Progressive supranuclear palsy
Progressive supranuclear palsy ( PSP
or
Stiel-Richardson-Olszewski syndrome
—sometimes named after the doctors who described it in 1963) is a degenerative disease associated with the gradual deterioration and death of certain brain structures. Approximately 6 people out of 100,000 people have progressive supranuclear palsy. This syndrome is usually described as tautopathy. The initial symptoms in 75% of cases are: loss of balance, falling forward, rapid walking, during which the patient may step on some objects and fall. Other common initial symptoms include personality changes, general slowness of movement, and visual disturbances.
Other symptoms and signs that appear later include dementia (usually involving disinhibition and the ability to organize information), intermittent speech, difficulty swallowing, sleep disturbances, facial muscle contracture, urinary incontinence and constipation, difficulty with gaze, especially in the vertical direction, which explains some of the falls in these patients because they cannot look up or down. Patients usually complain of difficulty reading due to an inability to look down correctly. Notably, the ophthalmoparesis that occurs in these patients primarily concerns voluntary eye movement and the inability to make vertical saccades, which is often more difficult than making downward saccades.
The cause of progressive supranuclear palsy is unknown. Less than 1% of those who have PSP have a family member with the same disorder.
A variant in the gene encoding tau protein, called haplotype H1, located on chromosome 17 is associated with PSP. Almost all patients with PSP received a copy of this option from each parent, but this applies to approximately two-thirds of the general population. However, naplotype P1 appears to be necessary but not sufficient to cause progressive supranuclear palsy; other genes, as well as environmental toxins, are considered as other possible factors influencing the cause of PSP.
The brain cells affected are both neurons and glial cells. In neurons, neurofibrillary tangles are detected, which are deposits of tau protein, part of the skeleton of the brain cell. These neurofibrillary tangles are often different from those seen in Alzheimer's disease, but may be structurally similar when they occur in the cerebral cortex. Their chemical composition is usually different, however, it may be similar to that of the glomeruli observed in corticobasal degeneration. Deposits of tau protein in astrocytes or clusters of astrocytes are also considered diagnostic. Unlike NFTs, they may be more common in the cortex. Lewy bodies are seen in some cases, but it is unclear whether this is a variant or an independent or joint process, and in some cases PSP may coexist with corticobasal degeneration, Parkinson's disease, and/or Alzheimer's disease, especially in adult patients.
The main areas affected are:
- the basal ganglia, especially the subthalamic nucleus, substantia nigra and globus pallidus;
- the brain stem, especially the part of the midbrain where “supranuclear” eye movement is localized;
- cerebral cortex, especially the frontal lobes;
- dental nucleus of the cerebellum;
- spinal cord, especially in the area where control of the bladder and bowels is located.
Some believe that PSP, corticobasal degeneration, and frontotemporal dementia are variations of the same disease. Others consider them separate diseases. PSP has been shown in some studies to be associated with Pick's disease.
Progressive supranuclear palsy is often initially diagnosed as Parkinson's disease due to slowness of movement and difficulty walking; or like Alzheimer's disease due to behavioral disturbances. However, it is one of a number of diseases that are collectively called parkinsonian disorders. Poor response to levodopa along with symmetrical onset of symptoms may help distinguish this disease from Parkinson's disease. In addition, patients with the Richardson variant tend to have an upright or arched posture, as opposed to the forward-leaning posture found in other parkinsonian disorders, although PSP parkinsonism may also present with a stooped posture. Early falls are characteristic of Richardson's syndrome.
Clinical PSP is often divided into two subgroups: progressive supranuclear palsy - Richardson's palsy and the classic type of PSP - parkinsonism, in the latter case which may respond to levodopa. Amantadine may also be useful for treatment. There is some evidence that zolpidem may improve motor function and eye movements.
Causes and mechanism of development
Paralysis may result from the following pathological processes:
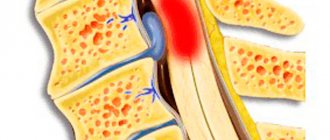
- space-occupying formations in the brain or spinal cord;
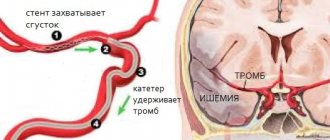
- acute disturbance of cerebral or spinal circulation;
- brain abscesses;
- spinal and traumatic brain injuries;
- demyelinating diseases (multiple encephalomyelitis, multiple sclerosis);
- inflammation of the spinal cord or brain.
Paralysis develops from poisoning with nerve paralytic and industrial poisons, salts of heavy metals, alcohol and its surrogates, and other toxic substances.
The cause of loss of voluntary movements can be myasthenia gravis, botulism, epilepsy, immunoinflammatory diseases, mechanical damage to the brain substance. Neurologists detect paralysis in patients suffering from motor neuron diseases (spinal muscular atrophy, amyotrophic lateral sclerosis). Voluntary movements of skeletal muscles are controlled by the motor area of the cerebral cortex. It contains pyramidal neurons - giant nerve cells, the processes of which descend into the spinal cord. There, the process of each pyramidal cell transmits a nerve impulse to the next neuron, which carries it to the corresponding muscle. When the chain is interrupted as a result of a congenital malformation, pathological process or damage, paralysis occurs.
Kinds
Motor nerve cells, which are located in the spinal cord, not only receive and transmit nerve impulses from the brain.
They themselves carry out simple reflexes and partially regulate muscle tone. For example, when a person unconsciously withdraws his hand from a hot object, his brain takes almost no part in this, since the nerve chain is closed in the spinal cord. Therefore, when the cerebral cortex is damaged, the muscles become flaccid only for a while. Then their tone increases, reflexes strengthen, but voluntary movements are still impossible. This type of movement disorder is called spastic paralysis.
When motor nerve cells in the spinal cord or peripheral nerves are damaged, nerve impulses to the corresponding muscles cease to flow at all. They become lethargic and decrease in size over time. Muscle atrophy develops. Neurologists call this type of paralysis flaccid.
Make an appointment
Patient examination
In order to establish the cause and type of paralysis, neurologists at the Yusupov Hospital conduct a comprehensive examination of the patient.
During the interview, the doctor asks the patient in which muscles there is a lack of strength, when he noticed the motor function disorder and for what reason it arose. The neurologist clarifies whether the patient’s relatives had similar diseases, and whether he connects the development of the pathological process with the presence of harmful substances (organic solvents, heavy metal salts) in the environment. The doctor then performs a neurological examination:
- assessment of muscle strength on a five-point scale;
- search for other symptoms of neurological pathology (facial asymmetry, lack of reflexes, muscle thinning, strabismus);
- determination of sensitivity, height of reflexes.
After a physical examination, he orders laboratory tests.
A general blood test can detect signs of inflammation (an increase in the number of leukocytes, erythrocyte sedimentation rate). In a biochemical study, an increase in the level of creatine kinase is found. A toxic blood test can detect the presence of harmful substances in the body. Patients in the neurology clinic of the Yusupov Hospital are examined using innovative research methods. Electroneuromyography is performed by leading experts in the field of physiology of the nervous system - neurophysiologists. Using a computer program, they assess the speed of nerve impulse transmission along nerve fibers and determine conduction blocks.
By analyzing electroencephalography data, the electrical activity of different parts of the brain is assessed. Using computed tomography and magnetic resonance imaging of the brain and spinal cord, the structure of these anatomical structures is studied layer by layer, a violation of the structure of their tissue is identified, the presence of abscesses (cavities filled with pus), hemorrhages, tumors, and foci of decay of nervous tissue are determined. Magnetic resonance angiography allows you to assess the patency and integrity of intracranial arteries and detect volumetric processes in the brain. If indicated, patients have the opportunity to consult a neurosurgeon.
Treatment of paralysis
The main goal of treating paralysis is to eliminate the cause of its occurrence. Most often, this includes a whole range of measures. In particular, these are: gymnastics, elimination of symptoms, various types of massages, exercise therapy. However, it should be remembered that for each individual case it is necessary to select your own treatment.
But doctors prescribe one thing to almost everyone and almost always: a patient who is “shackled” by this illness needs constant movement, but if it is difficult to move independently, outside help is needed. It is also important to remember about breathing exercises. It is also necessary to include it, since it helps develop the lungs, which usually work weaker in patients in this case.
Symptoms
The main symptom of paralysis is a lack of muscle strength in the affected muscle or muscle group. Depending on which muscle is affected, the patient may have impaired gait, drooping head and foot, and lack of muscle strength in the limbs. Cranial nerve palsies are manifested by the following symptoms:
- impaired movement of the eyeballs;
- nasality;
- slurred speech;
- sluggishness of the tongue;
- other symptoms that are associated with weakness or complete dysfunction of the facial muscles.
Signs of central paralysis directly depend on the level of damage. If the pathological process develops in the central gyrus of the cerebral cortex, the function of the upper and lower limbs falls on the opposite side of the pathological focus. When the pyramidal fibers of the brainstem of the head are damaged, hemiplegia occurs on the opposite side, combined with central paralysis of the muscles of the face and half of the tongue. Bilateral central motor neuron damage to the cranial nerves results in pseudobulbar palsy.
Central paralysis is manifested by the following symptoms:
- an increase in tendon reflex perceptions, which is accompanied by an expansion of the reflexogenic zone;
- muscle maintenance;
- the occurrence of pathological reflexes and synkinesis (involuntary movements of a limb or other parts of the body that accompany another passive or voluntary movement).
Increased muscle tone occurs reflexively. At the same time, the muscles are in constant tension. Resistance to passive movements requires significant effort.
Peripheral paralysis is the result of damage to the second motor neuron. There is a weakening or complete absence of tendon reflexes, decreased muscle tone, muscle atrophy, and degeneration of nerve fibers. Due to the death of nerve fibers, muscle imbalance occurs. The clinical picture of peripheral paralysis depends on the level and extent of damage to the peripheral neuron. If the anterior horns and nuclei of the cranial nerves are involved in the pathological process, peripheral paralysis is combined with muscle atrophy and characteristic fascicular twitching.
Movement disorders caused by pathology of the nuclei, brain stem, and cranial nerves are bulbar palsy. In case of deformation of the peripheral nerve, paralysis of the muscle innervated by it occurs. Due to the fact that peripheral nerves contain sensory fibers, patients experience impaired sensitivity. When the cervical, brachial, lumbar and sacral plexuses are damaged, peripheral paralysis of the muscles innervated by this plexus and lack of sensitivity occurs.
In which muscles can paralysis develop?
Paralysis, depending on the damage to one or another part of the nervous system, can develop in different parts of the body. Paralysis in different muscle groups has the following names:
- paralysis of one upper or lower limb - monoplegia;
- paralysis of both legs or arms - paraplegia (occurs when the spinal cord is damaged);
- paralysis of the left or right half of the body - hemiplegia (develops in patients suffering from stroke);
- tetraplegia – paralysis of all four limbs,
- Neurologists call paralysis of the facial muscles prosopoplegia.
Progressive paralysis
Progressive paralysis, or Bayle's disease, is a psychoorganic disease of syphilitic origin, characterized by a progressive disturbance of mental activity with the formation of a persistent defect up to dementia in combination with neurological and somatic disorders. Progressive paralysis is one of the forms of syphilis of the brain, characterized by the occurrence of meningoencephalitis (damage to syphilitic treponema of the brain tissue and its membranes). Only 1-5% of those who have had syphilis develop progressive paralysis. Men suffer 3-5 times more often than women. The average age of patients is from 35 to 50 years, i.e. progressive paralysis develops 10-15 years from the onset of syphilis. In the majority of those admitted to treatment in a psychiatric hospital for progressive paralysis, the syphilitic nature of the disease is established either directly during examination, or by chance during hospitalization in other medical institutions, where a blood test for the Wasserman reaction is mandatory. If a positive result is detected, the patient consults a venereologist, who, in turn, having determined the stage of the disease and predominantly mental disorders, refers him to a psychiatrist.
In other cases, the patient is admitted to a psychiatrist due to abnormal behavior or other mental abnormalities that are noticed by others (the patient usually does not have a critical attitude towards his illness), and the nature of the disease is established in the clinic. Patients, having learned their diagnosis, are often perplexed about this or even deny the presence of syphilis in the past, because they either really did not attach importance to the mild manifestations of the disease at stages 1 and 2 of the disease, or did not complete the full course of treatment for one reason or another.
Symptoms and course:
At the initial stage of the disease, nonspecific complaints of headaches, fatigue, irritability, sleep disturbances, and lethargy appear. However, quite soon signs of personality decline appear with loss of skills, moral attitudes, and intellectual level.
They cannot concentrate, become forgetful, and are unable to perform their usual functions (for example, work). Not only is consciousness of the disease lost, but also unjustified optimism, elevated mood, rudeness, explosiveness, and disinhibition of drives appear. In other patients, on the contrary, dullness, indifference, and lethargy increase.
The middle stage of the disease (paralytic dementia) is characterized by the leveling of individual personality traits with a complete loss of criticism. Either a benevolent high spirits or dull indifference prevails. Memory deteriorates sharply, dementia increases.
The initial stage (marasmus) occurs on average 3-5 years from the onset of the disease. By this time, a complete breakdown of mental activity occurs, physical helplessness develops, leading to death. However, with modern treatment methods, patients usually do not reach this stage, but remain at the level of paralytic dementia.
Recognition:
In addition to mental disorders, progressive paralysis is characterized by neurological manifestations: constriction of the pupils, their unevenness (anisocoria) and irregular shape, lack of reaction of the pupils to light. One of the early symptoms is speech impairment (slurred speech), then epileptic seizures appear, handwriting changes, and tendon reflexes are impaired. When making a diagnosis, special reactions of the blood and cerebrospinal fluid to syphilis are also used. The most famous of them is the Wasserman reaction (R.V.).
Treatment:
It consists of specific antibiotic therapy (8 courses) in combination with bioquinol. In the past, the method of inoculation with three-day malaria was widely used to increase body temperature, which contributed to the death of Treponema pallidum (the causative agent of syphilis). Currently, sulfozine and pyrogenal are used for this. The results of treatment are different and depend on the stage of the disease (the earlier the patient applies, the better the prognosis), as well as on the adequacy of therapy.
Prevention:
Prevention of syphilis in general and carrying out a full course of treatment in the early stages of the disease.