Main convolutions
Although the shape and size of some of the sulci and convolutions of the cerebral hemispheres differ from individual to individual, their number is normally unchanged. Every person, regardless of age and gender, has the following grooves:
- Sylvian fissure - separates the frontal lobe from the temporal lobe;
- lateral sulcus - separates the temporal, parietal and frontal lobes, and is also one of the deepest in the brain;
- Roland's fissure - separates the frontal lobe of the brain from the parietal lobe;
- parieto-occipital sulcus - separates the occipital region from the parietal;
- cingulate sulcus - located on the medial surface of the brain;
- circular - is the boundary for the insular part on the basal surface of the cerebral hemispheres;
- The hippocampal sulcus is a continuation of the cingulate sulcus.
The relief of the cerebral cortex is very complex. It consists of numerous convolutions of different shapes and sizes. But we can highlight the most important of them, which perform the most important functions. The main convolutions of the brain are presented below:
- angular gyrus - located in the parietal lobe, involved in recognizing objects through vision and hearing;
- Broca's center - the posterior part of the inferior frontal gyrus on the left (in right-handers) or on the right (in left-handers), which is necessary for correct speech reproduction;
- Wernicke's center - located in the posterior part of the superior temporal gyrus on the left or right (similar to Broca's area), is involved in the understanding of oral and written speech;
- cingulate gyrus - located on the medial part of the brain, takes part in the formation of emotions;
- hippocampal gyrus - located in the temporal region of the brain, on its inner surface, necessary for normal memorization;
- fusiform gyrus - located in the temporal and occipital regions of the cerebral cortex, is involved in face recognition;
- lingual gyrus - located in the occipital lobe, plays an important role in processing information coming from the retina;
- precentral gyrus - located in the frontal lobe in front of the central sulcus, necessary for processing sensitive information entering the brain;
- postcentral gyrus - located in the parietal lobe behind the central sulcus, necessary for voluntary movements.
Activity rate
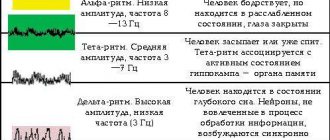
Diagnosis of the state of the brain, including the temporal lobe, is carried out using an electroencephalogram. The rhythm of neuron activity reflects the state of its individual sections.
In a normal state, indicators should be within certain norms.
For the temporal lobe, the main indicator is Kappa rhythm: the norm is within the range of 25 - 35 µV, with an amplitude from 5 to 40 µV. Alpha rhythms: from 8 to 14 Hz, within, amplitude up to 100 μV. Beta rhythm: normal amplitude 3 – 7 µV.
The pathological condition is shown by: Theta waves with a frequency from 4 to 7 Hz and Delta waves with activity: frequency from 1 to 3 Hz (amplitude over up to 40 μV).
MRI scanning allows you to determine the presence of cysts, neoplasms, enlargement or reduction of certain lobes of the temporal cortex.
These examinations confirm or refute the diagnosis.
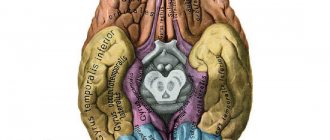
Anatomical parts of the brain
There are 5 separate anatomical parts of the brain, which were formed phylo-ontogenetically in different ways. Let's start with the oldest parts, gradually moving to the younger parts of the brain.
- Temporal lobe of the brain: structure and functions
- The structure of the hemispheres
- Sinuses and processes of the dura mater of the brain
- Frontal
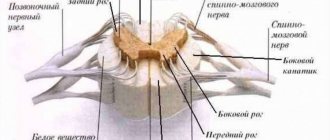
Medulla
This is the most ancient part of the brain, which is a continuation of the spinal cord. The gray matter here is presented in the form of the nuclei of the cranial nerves, and the white matter forms the pathways up and down.
Here are important subcortical centers for coordination of movements, regulation of metabolism, balance, breathing, blood circulation, and protective unconditioned reflexes.
Back of the brain
Includes the pons and cerebellum. The cerebellum is also called the small brain. It is located in the posterior cranial fossa and weighs 120-140 grams. It has 2 hemispheres, which are connected to each other by a worm. The bridge looks like a thick white cushion.
The hindbrain regulates balance and coordination in humans. There are also a large number of nerve pathways that carry information to the higher and lower centers.
Midbrain
Consists of 2 upper (visual) tubercles and 2 lower (auditory). Here is the center that is responsible for the reflex of turning the head in the direction of noise.
Divisions of the brain
Intermediate part
It includes the thalamus, which acts as a kind of mediator. All signals to the cerebral hemispheres pass only through the thalamic pathways. The thalamus is also responsible for adaptation of the body and all types of sensitivity.
The hypothalamus is a subcortical center that regulates the activity of the autonomic nervous system, and therefore all internal organs. It is responsible for sweating, thermoregulation, lumen and tone of blood vessels, respiratory rate, heartbeat, intestinal peristalsis, formation of herbal enzymes, etc. This part of the brain is also responsible for the body’s sleep and wakefulness, eating behavior and appetite.
In addition, it is the central organ of the endocrine system, where nerve impulses from the cerebral cortex are transformed into a humoral response. The hypothalamus regulates the functioning of the pituitary gland by producing releasing factors.
Terminal (cerebral hemispheres)
These are the right and left hemispheres, which are united into one whole by the corpus callosum. The telencephalon is the most recent part of the human brain in evolutionary terms and occupies up to 80% of the total mass of the organ.
Important Tsipramil: instructions for use, analogues, cost, reviews
The surface has a large number of convolutions and grooves, which are covered with cortex, where all the higher centers for regulating the body’s activities are located.
The hemispheres are divided into lobes - frontal, parietal, temporal and occipital. The right hemisphere is responsible for the left side of the body, and the left hemisphere is responsible for the opposite. But there are centers that are localized only in one part and are not duplicated. As a rule, for right-handers they are located in the left hemisphere, and for left-handers, vice versa.
Links[edit]
- ROSA LAFER-Souza and Bevil Conway (October 20, 2013). "Parallel, multistage processing of colors, faces, and shapes in macaque inferior temporal cortex". The Nature of Neuroscience. Retrieved October 1, 2021.
- Haxby points out that several studies have found face perception in the inferior temporal sulcus with most sites in other parts of the brain: page 2, Haxby, et.al. (2000) "A distributed human neural system for face perception" Trends in Cognitive Science 4 (6) June 2000, 11 pp.
- BRUCE Goldman (April 16, 2013). "Scientists identify brain region for number recognition". Stanford School of Medicine. Retrieved April 30, 2013.
- ^ a b Kolb, B; Whishaw, I. Q. (2014). Introduction to Brain and Behavior
(Fourth ed.). New York, NY: Worth it. pp. 282–312. - Jump up
↑ Gross, C. G. (2008).
"Inferior temporal cortex". Scholarpedia
.
3
(12): 7294. Bibcode: 2008SchpJ...3.7294G. DOI: 10.4249/scholarpedia.7294. - Pessoa, L., Tootell, R., Ungerleider L.G., Squire, L.R., Bloom, IP, McConnell, S.K., Roberts, J.L., Spitzer, N.C., Zsigmond, M. J. (Ed.) (2008). "Visual perception of objects." Fundamental Neuroscience
(Third Edition).CS1 maint: multiple names: authors list (link) CS1 maint: additional text: authors list (link) - Denis, Catherine; Wim Vanduffel; Denis Fiese; Koen Nelissen; Hendrik Peuskens; David Van Essen; Guy A. Orban (10 March 2004). "Visual shape processing in the cerebral cortex of humans and non-human primates: a functional magnetic resonance imaging study". Journal of Neuroscience
.
24
(24(10):2551–2565):2551–2565. DOI: 10.1523/JNEUROSCI.3569-03.2004. PMC 6729498. PMID 15014131. - Kolb, Brian; Whishaw, Ian K. (2014). Introduction to Brain and Behavior
(Fourth ed.). New York, NY: Worth it. pp. 282–312. - Mishkin, Mortimer; Ungerleider, Leslie G. (1982). "Two Cortical Visual Systems" (PDF). MIT Press. Cite journal requires |journal= (help)
- Creem, Sarah H.; Proffitt, Dennis R. (2001). "Defining Cortical Visual Systems: 'What', 'Where' and 'How'" (PDF). Acta Psychologica
.
107
(1–3): 43–68. DOI: 10.1016/s0001-6918(01)00021-X. PMID 11388142. - Jump up
↑ Gross, C. G. (2007).
"Single neuron studies of the inferior temporal cortex". Neuropsychology
.
46
(3):841–852. DOI: 10.1016/j.neuropsychologia.2007.11.009. PMID 18155735. - Dragoi, Valentin. "Chapter 15: Visual Processing: Cortical Pathways". Archived from the original on April 9, 2014. Retrieved November 12, 2013.
- Gross, Charles (2008). "Inferior temporal cortex". Scholarpedia
.
3
(12): 7294. Bibcode: 2008SchpJ...3.7294G. DOI: 10.4249/scholarpedia.7294. - Spiridon, M.; Fischl, B.; Kanwisher, N. (2006). "Location and spatial profile of categorical regions in human extrastriate cortex". Mapping the Human Brain
.
27
(1):77–89. DOI: 10.1002/hbm.20169. PMC 3264054. PMID 15966002. - Denis; and others. (March 10, 2004). "Visual shape processing in human and nonhuman primate cerebral cortex: a functional magnetic resonance imaging study" (PDF). Journal of Neuroscience
: 2551–2565. - Nakayama, Ken. "Research on Prosopagnosia". President and Fellows of Harvard College. Retrieved November 9, 2013.
- ↑
Gross, Charles (January 29, 1992).
"Representation of visual stimuli in inferior temporal cortex" (PDF). Philosophical Transactions: Biological Sciences
.
Face image processing. 335
(1273):3–10. DOI: 10.1098/rstb.1992.0001. PMID 1348134. Retrieved November 9, 2013. - Jump up
↑ Meadows, J. C. (1974).
"Anatomical basis of prosopagnosia". Journal of Neurology, Neurosurgery and Psychiatry
.
37
(5):489–501. DOI: 10.1136/jnnp.37.5.489. PMC 494693. PMID 4209556. - Purves D, Augustine, Fitzpatrick et al...editors (2001). "Lesions in cortical temporal association: recognition deficits". Neurology
(2nd ed.). Retrieved November 11, 2013.CS1 maint: uses authors parameter (link) - ^ a b Chan, D; Fox NC; Crum WR; Whitwell JL; Leschziner G; Rossor AM; Stevens J.M.; Cipolotti L; Rossor M.N. (April 2001). "Patterns of temporal lobe atrophy in semantic dementia and Alzheimer's disease." Annals of Neurology
.
49
(4): 433–42. CiteSeerX 10.1.1.569.8292. DOI: 10.1002/ana.92. PMID 11310620. - Haywood, California; Gaffan D; Cowie A. (1995). "Cerebral achromatopsia in monkeys" (PDF). European Journal of Neurobiology
.
7
(5):1064–1073. DOI: 10.1111/j.1460-9568.1995.tb01093.x. PMID 7613611. Retrieved November 11, 2013.
Temporal lobe of the brain: structure and functions
The temporal lobe of the dominant hemisphere of the brain is responsible for:
- word recognition;
- operates with long-term and medium-term memory;
- is responsible for assimilation of information while listening;
- analysis of auditory information and partially visual images (in this case, perception combines the visible and audible into a single whole);
- has a complex memory that combines the perception of touch, hearing and vision, while inside a person there is a synthesis of all signals and their correlation with the object;
- responsible for balancing emotional manifestations.
The temporal lobe of the non-dominant hemisphere is responsible for:
- facial expression recognition;
- analyzes speech intonation;
- regulates the perception of rhythm;
- responsible for the perception of music;
- promotes visual learning.
Left temporal lobe and its damage
The left lobe, usually the dominant lobe, is responsible for logical processes and contributes to understanding about language processing. She is assigned the role of controlling character, remembering words, and is associated with short-term and long-term memory.
If a disease or damage is localized in the temporal lobe of the brain of the dominant hemisphere, this is fraught with consequences such as:
- self-aggression;
- the development of melancholy, which manifests itself in endless pessimism, thoughts of meaninglessness and negativity;
- paranoia;
- difficulties in composing phrases during speech, choosing words;
- difficulties in analyzing incoming sounds (inability to distinguish crackling from thunder, etc.);
- reading problems;
- emotional imbalance.
Activity rate
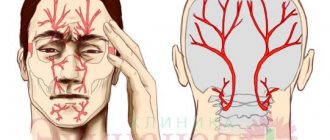
As you know, the temporal lobe is located at the level of the imaginary arch of glasses - that is, on a line below the level of the ears. The temporal lobes, combined with the activity of the limbic system, make life emotionally rich.
Their unity allows us to talk about the emotional brain, which is known for passionate desires and sublime experiences. These experiences make us feel the peak of pleasure or leave us in deep despair.
Normally, with balanced activity of the temporal lobes and limbic system, a person has full self-awareness, relies on personal experience, experiences a variety of uniform emotions, is inclined to experience spiritual experience, and is aware of everything. Otherwise, all of the listed activities of the human brain will be disrupted, and, therefore, problems in communication and everyday life will not be avoided.
Damage to the non-dominant hemisphere
The peculiarity of the location of the temporal lobes is the reason why this part of the brain is so vulnerable.
Emotional intelligence makes life meaningful and colorful, but once it gets out of control, cruelty, pessimism and oppression emerge from the depths of consciousness, threatening us and others.
Emotional intelligence is the most important element of the operating system of our Self.
In psychiatry, illnesses associated with these areas of the brain are called temporal lobe epilepsy, but in addition, disruption of the activity of these areas of the brain can explain many irrational manifestations of personality and, unfortunately, religious experience.
Neuropsychological syndromes with damage to the temporal regions of the brain
The temporal regions of the brain, representing a system related to the auditory analyzer, are characterized in the same way as other modality-specific structures by the presence of primary
and
secondary
zones.
At the same time, the structure and functions of the temporal regions of the brain are quite complex; they include the so-called extranuclear zones and provide not only auditory analysis and synthesis itself, but also other forms of mental reflection. It should also be noted that the medial
The surface of the temporal lobes of the brain is part of the limbic system, which is involved in regulating the sphere of needs and emotional processes. included in memory processes and providing activation components of brain function.
A special place in the structure and function of the temporal regions is occupied by areas adjacent to the convexital parieto-occipital regions. The complexity of the structure and function of the temporal systems is also determined by the variety of their connections with other parts of the cortex and subcortical formations.
All of the above determines the variety of symptoms of violation of higher mental functions with damage to various parts of the temporal region and not only related to acoustic-perceptual functions.
Currently, there is every reason to identify the following syndromes of damage to the temporal structures:
:
- lateral,
- medial and
- basal in terms of interhemispheric asymmetry and interhemispheric interaction.
a) Neuropsychological syndromes of damage to the lateral parts of the temporal region.
Assessing the function of the secondary sections of the temporal cortex, A. R. Luria states that they “play a decisive role in the differentiation of both complexes of simultaneously presented auditory stimuli and successive series of pitch relations or rhythmic sound structures” (A. R. Luria, 1973. P. 150).
When the secondary parts of the temporal region are damaged, a syndrome of auditory, acoustic agnosia
in speech (left hemisphere) and non-speech (right hemisphere) spheres.
Speech acoustic agnosia
is well described in a number of fundamental works as sensory aphasia, which is based on
a violation of phonemic hearing
- a factor that provides a differentiated analysis of meaningful speech sounds.
The severity of the impairment in distinguishing speech sounds can be:
- maximum (differentiation of all speech sounds is impaired),
- medium (distinction between close phonemes is impaired) and
- minimal (while the analysis of phonemes is intact, the perception of pairs of words that differ only in one phonemic feature, as well as words that are rarely used or have a complex sound composition, is defective).
Despite the fact that the central symptom is impaired speech understanding
, perceived by ear, the speech deficit is systemic in nature and is found not only in the impressive, but also in the
expressive
speech of the patient, which in the most pronounced variants of the syndrome has the character of a “verbal okroshka”. The speech of such patients consists of a set of syllables, as well as individual speech structures such as introductory words, interjections and emotional exclamations. It is important to note that in this case, the expressive components of speech (intonation, gestures, facial expressions, focus on dialogue) can remain intact.
In milder cases of dysfunction of the secondary parts of the temporal region, impaired understanding
manifests itself in the phenomenon of “
alienation” of the meaning of a word
when its sound shell is correctly reproduced, and in expressive speech there are difficulties in selecting words when constructing a statement, and a violation of the nominative function of speech.
In tests for naming visually presented objects, patients experience difficulties in updating the name of the object, which are characterized by:
- or by lengthening the latent period when selecting the desired name,
- or literal paraphasias
, i.e. replacing the name word with another that is similar in sound to the desired one.
Previously, it was mentioned about the violation of the nominative function of speech in amnestic aphasia in the syndrome of damage to the TPO zone.
A technique that allows you to differentiate naming difficulties
for amnestic and sensory aphasia, the patient is prompted by the examiner pronouncing the initial sounds of the word.
The fact that the violation of the nomination in the structure of temporal syndrome is associated with the search for the sound image of the word
is evidenced by the need for a very deep hint, often covering the entire sound range in a given word, except for the ending. And even such a deep hint does not always help the patient, provoking him to paraphasia or agrammatism. In contrast, in amnestic aphasia, a prompt helps “get right away.”
The so-called verbal deficit also affects the processes of discursive (logical) thinking
due to difficulties in understanding and comprehending verbal material.
The process of understanding when reading is disrupted
.
Dictation writing can be especially disruptive.
due to a defect in the analysis of the sound composition of words.
As mentioned above, the sensory-speech defect is, according to most authors, strictly lateralized in relation to the left
hemispheres of the brain. However, recently there has been evidence that the right hemisphere also contributes to the process of perception of speech stimuli, but not at the level of analysis of the linguistic characteristics of speech sounds, but at the level of the actual acoustic phonetic features (Yu. V. Mikadze, B. S. Kotik, 1962, In the book A. R. Luria and modern neuropsychology).
Right-handed
lesions in the secondary parts of the temporal region are characterized by defects in acoustic analysis and synthesis in
the non-speech sphere
. These include:
- violation of identification of household noises,
- impairment of perception and reproduction of melodies (expressive and impressive amusia),
- violation in identifying voices by gender, age, familiarity, etc.
The functions provided by the joint work of the temporal regions of the right and left hemispheres of the brain include acoustic analysis of rhythmic structures
:
- perception of rhythms,
- their retention in memory and
- reproduction by sample.
As is known, to assess the state of this function, the so-called auditory-motor coordination test is used. It seems no coincidence that A. R. Luria designated this test, where the gnostic and motor links are in an inextricable connection and unity. The motor component is present not only at the stage of the actual performance, but is also included in the process of perception (Korsakova, Moskovichiute, 1965), just as at the stage of reproducing rhythms, the participation of the acoustic link is necessary (retrieval of a stimulus series from memory and auditory control aimed at adequate updating given rhythmic structure). We specifically devote space here to auditory-motor coordination, since recently in the practice of neuropsychology they have come to be called “rhythm testing” with an emphasis on the acoustic-gnostic component in this activity. It must be emphasized that the so-called acoustic analysis of rhythms is a much more complex activity, not only because of its deep connection with the motor system, but also with a broader and more complex complex of rhythmic and oscillatory processes in the body and nervous system, regulated, among other things, by phylogenetically ancient subcortical structures of the brain. Obviously, therefore, impairments in performing this test are quite variable with different localizations of the pathological process, and the full neuropsychological qualification of these impairments still awaits systematic study.
Before moving on to the analysis of violations of the reproduction of rhythmic structures, we note that the following characteristics are subject to assessment:
- volume of quantitative structure of a rhythmic series (how many beats in a rhythmic cycle),
- complexity of the structure (simple beat packs, accented rhythms, double rhythmic cycles, etc.) and
- reproduction by sample and
- according to the instructions.
It is also important that the perception of a rhythmic series is always the perception of a holistic
structure, regardless of the complexity or simplicity of its internal organization.
If the left
the temporal region primarily suffers from
acoustic analysis and synthesis
of the internal structure of the rhythm; therefore, the more complex (accented, double) the series is to be memorized and reproduced, the greater the likelihood of errors in its execution, and not only in execution according to the model, but also according to the instructions. In this case, the assessment of the volume of the rhythmic cycle is not rough, although it may be characterized by instability. And yet, even erroneous reproduction of rhythms in case of left hemisphere lesions shows that the stimulus material is reflected by the patient as an integral structure.
In contrast, with right hemisphere
in the foci, first of all, the perception of the structural design of the rhythmic cycle as a whole is disrupted.
This is manifested in a pronounced impairment in the assessment of rhythmic structure by the type of narrowing of the volume of perception
- a disorder specific to damage to the right hemisphere, including in relation to acoustic stimuli. This is also evidenced by the presence of dissociation between the reproduction of simple unstructured and structured rhythmic series. Structurally designed rhythm packs are better reproduced compared to simple ones. It is interesting that the reproduction of rhythms according to instructions in patients with right-hemisphere lesions in the temporal region is often replaced by the actualization of an undifferentiated series, which also suggests the difficulty of forming a reproducible series of tappings as an integral structure.
Lateralization – Conclusions:
Thus, syndromes of damage to the secondary zones of the auditory analyzer, generally characterized as acoustic agnosia
, have distinct signs associated with the lateralization of the lesion.
Left
The hemisphere is manifested by a violation of speech and related processes (
sensory aphasia
), as well as a violation of the perception and reproduction
of rhythmic
structures.
Right
– impaired perception
of non-verbal
acoustic material.
It should be noted that by now there is an accumulation of facts working in favor of the concept of interaction of the hemispheres in both verbal and non-verbal auditory gnosis, which are still at the level of experimental research and are not included in the range of diagnostic neuropsychological clinical data.
b) Neuropsychological syndrome of damage to the “extranuclear” convexital parts of the temporal lobes of the brain.
One of the main features of the operation of the auditory analyzer, which is especially significant for understanding the nature of speech disorders and distinguishes it from other analytical systems, in particular visual, is associated with the specific organization of acoustic information, the perception of which requires the translation of successively arriving stimuli in the form of a sequence of sounds into a simultaneous scheme.
Thus, the perception of a sound series is based not only on the analysis of individual elements of the acoustic flow, but also on the retention of all its links in memory. In this regard, it becomes clear that there is a need for devices in the acoustic perception system to retain in memory the entire sequence of sounds in order to understand the meaning of non-verbal acoustic stimuli or the meaning of the perceived utterance. When these devices are damaged, the following occurs:
- Acoustic-mnestic aphasia syndrome
(
left
hemisphere) and - disorders of auditory non-verbal memory
(
right
hemisphere of the brain).
At the center of the acoustic-mnestic aphasia
There are
violations of auditory-verbal memory
, i.e. defects in memorizing verbal material presented aurally, while it is possible to reproduce the same stimuli presented visually. In essence, we are talking about a modality-specific memory impairment within a given analyzer. They manifest themselves in a narrowing of the volume of direct reproduction significantly below normal.
Thus, when presented with a series of 4 words, the patient reproduces 1-2 words. It is characteristic that, as a rule, the first or last elements of the series are reproduced, i.e., the “edge factor” is clearly expressed.
Similar difficulties (narrowing of the scope of reproduction) can be seen when memorizing phrases and stories.
An important diagnostic criterion is the lack of increase in reproduction productivity during memorization, which in some cases can lead to depletion of the function and deterioration of the initially achieved indicators.
Modality-specific impairments in auditory-verbal memory appear especially clearly under conditions of interfering
activities that fill the short time interval between memorization and reproduction (for example, a short conversation with a patient).
The basis for impairment of auditory-verbal memory is changes in neurodynamic
parameters of the analyzer in the form of pathological retro- and proactive inhibition and equalization of excitability.
The inhibition of auditory-verbal traces manifests itself not only in connection with the introduction of a special interfering task, but also as a result of the mutual influence of the elements of the acoustic sequence on each other (intra-stimulus interference), leading to a narrowing of the volume
direct playback.
The mechanism of equalization of excitability causes the occurrence of paraphasia
when the patient reproduces verbal material, i.e., the replacement of stimulus elements with words,
- similar in sound (literal paraphasias) or
- by meaning (verbal paraphasias).
In conclusion, the description of auditory-verbal memory disorders should be noted that the degree of their severity depends on the nature
memorized material. Verbal material, united by internal semantic connections (phrases, stories), is remembered by patients more easily than a series of words that are not related to each other. But even within semantic information, the factor of its volume plays a role: phrases are reproduced better than stories.
Why are these disorders considered within the framework of the syndrome of speech disorders (aphasia)?
The fact is that,
- Firstly, a deficit of auditory-verbal memory can lead to disruption of the patient’s understanding of speech addressed to him, verbal instructions, and a sharp limitation in the ability to operate with auditory-verbal material “on the spot”.
- Secondly, with an increase in verbal “load” in the form of an increase in the volume of auditory material, symptoms characteristic of sensory aphasia may arise: alienation of the meaning of the word and errors in the differentiation of phonemes. For example, the instruction to show parts of the body (“nose”, “eye”, “ear”) is correctly performed by the patient with a single presentation of verbal equivalents, and in tasks that require maintaining the display sequence (show “ear-nose-eye”), with its correct repetition causes errors in identifying the corresponding parts of the body.
Damage to the symmetrical parts of the right
hemispheres of the brain leads to memory impairment for
non-speech
and
musical
sounds, which manifests itself in difficulties in memorizing rhythmic structures with an increase in the volume of elements contained in them and the number of groupings, as well as in the inability to reproduce a given melody.
At the same time, processes associated with speech activity also suffer: the perception of intonation
components, determining
whether a voice belongs
to a person of a certain gender and age. The possibility of individual identification of voices is impaired.
Differential diagnosis:
The interaction of the cerebral hemispheres is manifested here in the organization of auditory-verbal memory. The test
, which tests the ability to reproduce the order of elements in a verbal sequence.
When performing a task to reproduce a series of 5 words, patients with damage to the temporal regions of the right
hemisphere of the brain at the first reproduction exhibit difficulties that are outwardly similar to the narrowing of the volume of direct reproduction in acoustic-mnestic aphasia.
Repeated
presentation of the material (learning) shows several clear differences in these initially similar-looking symptoms.
Firstly, incomplete reproduction in right-hemisphere patients is extremely rarely represented by the “edge factor”; the actualized words do not correspond to their position in the series and the order of occurrence.
Secondly, memorization can lead to complete reproduction of a given volume (unlike left-hemispheric lesions), but learning the sequence of words in a series significantly lags behind the task in terms of volume. In a significant number of cases, it is not possible to obtain stable reproduction at all.
Thirdly, the introduction of an interfering task does not lead to a decrease in the achieved level of reproduction.
Fourthly, the patient is often unable to give an answer after the first presentation of a series of words, how many elements it consists of, while a patient with left hemisphere
the focus, as a rule, controls the overall structure of the verbal series.
Possible mechanism
, which underlies the described variant of auditory-verbal memory impairment in patients with damage to the temporal regions
of the right
hemisphere of the brain, is the insufficiency of direct memorization, the formation of a “perceptual scheme” of the memorized stimulus material. It is interesting that this defect can be overcome if the presented words are either divided intotonationally into groups (“house-forest-cat” - pause - “night-ringing”), or the inter-stimulus intervals are increased.
The assumption of a violation of the simultaneous “grasping” of the integrity of the memorized structure is supported by the violation of the reproduction of the visually presented Ray-Taylor figure. In this sense, the defect in auditory-verbal memory in right hemisphere foci within the extranuclear parts of the temporal region is not modality-specific, but reflects one of the basic factors in mental activity provided by the right hemisphere - the simultaneity of perception and actualization
. However, it is important to note that the right hemisphere also contributes to the organization of the verbal-mnestic function at a certain stage of its development.
c) Syndromes of damage to the medial temporal region.
Syndromes of damage to the medial temporal region have not been studied and described fully. As already mentioned, this area of the brain is related, on the one hand, to such basal functions in brain activity and mental reflection as
- emotional-need sphere and thereby –
- to the regulation of activity.
On the other hand, when these systems are damaged, disorders of the highest level of the psyche— consciousness—
, as a generalized reflection by a person of the current situation in its relationship with the past and future and of himself in this situation.
Clinical observations show that focal processes in the medial temporal lobes can manifest as affective disorders
by the type of exaltation or depression, as well as paroxysms of melancholy, anxiety, fear in combination with conscious and experienced vegetative reactions.
Often, as symptoms of irritation, disturbances of consciousness may occur in the form of absences
and such phenomena as “deja vu” and “jamais vu”, disturbances
in orientation in time and place
, as well as psychosensory disorders in the auditory sphere (verbal and non-verbal
auditory deceptions
, usually with critical attitude towards them on the part of the patient), distortion of taste and olfactory sensations. All these symptoms can be identified in a conversation with the patient and in observing his behavior and emotions during the examination.
The only systematically (clinically and experimentally) studied disorder associated with pathology of the medial temporal region is memory impairment.
The development of these ideas was largely facilitated by data obtained during operations on the medial temporal structures aimed at the surgical treatment of severe forms of epileptic disease.
Memory impairment in this syndrome is characterized by the following symptoms.
- They have a modally nonspecific character,
- proceed according to the type of anterograde amnesia (memory of the past remains relatively intact),
- combined with disturbances in orientation in time and place.
In the vast majority of cases, they are similar to those described by S. S. Korsakov and are designated as amnestic (or Korsakovsky) syndrome
. Patients are aware of their defect and strive to compensate for it by actively using the recording system.
A clinical experimental study of the structure and mechanisms of amnestic syndrome in this localization shows that the volume of direct memorization in these patients corresponds to the lower limit of the norm and amounts to 5-6 elements; with memorization, their number may increase. The learning curve for 10 words has a visible tendency to rise, although the learning process is extended over time and the level of achievement may fluctuate. Patients can hold a series of 4-5 elements during an empty pause of 2 minutes. Over time, patients begin to recognize the attending physician and remember the procedures or examinations they underwent. These facts indicate that the process of fixing information in memory is relatively preserved
.
At the same time, distinct difficulties in reproducing current events and experimental material are revealed, which are easily objectified when an interfering task is introduced between memorization and reproduction, the negative impact of which depends on its content.
For example, when memorizing a sequence of words after its immediate reproduction, you can ask the patient several arithmetic examples (heterogeneous interference), name several words starting with the letter “k” (homogeneous interference based on the similarity of the verbal content of the material being learned and the interfering activity).
Finally, after memorizing one series of words, it is proposed to remember a similar second series (homogeneous interference, similar to primary memorization both in content and in the mnestic task).
In all cases, after interfering activity, reproduction will be deficient
, and the forgetting will be the deeper, the more homogeneous in its content and task the interfering activity with the preceding memorization is.
Interfering activity carried out in the delay interval between memorization and reproduction has an inhibitory, blocking effect on the actualization of the material just memorized.
Clinical and experimental data allow us to speak about the main mechanism of the formation of amnestic syndrome with damage to the medial parts of the temporal systems of the brain - pathological inhibition of traces
interfering influences, i.e. consider memory impairment in connection with changes
in the neurodynamic parameters
of brain activity towards the predominance of
inhibitory
processes.
It is characteristic that when this level is damaged, memory impairments appear in a “pure” form without involving side elements in the reproduction product. The patient either names several words available for actualization, noting that he forgot the rest, or says that he forgot everything, or amnesizes the very fact of memorization preceding the interference. This feature indicates the preservation of control over reproduction activities. In addition to the sign of modal nonspecificity, the described memory disorders are characterized by the fact that they “capture” various levels of semantic organization of the material (series of elements, phrases, stories), although semantic structures are remembered somewhat better and can be reproduced with the help of hints. In some cases, a story can be reproduced better than a series of words or a phrase, especially if the patient understands its meaning well (compare with auditory-verbal memory impairments).
Lateralization:
Within the framework of the study of this syndrome, one significant question remains unresolved: is it the result of bilateral or unilateral damage to the medial temporal region?
There is reason to consider it as a consequence of a bilateral pathological process. However, these grounds are not 100% valid. We can only recommend not limiting ourselves to the study of mnestic disorders, but looking for (or excluding) signs of unilateral deficits in other mental processes.
d) Syndromes of damage to the basal parts of the temporal region.
The most common clinical model of the pathological process in the basal parts of the temporal systems is tumors of the wings of the sphenoid bone in the left or right hemispheres of the brain.
Left-handed
the localization of the focus in this case leads to the formation of
a syndrome of auditory-verbal memory disorders
, which differs from a similar syndrome in acoustic-mnestic aphasia. This difference concerns two components of the latter:
- speech
itself and - narrowing the volume
of auditory-speech perception.
When the temporobasal regions are damaged, the main radical that determines the nature of memory disorders is increased inhibition of verbal traces by interfering influences under conditions of homogeneous interference
, i.e., when memorizing and reproducing two “competing” rows of words, two phrases and two stories.
There is no noticeable narrowing of the volume of auditory-speech perception, as well as signs of aphasia. At the same time, in this syndrome there are signs of inertia in the form of repetition when reproducing the same words. In tests for the reproduction of rhythmic structures, patients have difficulty switching when moving from one rhythmic structure to another; Perseverative performance is observed, which, however, can be corrected. It cannot be excluded that pathological inertia in this case is associated with the influence of the pathological process either on the basal parts of the frontal lobes of the brain, or on the subcortical structures of the brain, especially since with this localization the tumor can disrupt blood circulation precisely in the system of subcortical zones.
Damage to the basal-temporal regions in the right
cerebral hemisphere manifests itself in difficulties in reproducing the order of elements and corresponds to the disorders described above (b), which manifest themselves here only in a milder form.
Concluding the description of the pathology associated with damage to various parts of the temporal systems of the brain, we should dwell on two important points in the diagnostic aspect.
The deep location of the pathological focus in the temporal regions of the brain reveals itself not so much as a primary disorder, but as a disorder in the functional state of the systems included in the temporal zones, which in the situation of a clinical neuropsychological examination manifests itself in the partial exhaustion of the functions associated with these zones. For example, testing phonemic hearing can reveal its preservation when performing the first two or three differentiations. However, continuing to perform this task causes errors in the differentiation of phonemes. In fact, in conditions of depleted function, genuine disorders of phonemic hearing arise, which cannot be considered as a result of cortical insufficiency itself, but must be interpreted in connection with the influence of a deeply located focus on the secondary parts of the temporal region of the left hemisphere of the brain. Similarly, with deep-seated tumors, other symptoms characteristic of the described syndromes of focal pathology in the temporal regions of the brain may appear. The dissociation between the initially available test performance and the appearance of pathological symptoms during the period of “load” on the function gives grounds for the conclusion about the predominant influence of a deep-lying focus on convexital, medial or basal structures in the left or right hemispheres of the temporal regions of the brain.
The second important remark in the diagnostic aspect concerns the difficulties of determining the local zone of damage to the right temporal lobe. It must be borne in mind that, as shown in a number of studies, the right hemisphere, compared to the left, reveals less pronounced differentiation of structures in relation to individual components of mental functions and the factors that ensure them. In this regard, the interpretation of syndromes and their component symptoms obtained during a neuropsychological examination in a narrow local sense should be more careful.
The structure of the hemispheres
The outside of the hemispheres is covered with a cortex (a plate of gray matter). They have 3 surfaces: superolateral, medial (middle) and inferior. The surfaces are separated by edges.
The hemispheres have poles: frontal, occipital and temporal.
There are grooves on all surfaces of the hemispheres, except the lower one. They can be deep or shallow, have an irregular shape and can change their direction. Each hemisphere is divided into lobes by deep grooves.
The following types of shares are distinguished:
- frontal;
- occipital;
- parietal;
- insular;
- temporal
Frontal lobe
It is located in the anterior sections of both hemispheres and is limited by the pole of the same name, the lateral and central sulci.
The central sulcus (Roland's) begins on the median surface of the hemisphere and is directed towards its upper edge. Then it goes downwards, but does not reach the lateral sulcus.
The precentral sulcus is located parallel to the central sulcus. From it go upward 2 frontal sulci - superior and inferior, which divide the frontal lobe into convolutions.
The convolutions separate the small grooves from each other. The frontal lobe has 3 gyri - superior, middle and inferior. Broca's center is located in the area of the inferior gyrus. Its significance is great. He is responsible for interpreting the meaning of speech, syntactically forming sentences and arranging words in them. The frontal lobe consists of 3 parts - triangular, orbital and tegmental.
Important Effectiveness of bioacoustic brain correction
Functions of the frontal lobe:
- thinking;
- regulation of behavior;
- conscious movements;
- physical activity;
- speech function;
- handwriting;
- memory center.
Parietal lobe
The parietal lobe is located behind the Rolandic fissure. Limited by the occipito-parietal and lateral sulci.
This lobe contains the postcentral sulcus, which runs parallel to the central sulcus. Between them is the postcentral gyrus. Heading towards the frontal lobe and connecting with the precentral gyrus, the paracentral lobule is formed. In addition to this lobule, the parietal lobe has the same superior and inferior lobules. The inferior parietal lobule has 2 gyri: supramarginal and angular.
Functions of the parietal lobe:
- deep and superficial sensitivity of the whole body;
- automatic movements provoked by constant repetitions (washing, dressing, driving, etc.);
- tactile function (the ability to recognize the size and weight of an object by touch).
Occipital lobe
It is located behind the parieto-occipital sulcus. Has a small size. The occipital lobe has grooves and convolutions that can change their shape and direction. The most pronounced are the calcarine and transverse grooves. The occipital lobe ends at the occipital pole.
Functions of the occipital lobe:
- visual function (perception and processing of information);
- perception of light.
Temporal lobe
The temporal lobe is separated from the frontal and parietal by the Sylvian fissure (lateral). The edge of this lobe covers the side of the insula and is called the temporal operculum. The temporal lobe has a pole of the same name and 2 convolutions of the same name - superior and inferior. It also contains three short convolutions, which are located in the transverse direction - Heschl’s convolutions. Wernicke's center is located in the temporal lobe, which is responsible for giving meaning to our speech.
Functions of the temporal lobe:
- perception of sensations (hearing, taste, smell);
- sound and speech analysis;
- memory.
Insula
Located in the depths of the Sylvian fissure. It can only be seen if you expand the operculum (temporal, frontal and parietal lobes). It has a circular sulcus, a central sulcus, a long and a short gyrus.
The main function of the insula is taste recognition.
The following structures are located in the medial region of the hemispheres:
- grooves: corpus callosum; hippocampus; waist
- gyri: parahippocampal, dentate, cingulate, lingual.
On the lower surface of the hemispheres there are olfactory bulbs, grooves and pathways. In addition, there are the nasal sulcus, the uncus (the end of the parahippocampal gyrus), the occipitotemporal gyrus and the sulcus.
The olfactory bulb, tract, triangle, substantia perforatum, cingulate, parahippocampal, dentate gyrus and hippocampus form the limbic system.
The function of the limbic system is olfactory.
Cortex of the hemispheres
The cerebral cortex is gray matter located in the peripheral areas of the hemispheres. Its surface area is about 200 thousand mm2. The shape, appearance and location of neurons and other structures are different in different parts of the cortex and are called “cytoarchitecture”. The cerebral cortex contains the nuclei of cortical analyzers of all types of sensitivity: motor, cutaneous, auditory, olfactory and visual.
Sinuses and processes of the dura mater of the brain
The following are considered to be the processes of the dura mater:
- A large crescent-shaped continuation, or the crescent-shaped process of the largest hemispheres of the brain, is located between both large parts of the brain;
- A small falciform process, or a falciform process near the cerebellum, extends into the cavity between the cerebellar hemispheres, joining the bone tissue of the occiput from the internal occipital indentation to the large foramen of the occiput;
- Cerebellar tentorium - located between the parts of the cerebral hemispheres at the back of the head and the cerebellum;
- The plate is located above the sella turcica; in the middle there is a hole through which a funnel runs.
Sinuses (lacunae) of the dura mater of the brain, formed due to the splitting of the dura mater into two strands, are essentially channels through which blood from the veins is drained from the head into the internal dual veins.
The hard shell plates that form the lacunae are tightly reinforced and do not move. Therefore, these sinuses are visible in the section. They are not equipped with valves. This structure of these tanks allows venous blood to flow freely from the brain, completely independent of pressure surges inside the skull. On the inner walls of the bone tissue of the skull, in the areas where these recesses of the hard shell are located, there are proper tentories. In medical practice, the following names of the dura sinuses are used:
- The superior vertically dividing sinus is located longitudinally along the entire upper-outer border of the falx of the cerebral hemispheres, from the edge resembling the cockscomb of the ethmoid bone to the indentation of the occiput inside. In the anterior parts, this tank is equipped with anastomoses with veins of the paranasal space. Its termination at the rear is included in the transverse manifold.
- The lower vertically dividing lacuna is located inside the lower spacious border of the falx of the cerebral hemisphere. It is much smaller than the top one.
- The straight sinus is located vertically in the splitting of the cerebellar membrane in the direction of the attachment of the falx of the cerebral hemisphere to it. This collector combines the posterior ends of the superior and inferior sagittal sinuses.
- located in the part of the separation of the cerebellar plate from the dura mater of the brain. On the inner side of the scales of the bone tissue of the back of the head, an extensive groove of the transverse sinus is related to this depression.
- The occipital lacuna lies at the bottom of the cerebellar falx. Descending longitudinally from the inside of the occipital border, this tank is located to the posterior border of the large opening of the occiput, where it diverges into two grooves that frame this opening at the back and on both sides.
- The sigmoid collector is double, located in the sigmoid branch on the inside of the skull, characterized by an S-shaped appearance. In the area of the opening of the great veins, this tank flows into the jugular vein.
- The cavernous sinus is double and lies on the vault of the cranium away from the sella turcica. The carotid artery and some intracranial arteries pass through this cistern. The recess has a very intricate structure in the form of interconnected caves, which is why it got its name.
- The sphenoparietal lacuna is double, refers to the spacious posterior border of a small wedge-shaped bone fragment, in the cleft it connects in this place with the dura mater of the brain.
- The upper and lower stony recesses are double and lie longitudinally along the upper and lower borders of the triangle of bone tissue in the temporal region.
Important: What is the danger of ischemic cerebral stroke?
In some areas, all these cisterns form connections - anastomoses - with the external veins of the skull through connections of vessels. In addition, the sinuses of the TO connect to the diploic arteries, which are located in the spongy structure of the bones of the base of the skull and are included in the superficial vessels of the head. Thus, blood from the veins of the brain flows through the branches of its vessels located on the surface and in the depths into the sinuses of the brain and then into both internal large veins.