Types of intracerebral formations of the brain
Astrocytoma
The most common types of intracerebral brain tumors are:
- Neoplasms that arise from the vessels of the brain and meninges.
These tumors include meningioma. It is characterized by slow growth and can be treated quite effectively using surgical techniques. Also included in this category is angioreticuloma. This benign intracerebral mass is localized primarily in the cerebellum.
- Neoplasms of neuroectodermal nature.
Such formations include the following types:
- astrocytoma;
- glioma;
- glioblastoma.
- Pituitary and metastatic tumors.
The exact type of tumor can be determined using neurological diagnostics. The capabilities of diagnostic neurology today make it possible to easily identify such benign and malignant neoplasms. The Burdenko Research Institute has modern technical equipment, which is used both at the differentiation stage and during the period of assessing the effectiveness of operations performed and at the stage of preparation for surgical interventions.
Structure of brain tissue
The brain is a very complex and very fragile structure, so nature has created a triple system of brain protection. As a result, the brain is covered in three protective layers.
This is, firstly, a soft choroid that fuses with the brain and fills its entire space.
Secondly, this is the arachnoid membrane, which fuses with the soft one and connects with the hard one.
And thirdly, it is a hard shell that fuses with the periosteum of the skull and connects with the arachnoid.
The structure of the shells can be schematically represented as follows:
The terms “epidural space”, “subdural space”,
The “subarachnoid space,” which you can read on the diagram, refers to the space between the layers of the brain. CSF channels are channels through which cerebrospinal fluid circulates. Sometimes it is also called cerebral fluid.
Liquor is generated from blood plasma, penetrates into the space under the membranes and “goes” to the lymph nodes. Cerebrospinal fluid nourishes nerve cells, maintains stability of intracranial pressure, protects the brain from concussions and removes harmful metabolic products.
The brain itself consists of gray and white matter. Gray matter is on the outside, forming the cerebral cortex, white matter is on the inside. The gray matter layer can range from 1.3 to 4.5 millimeters, with the layer being thicker at the front of the brain.
The gray matter contains neurons and glia, the supporting cells of the central nervous system. It is the number of neural connections that determines the effectiveness of a person’s thinking, the ability to compare new information with existing information, etc.
The number of neurons in the brain is in the billions. Thus, there is evidence that the adult male brain contains on average 86.1 billion neurons +/- 8.1 billion [F. Azevedo et al., 2009]. And some scientists believe that the number of neurons in the human brain can reach 100 billion [R. Hodson, 2019].
Neurons have processes called axons and dendrites. The function of axons is the propagation of nerve impulses, the function of dendrites is the receipt of nerve impulses. The relationship between axons and dendrites can be schematically represented as follows:
Glial cells (glia) are responsible for the coordinated functioning of neurons, providing neurons with nutrients. The cerebral cortex plays a leading role in higher nervous activity, ensures communication between brain cells, and corrects deviations in the functioning of human systems and organs.
The white matter of the brain consists primarily of axons, which are covered with myelin. Hence the name “white matter” because myelin is white in color. Please note that the so-called unmyelinated axons, which are not covered with myelin, are concentrated in the gray matter.
White matter connects different areas of gray matter, where nerve cells are located, to each other, and provides the transfer of impulses between neurons. The myelin coating in this case functions as a signal accelerator.
The brain contains 12 pairs of nerves, each of which provides a specific function:
- 1 pair – olfactory.
- 2nd pair – visual.
- 3 pairs – oculomotor.
- 4th pair – trochlear (innervate the muscles that rotate the eyeballs outward and downward).
- 5 pair - trigeminal (responsible for the sensitivity of the facial muscles).
- 6th pair – abductors (innervate the muscles responsible for abduction of the eyeball).
- 7th pair – facial (innervates facial muscles).
- 8th pair – vestibulocochlear (responsible for transmitting auditory signals and impulses from the inner ear).
- 9th pair – glossopharyngeal.
- 10th pair – vagus (innervates internal organs).
- 11th pair – accessory (innervate the muscles responsible for turning the head).
- 12 pair - sublingual.
In general, the functions of the nerves are clear from their names, so explanations in parentheses are provided only where the names are not very informative. You can see the location of the nerves in the brain in the following picture:
The cerebral cortex is divided into lobes, the location and functions of which we discussed above, and is dotted with convolutions, due to which the surface area of the cortex can reach 2-2.5 square meters. The more convolutions, the more gray matter is “fitted” in the brain and the more neural connections can potentially be formed, and the higher the brain's performance. The appearance of a large number of convolutions is a product of evolution, as a result of which complex cognitive structures can develop without increasing the volume of the cranium.
So, we have examined in the most general simplified form how the human brain works, its structure and the structure of the tissues of which it consists. This, in general, is enough to understand the general patterns of brain function and what thought processes actually depend on. You can develop thinking techniques more deeply by studying our Cognitive Science program.
We wish that your brain always functions flawlessly and never fails you. And in conclusion, we suggest you take a short test on the topic of the article :
We also recommend reading:
- Storytelling
- Books about development and for development
- 3 tasks for quick brain training
- 10 simple ways to keep your brain sharp
- Neuroplasticity
- 5 neurolifehacks: how to improve brain productivity
- Intelligence and its development: several recommendations
- Brain structure
- “Are you out of your mind?” or 32 exercises for brain development
- Creativity and logic: the myth of functional asymmetry of the cerebral hemispheres
- Brain digest
Key words:1Cognitive science
Localization of tumors
Astrocytoma of the right parietal lobe
Clinical manifestations depend on the location of the tumor. Intracerebral tumors of the frontal lobe do not make themselves felt for a long time. When the tumor is localized on the left, speech disturbances appear. Later, weakness occurs in the muscles of the arms and face on the right.
Intracerebral tumor of the temporal lobe is often accompanied by hallucinations and epileptic seizures. Subsequently, visual impairment in the form of loss of visual fields, when half of the image on the left or right is not visible, joins the main manifestations.
Among intracerebral tumors of the cerebellum, meningioma is the most common. The growth of the tumor is accompanied by impaired memory and consciousness, constant headaches, and a tendency to epileptic seizures. The tumor grows from the arachnoendothelium of the brain and is characterized by slow growth.
Parietal lobe
The parietal lobe is a part of the cerebral cortex, lying between the occipital and frontal lobes, and above the temporal lobe. It is named for its proximity to the parietal bone, the wall of the skull (from Latin pari, wall). The parietal lobe takes part in five somatic functions: primary analysis of somatic sensations (touch, position of limbs, temperature); spatial analysis using all sensory modalities; determination of spatial goals for the motor system; attention; and visual motion analysis.
Understanding of the role of parietal function arose from analysis of the deficits of patients with lesions of the parietal lobe (Critchley 1953)). Subsequent understanding of the mechanisms of parietal function came from neuroanatomical and neurophysiological studies.
The parietal lobe occupies a unique place in the human brain. Anatomically, it lies at the crossroads between the frontal, occipital and temporal lobes, thereby providing the basis for multimodal sensory integration. Functionally, the parietal lobe supports "high" cognitive functions characteristic of humans, such as mathematical knowledge, semantic and pragmatic aspects of language, and abstract thinking.
The largest tract identified in both humans and monkeys is the vertical tract between the superior and inferior parietal lobules. This tract can be divided into anterior (supramarginal gyrus) and posterior (angular gyrus) parts. The second intraparietal tract connects the postcentral gyrus with the supramarginal and angular gyrus of the inferior parietal lobule. The third pathway connects the postcentral gyrus with the anterior region of the superior parietal lobule and is more pronounced in monkeys compared to humans. Finally, short U-shaped fibers were identified in the medial and lateral parts of the parietal lobe.
The general picture of intraparietal connection confirms the special role of the inferior parietal lobule in cognitive functions characteristic of humans.
Three regions of the inferior parietal lobule and the adjacent lateral intraparietal sulcus (IPS) are distinguished by the relative strength of their connections to the superior colliculus, parahypocampal gyrus, and ventral premotor cortex. The medial IPS appears to be connected to the superior colliculus. The posterior angular gyrus and adjacent superior occipital gyrus are most likely connected to the parahypocampal gyrus.
In processing somatic, visual, acoustic, and vestibular sensory information, parietal lobe projections play a critical role in spatial cognition and control of eye and limb movements. Sensory information from the primary and secondary somatosensory areas enters the superior parietal lobule and is carried to the inferior parietal lobule. Visual information is processed through the dorsal visual pathway and reaches the inferior parietal lobule, the intraparietal sulcus. Acoustic information is transmitted backward from the primary acoustic area and reaches the posterior region of the inferior parietal lobule. Areas of the intraparietal sulcus project to the premotor area, frontal orbital fields, and prefrontal area. These areas are involved in the control of eye movements, reaching and grasping objects in the upper limbs, and spatial working memory. The posterior region of the inferior parietal lobule either directly or indirectly through the posterior angular gyrus is sent to the parahippocampal and entorhinal cortex. Both of these areas are closely related to the functions of the hippocampus for long-term memory formation.
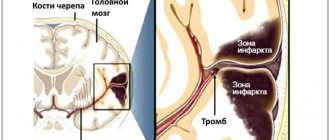
Clinical manifestations
In case of intracerebral tumors, general cerebral symptoms come first. They are associated with the appearance of hydrocephalus, provoked by increased intracranial pressure. Headaches are dull and bursting in nature. An additional symptom is dizziness. It occurs when rotating the head, often accompanied by nausea and tinnitus. First of all, dizziness occurs with tumors of the cerebral hemispheres.
One of the symptoms of the disease is vomiting, which is not associated with food intake and occurs mainly in the morning on an empty stomach and at the peak of the pain syndrome. With the growth of a tumor in the area of the ventricle of the brain, it is possible to identify mental disorders that manifest themselves with irritability, aggressiveness, or periods of severe apathy.
Patients' attention is impaired, memory deteriorates, and delusional states and hallucinations may occur. The tumor begins to affect surrounding tissues, causing displacement and infringement of brain structures, signs of ischemia, and insufficient blood flow.
General brain structure
To simplify the task, we will take as a basis material from a school biology textbook for grade 8, where the structure of the human body is explained [V. Pasechnik, 2010]. And to make it more interesting, we will supplement the explanations with interesting facts from other sources.
So, the brain is located in the cranium and occupies up to 80% of its volume. The weight of the brain on average is 2% of the total weight of a person. This explains the difference between the average brain weight of men and women: men weigh more on average than women. Interestingly, no linear relationship was found between the weight and size characteristics of the brain and human intelligence, and bigger does not mean better.
History shows that a record-breaking brain weighing 2850 grams was discovered in a young man who suffered from epilepsy and idiocy [G. Elliot, 1925]. At the same time, according to the head of the embryology department of the Research Institute of Human Morphology, Professor Sergei Savelyev, 72% of gifted people have a brain that exceeds the average weight [S. Kuzina, 2010].
One way or another, despite all the differences in size and abilities, all people have the same brain structure. The structure of the brain is considered, firstly, in the context of the functions of the hemispheres, and secondly, in the context of the functions of various parts or lobes of the brain. From the school biology course we remember (or don’t remember) that the brain consists of the following parts:
- Frontal lobe.
- Parietal lobe.
- Temporal lobe.
- Occipital lobe.
- Cerebellum.
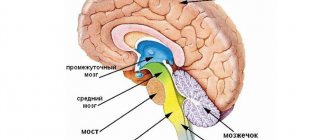
- Diencephalon (thalamus, hypothalamus, pituitary gland).
- Midbrain.
- Bridge.
- Medulla.
In addition, the spinal cord originates from the brain. Since the spinal cord is not the topic of today’s material, we will not consider it, but we suggest studying the general diagram of the structure of the brain
The most attentive of you have noticed that the diagram does not show some parts of the brain from the list above. Everything is correct, because the diagram shows only the external structure of this organ. Everything inside is hidden by the outer lobes and parts of the brain.
In order not to clutter the diagram and not to confuse you in the details and nuances of how the human brain is structured, we will give an idea of the location of the internal components of the brain relative to the external ones in separate pictures as we look at the parts of the brain. Now let's move on to studying the functions of each of them.
Medulla
It is a continuation of the spinal cord, and its main function is conduction. Through the medulla oblongata, information is transmitted to other parts and there is a reverse transfer of information from the brain to the spinal cord.
In addition, this part of the brain is responsible for many different protective reflexes, in particular sneezing and coughing. The centers of respiratory and digestive reflexes, such as swallowing and salivation, are also located here.
Bridge
The pons is adjacent to the medulla oblongata and its main function is directly related to it. It is through this “way station” that the medulla oblongata transmits signals to the rest of the brain and through it receives signals coming from different parts of the brain.
In the medical literature you can find the second name “Varoliev's bridge”, named after the Italian physician and anatomist Constanzo Varolius (1543-1575), who made a huge contribution to the study of the structure of the brain.
Midbrain
This part of the brain is responsible for the primary processing of visual and auditory information, including the so-called “hidden” or “lateral vision.” Information about everything that comes into our field of vision enters the brain, but remembering what we saw with hidden vision is somewhat more difficult than what we consciously focused our gaze on.
In addition, the midbrain is responsible for some vital reflexes, such as the orientation reflex. When we startle from an unexpected loud sound (thunder, falling object, squeaking brakes) or a bright flash (lightning, explosion), and then try to figure out the origin of the sound or flash, this is an example of the work of the orienting reflex and the midbrain.
As we just found out, the midbrain conducts the primary processing of visual and auditory information, and the orientation reflex is directly related to these functions.
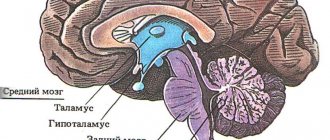
Diencephalon (thalamus, hypothalamus, pituitary gland)
Here we will talk about the main components of the diencephalon: the thalamus, hypothalamus and pituitary gland. The hypothalamus is responsible for reflexes such as thirst and hunger, regulates sleep, maintains the stability of the internal environment of the whole body and is involved in the formation of emotions. For example, such as love and aggression.
The thalamus is sometimes called the “central relay station of the brain,” where almost all sensory and motor information is collected, with the exception of signals from the olfactory organs. In addition, the thalamus is involved in controlling motor functions, speech and memory.
The pituitary gland, in principle, is an organ of the endocrine system in which the synthesis of hormones that affect metabolism, growth and reproductive function is carried out. The pituitary gland is closely interconnected with the hypothalamus and forms the hypothalamic-pituitary system, which regulates many body functions related to metabolism, reproductive function, and growth.
Cerebellum
The cerebellum is anatomically located behind the medulla oblongata and the pons and is responsible for coordination of movements, balance, maintaining the desired body position and muscle tone. The traditional way to test cerebellar function is to stretch your arms out in front of you with your eyes closed and then touch the tip of your nose without opening your eyes. A healthy person can easily do this, despite the fact that about 30 muscles are involved in this simple movement.
In addition to coordinating movements, this part of the brain performs an adaptive-trophic function, which ensures the body’s adaptation to changing conditions.
Occipital lobe
The occipital lobe borders the parietal and temporal lobes. Visual analyzers are concentrated in this part of the brain. They include the so-called “primary visual cortex” and visual association areas.
To make it clearer what we are talking about, let's say that disturbances in the primary visual cortex lead to a specific visual disorder, Anton Babinski syndrome. This is when people do not distinguish objects by appearance, but at the same time they do not even suspect their disorder and are sure that they see exactly what they really are. You can learn more about this syndrome from the video lecture dedicated to this problem:
Temporal lobe
The temporal lobe is adjacent to the frontal, occipital and parietal lobes. Auditory and taste analyzers are concentrated in this part of the brain. Thanks to auditory analyzers, we recognize speech and can perceive music. If there are disturbances in the right lobe, a person loses the ability to perceive music; if in the left, he will have a speech disorder.
Here, in the temporal lobes, is the hippocampus. This is a paired structure that, together with the cortex (outer covering) of the temporal lobe, is involved in the formation of emotions, long-term and spatial memory.
In addition, the so-called “ amygdala ” is located in the temporal lobes. This is also a pair structure, one “body” on each side. The amygdala is responsible for the formation of many emotional reactions, such as fear, and decision making.
If it is destroyed, say, due to illness, a person will not experience a feeling of fear and will not be able to make a decision adequate to the threatening danger.
Parietal lobe
The parietal lobe is adjacent to the frontal, temporal and occipital parts of the brain. It is responsible for processing and integrating sensory information. For example, for the perception of the relationship between tactile sensations and pain. Thus, a person learns that if you touch something hot, it will hurt and you can get burned.
In addition, this part of the brain allows you to orient yourself in space and understand which part of the body is affected by sensations. For example, you touched a hot object with your finger or palm, or accidentally caught it with your elbow.
Frontal lobe
The frontal lobe covers the anterior parts of the cerebral hemispheres. It is adjacent to the parietal and temporal lobes. The frontal lobe is responsible for learning, perception of information, memory and thinking. Thus, when someone is called “brainless”, it essentially means that the frontal lobes are not functioning very well, not the entire brain.
In general, the frontal lobes can be thought of as the “command post” of the entire brain. The health and safety of these lobes of the brain determines a person’s ability to analyze the situation, take initiative, make independent decisions, and control their behavior.
When this part of the brain is damaged, a person often experiences symptoms similar to those of laziness: lack of interest in what is happening, lack of initiative, inadequate carelessness. In addition, a person may lose social control over his behavior and, for example, begin to use profanity in public places.
Another difficulty that accompanies frontal lobe disorders is the loss of previously acquired skills. For example, a person forgets how to cook a particular dish that he prepared before. In this case, learning new skills is also difficult and sometimes impossible.
A sign of a disorder in this part of the brain is also perseveration in speech (for example, repetition of words unreasonable by the situation) or in actions (meaningless shifting of things from place to place). And finally, the frontal lobes are responsible for upright posture and maintaining an upright body position. When the lobes are affected, a specific “mincing” gait and constant stoop may be observed.
In addition to all of the above, in the medical literature you can find the term “telebrum”. This refers to the cerebral hemispheres covered with cortex, the corpus callosum, the striatum and the olfactory brain. We will tell you more about the cerebral cortex a little later, when we consider the structure of brain tissue. Let’s say a few words about the remaining components of the telencephalon right now.
The corpus callosum is responsible for coordinating the hemispheres and transmitting information from one hemisphere to the other:
The striatum regulates muscle tone, takes part in the formation of conditioned reflexes and regulation of the functioning of internal organs:
The olfactory brain , as the name implies, is responsible for the sense of smell and is part of the so-called “ limbic system ” of the brain, which refers to the totality of brain components and their connections involved in controlling instinctive behavior and autonomic functions:
This is, let’s say, “knowledge for the advanced,” so we will not dwell in detail on the structure of this part of the brain. Here we have provided this information so that you understand what we are talking about if you suddenly come across these terms in the specialized literature.
By the way, the limbic system is sometimes called the “animal part” of the brain because it is more about reflexes than consciousness. In this regard, the book “Will and Self-Control” is very interesting. How genes and the brain prevent us from fighting temptations” [I. Yakutenko, 2020].
So, we have found out how the human brain is structured, and now we know that the brain is symmetrical. From a school course in biology and general development, we know that the brain is divided by a fissure into two hemispheres, right and left, and that the functions of these hemispheres are different.
A natural question arises: if we have already studied in general terms the functions of all parts of the brain, how exactly should the functions of the right and left hemispheres differ? To understand this nuance, you should know that the left hemisphere processes information that comes in gradually, and the right hemisphere instantly creates a complete image. The left hemisphere stores information that needs to be thought through and coordinated, while the right hemisphere stores previously created and imprinted images.
Thus, when you are preparing for a report or exam, the left hemisphere is working, and when a spontaneous idea comes to your mind, even regarding the topic of the report or exam paper, this means that the right hemisphere is “involved” in the process. If you are right-brain dominant, you can visualize the difference between the hemispheres by simply looking at the picture with examples of the work of the right and left hemispheres:
Even a cursory glance is enough to understand: how the human brain is structured and human psychology are closely interconnected. The foundations of the processes that predetermine a person’s behavior, his success or lack of achievement in life, the presence or absence of talents for music, painting or poetry, stem from the depths of the brain.
This is why scientists are so interested in the structure of the brain, its mysteries and secrets. Moreover, it is believed that the human brain has not yet been fully studied, and new discoveries are yet to come.
If it’s easier for you to perceive information by ear than from text, we can recommend a video on the topic “How the human brain works” - a biology lesson for grade 8:
It tells how the human brain works for children, so the presentation is simple, understandable and gives a general idea of the topic, quite sufficient for a person who, due to his profession, is not related to medicine. From this video you can learn about both the structure and structure of brain tissue. We will dwell on the structure of tissues in a little more detail.
Treatment methods
The treatment tactics for intracerebral formations are selected by a neurosurgeon or neurologist after a comprehensive examination. It includes the appointment of the following studies:
- EEG, Echo-EG;
- determination of visual acuity;
- ophthalmoscopy;
- perimetry;
- MRI and CT of the brain.
The main diagnostic method is magnetic resonance imaging. With its help, you can identify the exact location of the tumor and differentiate the tumor from an intracerebral hematoma, abscess or cyst.
Removal of the brain mass is the main treatment method. When a pathological lesion grows into the brain tissue, shunt operations are used, which ensure the outflow of cerebrospinal fluid and the installation of modern drainage systems. Additionally, specialists use radiation therapy. With its help, you can influence the pathological formation from different positions, while preserving healthy cells. This slows down further growth of the tumor and reduces the main clinical manifestations.
Surgical treatment can be combined with radiation therapy, as well as chemotherapy. But the main method of combating the disease is surgery. Precision neurosurgical operations make it possible to completely or partially remove brain tumors, relieve the patient from severe clinical manifestations of pathology and improve the future prognosis.
General information about the parietal lobe
The parietal lobe is a part of the cerebral hemisphere that is located behind the central sulcus.
The posterior border runs along the parieto-occipital sulcus and borders the occipital lobe. On the sides, the parietal lobe is limited by the Sylvian fissure. This structure of the cerebral hemisphere has the following main grooves:
- postcentral, which in turn is divided into upper and lower;
- interparietal.
The intersection of these grooves is called the helix, or star.
In the anterior part is the postcentral gyrus. The other two gyri are the superior parietal and inferior parietal, which are located horizontally.
b) Syndrome of disturbance of spatial synthesis
Also known as “ TPO syndrome ” is a syndrome of damage to the tertiary temporo-parieto-occipital cortex, which provides simultaneous (simultaneous) analysis and synthesis at a higher supramodal level (“quasi-spatial” according to Luria).
What is the manifestation of damage to the SRW zone?
Damage to the TPO zone manifests itself in disturbances in orientation in external space (especially on the right - left), defects in the spatial orientation of movements and visual spatial actions (constructive apraxia).
In visual-constructive activity, lateral differences are observed, which are easily detected in tests for drawing (or copying) various objects.
Significant differences occur when drawing (copying) real objects (house, table, person) and schematic images (cube or other geometric structures).
At the same time, it is important to evaluate not only the final result of performing a visual-constructive task, but also the dynamic characteristics of the execution process itself.
In the process of drawing (copying), patients with damage to the TPO zone of the right hemisphere of the brain perform a drawing, first depicting its individual parts, and only then bringing it to the whole.
With left-hemisphere lesions, visual-constructive activity unfolds in the opposite direction: from the whole to the details. At the same time, patients with damage to the right hemisphere tend to draw realistic parts of the picture (hair, a collar on a person, crossbars at a table, curtains, a porch at a house, etc.), while patients with left hemisphere tend to draw schematic images.
With right-hemisphere lesions, visual-constructive activity suffers more deeply, as evidenced by a violation of the integrity of the copied or independently depicted picture. Often parts are taken outside the contour and “attached” to it in random places. Structural errors such as lack of closure of the figure, violation of symmetry, proportions, and the relationship between the part and the whole are quite often observed. The presence of a sample not only does not help patients with damage to the right hemisphere (unlike those with left hemisphere), but often complicates and even disorganizes visual-constructive activity.
In addition to the listed symptoms, when the SRW zone is damaged, the following symptoms appear:
- agraphia,
- mirror copying,
- acalculia,
- finger agnosia,
- speech disorders (“semantic aphasia”, “amnestic aphasia”).
Violations of logical operations and other intellectual processes are noted. Patients are characterized by difficulties in operating with logical relationships, which require, for their understanding, the correlation of the elements included in them in some conditional, non-visual space (quasi-space).
The latter include specific grammatical constructions, the meaning of which is determined by the endings of words (father’s brother, brother’s father), ways of their arrangement (the dress touched the oar, the oar touched the dress), prepositions reflecting the turn of events in time (summer before spring, spring before summer), discrepancy between the actual course of events and the order of words in a sentence (I had breakfast after reading the newspaper), etc.
Intellectual disorders are manifested by disturbances in visual-figurative thought processes (such as mental manipulation of three-dimensional objects or tasks on “technical” thinking). Such patients cannot read a technical drawing or understand the structure of a technical mechanism.
The main manifestations also include disorders associated with operations with numbers (arithmetic problems).
Understanding of numbers is associated with a rigid spatial grid of placing the digits of units, tens, hundreds (104 and 1004; 17 and 71); operations with numbers (counting) are possible only if the scheme of the number and the “vector” of the operation performed are kept in memory (addition - subtraction; multiplication - division).
Solving arithmetic problems requires understanding the conditions containing logical comparative constructions (more - less by so many times, so many times, etc.).
All of these disorders are especially pronounced in left-sided lesions (in right-handed people).
With right-sided lesions in TPO syndrome there are no phenomena of semantic aphasia; Disturbances in counting and visual-figurative thinking become somewhat different.
Medical Internet conferences
Introduction. The parietal foramen is found in 33–87% of skulls (about 60% in most populations), more often on the right [1–4 ] , demonstrating a weak connection with other non-metric characters [5]. The diameter of the parietal foramen usually does not exceed 2 mm [1, 6 – 8], in 70–78% of cases it ranges from 0.5 to 1.0 mm, in 19–23% – from 1.1 to 1.5 mm, in 3.7% it is more than 1.5 mm [9, 4], and the size of the right hole prevails over the size of the left one [4]. The diameter and number of parietal foramina are subject to pronounced age-related variability [9-13]. Through the parietal foramen, venous blood flows from the soft tissues of the calvarium and its periosteum into the superior sagittal sinus [14], and arterial anastomoses pass through the parietal foramen [7, 3, 15]. Various forms of diploe – emissary communications have been described [16].
Purpose: a comprehensive description of age, gender, topographic, bilateral and individual variability of the parietal foramen.
Methods. The study material included 819 cranial vaults. The material was divided into age groups in accordance with the age periodization scheme adopted at the 7th All-Union Conference on Problems of Age-Related Morphology, Physiology and Biochemistry of the Academy of Pedagogical Sciences of the USSR. Due to the fact that at least 30 skulls must be examined when analyzing nonmetric features, some age groups were combined (Table 1).
The frequency of parietal foramina was calculated both per skull and per side of the skull, taking into account the frequency of unilateral and bilateral foramina. The outer and inner diameters of the parietal foramina were measured using an MBS-2 binocular magnifier with an ocular ruler insert. The angle of inclination of the parietal foramen in the sagittal plane was determined using a protractor as the angle between the probe inserted into the hole and the outer surface of the post-obelion part of the parietal bone (obelion is a point in the median plane at the intersection of the line connecting the parietal foramina, or on the perpendicular restored from the hole) . The position of the hole on the outer surface of the skull was determined as the distance from the center of the hole to the obelion (using an MBS-2 binocular loupe with an ocular ruler insert) and from the obelion to the lambda (lambda is the connection point of the sagittal and lambdoid sutures of the skull) using a millimeter tape.
When statistically processing the primary data, methods of variation statistics were used and, to identify patterns of age-related changes, correlation and regression analysis was used. In this case, the age of the skull was taken as an independent variable, and the resulting mathematical models were considered as the basis for judging the patterns of age dynamics of the studied parameters of the parietal foramen. To determine the strength and reliability of the influence of gender and age factors on the frequency of parietal foramina, analysis of variance of two-factor complexes was used.
Results. Age-related changes in the frequency of the parietal foramina, regardless of the gender of the skull, are presented in Table 2 and are approximated by a parabolic function with one maximum, reflecting the pattern of increase in frequency until adulthood and its decrease in old and senile age:
p = 0.217 + 0.207 (x + 1) – 0.024 (x + 1)²,
where p is the overall frequency of the parietal foramina (on the right, left and on both sides of the skull), x is the serial number of the age group (Table 2).
In all the material studied, the overall frequency of the parietal foramina is 0.578±0.017. The frequency of the parietal foramen on one side is 0.334±0.017, on both sides – 0.244±0.015. The difference between these values reaches the level of statistical significance at the highest level of error-free judgment (t=3.97; p<0.001). In the unilateral position, the frequency of the right parietal foramen (0.195±0.014) is significantly (t=3.04; p<0.01) higher than the left one (0.139±0.012). Of all 624 detected holes, 54.6±2.0% were right, and 45.4±2.0% were left; the differences between these indicators are also statistically significant (t=3.20; p<0.01).
In the skulls of fetuses, out of 66 detected holes, 40 are located in the bone, and 26 are located in the membrane of the posterior fontanel, while the parietal holes occur with a frequency of 0.430±0.050, which is significantly (t=3.18; p<0.01) less than the frequency parietal foramina in the postnatal period (0.599±0.018). In fetal skulls, the differences in the frequencies of the parietal foramina on one side (0.200±0.040) and on both sides (0.230±0.042) are not significant (t=0.52; p>0.05) (even with a slight predominance of skulls with bilateral foramina positions) , as well as the differences in frequencies of the right and left holes.
Statistical significant differences were revealed between the maximum frequency of parietal foramina (in the second period of adulthood - 0.679±0.036) and in the first age group (0.545±0.045, t=2.06; p<0.05), as well as in old age (0.509 ±0.047, t=2.87; p<0.01). In old age, the differences between the frequencies of the parietal foramen on one side and on both sides are significant (t=2.31; p<0.05), while the significance of the differences between the frequencies of the right and left parietal foramina becomes statistically insignificant (t=1.47 ; p>0.05). In old age, the differences between the frequencies of the parietal foramina on one and both sides, as well as the frequencies of the right and left foramina, are statistically insignificant (t=0.78 and t=0.98, respectively; p>0.05).
In old and senile age, in the obelion section of the vault, 12% of skulls have holes with a diameter of 0.2–0.5 mm, which are not through. X-rays of the corresponding sections of the vaults will allow us to regard these openings as the mouths of the diploic canals. At the same time, the typical location and size indicate that they may be traces of parietal foramina obliterated from the inside.
To identify sexual dimorphism in the frequency of parietal foramina, 362 male and 236 female skulls of people aged 8–90 years were examined (Table 3).
Parietal foramina are significantly more common in female skulls than in male ones. These differences are most pronounced in the skulls of the second period of adulthood, mainly due to the high frequency of parietal foramina on both sides in female skulls. In male skulls, the frequency of parietal foramina on the right and both sides decreases with age, whereas the frequency of foramina on the left increases to a maximum in the skulls of older people. In female skulls, the frequency of parietal foramina on the right and left increases towards adulthood and decreases in old age.
Discussion. The total frequency of the parietal foramen found on all studied material (on the right, left and on both sides of the skull) is 57.8±1.7% (in the postnatal period - 59.9±1.8), while the parietal foramen is more often found on one side (33.4±1.7%) than on both (24.4±1.5%), mainly on the right, which corresponds to the information given in the literature (about 60%) [1 – 4]. A significantly higher frequency of parietal foramina in the postnatal period (59.9±1.8%) compared to the frequency of parietal foramina in fetuses (43.0±5.0%) suggests that the formation of foramina continues after birth. The absence in the skulls of fetuses of differences in the frequencies of the parietal foramina on one and two sides (with a certain predominance of skulls with a bilateral position of the foramina), as well as differences in the frequencies of the right and left foramina, may indicate the formation of bilateral variability of the parietal foramina (the predominance of skulls with a unilateral position of the foramen and predominance of holes on the right) in postnatal ontogenesis. In elderly and senile age, a decrease in the frequency of the parietal foramina occurs mainly due to the holes located on the right, due to which the characteristic right-sided predominance of the frequency of the parietal foramina is smoothed out. In this case, obliteration coming from the internal compact plate mainly affects the parietal foramina of small diameter. Parietal foramina are more common in female skulls; these differences are most pronounced in the skulls of people in the second period of adulthood. The age-related dynamics of the frequency of parietal foramina is different in male and female skulls.
What fields are included?
In total, the parietal lobe of the brain has nine fields.
The first three fields, which are 1, 2 and 3, are primary sensorimotor fields. They are located in the vertical gyrus of the parietal lobe (postcentral). The fourth field is the primary motor cortex. Areas 5 and 6 are secondary somatosensory and motor areas, respectively. The seventh field, which is located in the upper part of the parietal lobe, is the tertiary motor cortex. Field 39, in turn, is responsible for analyzing written speech. The main function of field 40 is reading comprehension, as well as ensuring the reading process. This part of the brain is characterized by the presence of the following centers:
- - responsible for recognizing the position of the body and individual organs in space;
- sensitivity center – analyzes information about any changes in the environment;
- center of praxia – responsible for performing complex actions;
- vocabulary center – helps in recognizing letters and other signs;
- calculus center - responsible for carrying out numerical calculations in the mind.