurgical intervention was performed due to the severe condition of the patients, caused by a pronounced mass effect and occlusion of the cerebrospinal fluid ducts. In observation 3, removal of a tumor node on the right led to the patient’s left-sided hemiparesis worsening, while the hemiparesis on the right significantly regressed during chemotherapy. In observation 4, regression of hemiparesis was noted in the postoperative period.
There are isolated publications concerning long-term results of treatment of basal ganglia germinomas [9, 10].
According to the data presented in them, patient survival is slightly lower than with germinomas located in the midline. Ji Hoon Phi in 2010 in a series of 17 patients reported 66% disease-free survival and 77% overall survival [10]. Y. Sonoda (2008) in a group of 10 patients noted 3 tumor relapses and 1 death [9]. A possible reason for the unfavorable outcome is the late diagnosis of germinomas of the subcortical ganglia, when the disease takes on a disseminated form, spreading throughout the ependyma of the ventricles and subarachnoid spaces of the central nervous system. Also, the cause of relapses may be an incomplete volume of radiation therapy, which in these cases must necessarily cover the entire ventricular system [10, 17, 23, 24].
Features of the structure and function of the cerebral cortex
The cerebral cortex is divided into: ancient, old and new cortex. The ancient and old cortex combines with some nearby nuclei to form the limbic system. The thickness of the new cortex is 3 mm, includes many convolutions, the area of the new cortex is 2500 cm2, 3 types of structures of the cerebral cortex: nerve cells, processes of nerve cells, neuroglia.
The cerebral cortex contains neurons of different structures - stellate, large and small pyramidal, fusiform, basket-shaped and others.
Functionally, all neurons are divided into:
- afferent (stellate cells) - impulses from specific pathways go to them and specific sensations arise. They transmit impulses to intercalary and efferent neurons. A group of polysensory neurons - receives impulses from the associative nuclei of the visual thalamus;
- efferent neurons (large pyramidal cells) - impulses from them go to the periphery and provide a certain type of activity;
- intercalary neurons (small pyramidal, fusiform and others). Interneurons can be excitatory or inhibitory (large and small basket neurons, neurons with brush-shaped axons, candelabra-shaped neurons).
Functions of nerve cell processes:
- provide communication within the cerebral cortex between the above and underlying cells;
- provide communication within one hemisphere of the cerebral cortex;
- commissural - leave the cerebral cortex, pass through the commissure and go to the cerebral cortex of the opposite hemisphere;
- leave the cerebral cortex and go in a descending direction, forming pyramidal and extrapyramidal tracts.
Neurons and processes in the cerebral cortex are located in 6 layers. Neurons performing the same reflex function are located strictly above each other. Thus, the structural unit of the cerebral cortex are individual columns. The most pronounced connection is between layers 3, 4, 5 of the cerebral cortex.
Proof of the presence of columns: when microelectrodes are introduced into the cortex, an impulse is recorded strictly perpendicularly when exposed to the same reflex reaction. If the electrodes are inserted in a horizontal direction, impulses characteristic of various reflex reactions are recorded. Column diameter is 500 µm. Neighboring columns are closely related functionally and are often in reciprocal relationships with each other (some excite, others inhibit). When a stimulus acts, many columns are involved in the response, a perfect analysis and synthesis of stimuli occurs - the principle of screening (when a strictly certain number of receptors in the cerebral cortex are stimulated, a significant area is involved in the response).
The cerebral cortex is the highest manager and distributor of the functions of the animal and human body (I. P. Pavlov).
Functions of the cerebral cortex:
- perfects the relationship between organs and tissues within the body;
- ensures complex relationships between the body and the external environment;
- provides processes of thinking and consciousness;
- is a substrate of higher nervous activity.
conclusions
Germinomas of the subcortical ganglia are a very rare pathology. Based on our experience and publications, subcortical ganglion germinomas are often diagnosed at a late stage, due to atypical clinical symptoms and a variety of neuroimaging manifestations. The manifestation of the disease in boys in the second decade of life can help in diagnosis: bilateral damage to the subcortical nodes according to MRI; neuroendocrine symptoms that occur in some of these patients, despite the absence of MRI signs of damage to the suprasellar region; psychopathological symptoms that are present in these patients and are not pathognomonic for glial tumors of the subcortical ganglia.
There is no conflict of interest.
PRACTIK
For the emotional brain, safety is doing today what you did yesterday, and tomorrow what you did today. Cooperating with the reptilian brain, it transfers the lessons of the past to the “now” moment and does not think about the future. In other words, it connects all the memories as if the events were happening in the present time, and then you experience the feelings and emotions from past experiences.
The “gravity” of the emotional brain, in its desire to preserve what we already have, manifests itself in resistance to change, it holds and pulls us back into the so-called “comfort zone” - the status quo, as part of homeostasis. Any of our attempts to get out of it is stressful for the emotional brain. Remember this concept - “comfort zone”, it is extremely important for understanding our behavior when we decide to change.
We can say that this is our “caring parent” and “protective parent.” He likes things that are familiar to you: “mom’s porridge”, everything that has made you happy since childhood, familiar surroundings, behavior and atmosphere.
Every decision you make goes through his filter: “Is this good for me? Is it safe for my family? Isn’t there a threat in this?” And if something threatens, you reject this choice. In other words, when the emotional brain makes decisions, it bases it on what is close and familiar to you. When you feel resistance to change, it means your emotional brain is controlling your mind. It is he who whispers to you: “the hat doesn’t suit Senka” or “we didn’t live richly, there’s nothing to start with.” Its features: - lives in the present time; — auditory (communication using sounds and tones); - orientation towards life in a group, his priority is the survival of the group, family, clan; - does not know the options, only “yes” and “no”, “good and bad”, “this or that”; - associativity with certain moments of life - when we think about something, we enter into an image and experience feelings.
The emotional brain does not distinguish between threats to our body and threats to our ego. Therefore, we begin to defend ourselves without even understanding the essence of the situation. When someone hurts our feelings, it releases adrenaline, stimulates blood flow to the large muscles, instantly focusing our thoughts to protect ourselves from the threat.
It is important to know that before any transformation processes begin to occur in you, the emotional brain must understand that the entire group, family or clan will be safe. His thinking is designed in such a way that he will always look for manifestations of similarity. For example, when communicating with new people, he will feel the safety of the “comfort zone” when he is convinced that the new person is similar to you. This is the fulfillment of his “friend or foe” function. Convincing him of this is the task of your mind. “Everything you want is just outside your comfort zone,” says Robert Allen, co-author of One Minute Millionaire.
The reptilian and emotional systems of the brain have existed together for 50 million years and interact very well. This is why it is so important to understand that these two tightly coupled systems can often take control of the mind and body. For the reptilian brain, the threat can be physical, for the emotional brain it can be emotional. For example, loss of love, fear of the unknown, or changes occurring in a person's life. Your emotional brain may reject your best efforts, such as going to the gym or losing weight. Instead of eating right, you find yourself unconsciously reaching for food. The emotional brain is a merit of this - it is concentrated on the moment “now” and sensitively monitors your desires at the moment, and immediately implements all your habits. Anyone who has lost weight knows that as soon as you lose control, the extra calories end up in your mouth.
How can you overcome the “empathetic concern” and habits of our most ancient brain structures and achieve what you consciously want? You need to learn how to harness the power of your visual brain.