It is known that a person receives up to 85% of information about the environment through vision, and only the remaining 15% is hearing and other senses. The occipital lobe is the area responsible for the highest processing of visual signals. Thanks to it, healthy humanity is able not only to distinguish surrounding environmental objects by their visual characteristics, but also to contemplate the creations of artists, to create themselves. We can catch the mood of other people by observing the changes in their facial expressions, enjoy the beauty of the sunset, and, finally, choose food based on our favorite color.
- Location
- Functions
- What fields are included?
- Symptoms of the lesion
General information about the cisterns of the brain
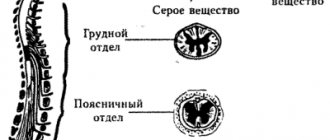
The meninges have a three-layer structure:
- hard, which is located directly next to the cranial bones;
- arachnoid;
- soft, which covers the brain.
Let's look at each of the layers in more detail:
- In the structure of the dura mater there are small processes that are designed to separate different parts of the brain. This layer fits tightly to the skull. The largest process is considered to be the one that divides the human brain into two equal hemispheres; in appearance it resembles a crescent. A special diaphragm is located at the top of the hard layer; it protects the brain from external damage.
- After the hard layer comes the arachnoid (arachnoid). It is very thin, but at the same time provides sufficient strength. Simultaneously connects to the hard and soft shell. This layer is intermediate.
- The soft shell, or as it is also called the soft leaf, envelops the brain itself.
Between the soft and arachnoid layers there is a subarachnoid cavity in which cerebrospinal fluid circulates. The spaces between the convolutions of the brain contain cerebrospinal fluid.
Cisterns are structures that are formed from depressions above the interarachnoid space.
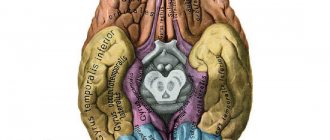
What fields are included?
The occipital lobe of the cerebral cortex contains:
- 17th field – accumulation of gray matter of the visual analyzer. This field is the primary zone. Consists of 300 million nerve cells.
- 18th field. It is also a nuclear cluster of the visual analyzer. According to Brodmann, this field performs the function of perceiving written speech and is a more complex secondary zone.
- 19th field. This field takes part in assessing the meaning of what is seen.
- 39 field. However, this brain area does not entirely belong to the occipital region. This field is located on the border between the parietal, temporal and occipital lobes. The angular gyrus is located here, and its list of tasks includes the integration of visual, auditory and general sensitivity of information.
Types of tanks, their characteristics, what they are responsible for
Let's look at the main types of tanks:
- The largest is considered to be the one located between the cerebellum and the medulla oblongata; it is called the magnum occipital;
- interpeduncular fills the area between the processes of the midbrain;
- the visual chiasm is surrounded by Cisterna chiasmatis, which runs along its frontal parts;
- the bypass is located in the space between the upper part of the cerebellum and the occipital lobes;
- The prepontine is located between the interpeduncular and cerebellocerebral. Located on the border of the subarachnoid region in the spinal cord;
- the basal cisterns include the interpeduncular and cross cisterns and form a pentagon;
- the bypass tank is located on the border of the interpeduncular, caudal and quadrigeminal (posterior part), has an unclear shape;
- The quadrigeminal cistern is located in the area of the corpus callosum and cerebellum. In its structure it has archanoid cystic formations, which cause dysfunction of the cranial nerve endings and pressure inside the skull;
- the superior cerebellar cistern covers the top and front of the cerebellum;
- The cistern of the lateral fossa is located in the lateral region of the cerebrum.
It should be noted that the cisterns are mainly located in front of the brain. They are connected to each other by the openings of Manaji and Lushka, the spatial openings are completely filled with cerebrospinal fluid.
If we consider the arachnoid layer using the example of a child’s body, we can say that it has a more delicate structure.
In newborn babies, the volume of the interarachnoid region is very large; it decreases as the child grows.
Changes in the occipital lobe in schizophrenia
The occipital lobe is known to be associated with vision. This triangular part of the brain is located behind the parietal lobe. The medial border of the occipital lobe is limited by the parieto-occipital sulcus. The lateral side is outlined by an imaginary line known as the parietotemporal lateral line (PO sulcus to the pre-occipital notch, parieto-temporal lateral line). The inferior tentorial surface is outlined by a line connecting the occipital sulcus with the beginning of the PO (parieto-occipital) sulcus. Three Brodmann areas (areas: 17, 18 and 19) are also located in the occipital lobe. On its medial surface there is a cuneus, a gyrus located between the calcarine groove and the PO sulcus. The lingual gyrus is noted on the tentorial surface of the occipital lobe (lower than the calcarine sulcus); this lingual gyrus is separated from the fusiform gyrus by a collateral groove. The fusiform gyrus is outlined laterally by the occipitotemporal sulcus.
A positive correlation was found between the frontal, temporal, and occipital regions and effective performance on tests of verbal intelligence quotient (IQ), verbal learning, and various executive functions. Diagnostic synergy was observed for the alliance between verbal IQ and the right temporo-occipital junction and left middle occipital gyrus. Another study showed an increase in activation in the left middle and superior occipital lobe.
Occipital epilepsy is not as common as other types of epilepsy. It is widely known among clinicians mainly due to its rarity (about 1.2-2.6% of all epilepsy cases). The hallmark of occipital seizures is visual hallucinations, but these are not present in every case of occipital epilepsy. Hallucinations typically initiate in the visual field contralateral to the affected visual cortex and then spread to cover the entire visual field. Transient visual symptoms, which may be commonly observed productive symptoms (eg, phosphenes and flares), as well as negative symptoms such as amaurosis, hemianopia, and scotoma, are commonly reported by patients here. Static or mobile outbreaks, which are productive symptoms, can be considered as a distinctive feature of the involvement of the occipital lobe in the pathological process. Visual hallucinations become vivid and complex if the pathological process is involved in the occipitotemporal cortex, and hallucinations with scenes of varying complexity are observed.
Compared with infarctions of other brain regions, occipital lobe infarctions differ in etiology, risk factors, and prognosis. Patients with occipital lobe infarcts typically have no other neurological symptoms other than visual loss in a specific field and are relatively milder than infarcts in patients with multiple infarcts or infarcts in other areas of the brain.
Patients with deep bilateral occipital injuries complain of complete loss of sleep. Moreover, the 'minimal lesion extension,' which is obligatory for Charcot-Wilbrand Syndrome (CWS), may be represented here by deep bilateral damage to the occipital lobe in the right lower lingual gyrus. CWS may represent a discrete and isolated neuropsychological symptom of deep occipital lobe damage and may occur even in the absence of documented REM sleep aberrations and other manifestations of cognitive deficits.
In the context of social perception, visual social information passes through the ventral stream during initial visual processing and is then sent to areas such as the prefrontal cortex when higher order cognitive processing is needed. Visual face processing occurs in the ventral tract (stream), and the location of activation is task dependent, indicating a hierarchical location of the ventral stream. The thalamus may be involved in visual processing of faces, along with the temporo-occipital cortex, fusiform, paracingulate and lingual gyri, while face and body stimuli also activate the superior temporal sulcus and middle occipital gyrus. The ventral stream may also be involved in the perception of emotional stimuli due to its significant connection with the amygdala. Thus, initial visual processing, emotional and social information is processed in the ventral stream in conjunction with the thalamus, temporal and occipital lobes.
Little is known about the association of schizophrenia with occipital lobe lesions. However, the association of visual hallucinations with damage to the occipital lobe in schizophrenia is beyond doubt. Still, open questions remain: do visual hallucinations intensify if the occipital lobe is damaged sufficiently; whether the entire occipital lobe in schizophrenia or some part of it is involved in the pathological process; if all lobes or structures of the brain are involved in the pathogenesis of schizophrenia, then what is the sequence of damage (the occipital lobe is damaged before other lobes or after their initial damage), can we prevent the involvement of the occipital lobe in the pathological process of schizophrenia or not?
Patients with schizophrenia had a decrease in the fractional anisotropy of the outer white matter scattered transversely in each hemisphere, particularly in the left temporal lobes and bilaterally in the occipital lobes compared with control subjects (fractional anisotropy varies by relatedness to the patient in both hemispheres and occipital and temporal regions).
There is ample evidence to support the notion that overall volume of the occipital lobe is reduced in patients with schizophrenia. Cranial asymmetry is able to predict increased prefrontal labeling in patients with schizophrenia. Comparison of microstructural diffusion parameters relative to the entire brain voxel map between schizophrenia in its deficit (SZD) and non-deficit (SZND) subtypes indicated that radial diffusivity was higher in the left forceps of patients with SZD, in the left internal capsule of patients with SZND and in the right lower fronto-occipital fasciculus in the entire schizophrenia group. The mean diffuseness was increased from healthy controls to patients with SZD and SZND in the right occipital lobe.
Long-term persistence of untreated psychosis was associated with decreased temporal and occipitotemporal gray matter volume in patients with newly treated schizophrenia. It was also found that patients with schizophrenia have significantly lower fractional anisotropy in the temporal (superior temporal and parafungiform) and occipital (superior and middle occipital) white matter compared to patients with bipolar disorder and healthy volunteers. In some patients with schizophrenia, there is an increase in gray matter density in the left occipital lobe and basal ganglia. Several authors have investigated the role of white matter DTI in early schizophrenia. They found a marked decrease in regional white matter functional anisotropy values in the right anterior and right middle occipital lobes.
In patients with schizophrenia, activity in the middle occipital gyrus decreases during decision making. There is moderate evidence that decreased functional activity in the right lingual gyrus during episodic memory encoding and decreased activation in the fusiform gyrus are observed during episodic memory retrieval in patients with schizophrenia compared with control groups.
Brain imaging of patients with schizophrenia demonstrates decreased activation during emotional processing tasks in the lentiform, fusiform, and middle occipital gyri. When solving unambiguous emotional problems, patients with schizophrenia experience a decrease in activation in the fusiform gyrus, and hidden emotion is associated with a decrease in the amount of activity in the middle occipital gyrus. Also observed during subsequent memory activation were activations in the occipital pole, lateral occipital cortex, left inferior temporal gyrus, and fusiform cortex.
Pathology of the parieto-occipital and parietal regions was also detected in schizophrenia. When processing tasks involving aversive versus neutral images, the familial at-risk group demonstrated less activation in the anterior cingulate cortex, with reduced activity in the inferior prefrontal and occipital regions of the brain. The decrease in connections between neuronal chains (coupling) was most noticeable between the frontal-parietal cortical areas and subcortical structures, as well as between the frontal and occipital areas. Moreover, increased connectivity was found between limbic and frontal regions, as well as for the temporo-occipital connection.
A study using mapping statistics showed that the severity of delirium is associated with density in the orbitofrontal cortex (Brodmann area 11/47). On the other hand, delusions, flat affect, and antisocial behavior were associated with decreased cortical density in the dorsolateral prefrontal region. Hoptman et al., (2012) studied functional connectivity between homotopic points in the brain using voxel-mirror homoseptic connectivity (VMHC). They examined VMHC from resting-state fMRI data and found significant VMHC reductions in patients in the occipital lobe, thalamus, and cerebellum.
In patients with early onset schizophrenia, atypical decreases in connectivity between the dorsolateral prefrontal cortex and the anterior cingulate cortex, inferior parietal lobule, and middle occipital gyrus have been found. Fujimoto T et al. (2012) conducted a study of patients with schizophrenia, collecting some images in the functional map of event-related desynchronization (ERD) and synchronization (ERS) in the theta, lower alpha (8-10 Hz), upper alpha (10-13 Hz) and beta bands . ERD/ERS changes were noted in left temporal and midline frontal and anterior cortices in theta ERS, occipital lobe in alpha ERS, and right temporofrontal-parietal, midline frontal and anterior cortices in beta ERD. .
Delta waves were studied during sleep in bilateral frontal, central, parietal and occipital regions of the brain. It was noted that patients with schizophrenia had lower levels of total delta waves during nighttime sleep.
Analysis of the psychophysiological interaction of the dorsal anterior cingulate cortex showed that activity in the occipital cortex is associated with poor social change and impaired social cognition (Taylor S., et.al., 2011). In addition, fMRI showed three brain networks that had disrupted connections between neurons in children and adolescents with schizophrenia. These networks included the anterior cingulate and temporal lobes, the cerebellum with subcortical regions, and the occipital lobe and cerebellum. Patients with early onset schizophrenia exhibited abnormal functional connectivity in networks involving temporal lobe, limbic, and cerebellar tracts during early visual processing. Additionally, altered prefrontal-hippocampal and parieto-occipital connectivity have been found to be associated with positive symptoms of schizophrenia, which may have implications when analyzing the pathophysiology of these symptoms.
Patients with schizophrenia exhibit remarkably high state functional connectivity density (rsFCD) in the bilateral striatum and hippocampus and significantly lower rsFCD in the right occipital cortex and bilateral sensorimotor cortex. The connection between the left inferior frontal gyrus and the bilateral occipital cortex is reduced in patients with schizophrenia.
Levels of N-acetylaspartate in the ratio of creatinine (NAA/Cr), in the left basal ganglia and parieto-occipital lobe, were significantly lower in patients with first-episode schizophrenia psychosis than in control subjects. Pro-oxidant xanthine oxidase (XO), which has been shown to play an integral role in purine/adenosine metabolism, is downregulated (XO) in the occipital cortex and thalamus of patients with psychosis.
So, patients with schizophrenia show structural changes (CT, MRI) in the occipital lobe, and some studies show functional changes (fMRI, PET) in this region. On the other hand, some patients experience metabolic changes in the occipital lobe. Moderate quality evidence (due to large sample size and lack of consistency and precision) showed that white matter integrity is reduced in the occipital cortex compared to healthy individuals, moderate to low quality evidence (inconsistent, imprecise) shows that there is a higher frequency abnormal (reverse) asymmetry in the occipital lobe in schizophrenia compared to controls. Progressive changes in gray matter volume have been reported on longitudinal MRI scans. Significantly greater reductions were reported over time in schizophrenia compared with controls (occipital gray matter: 69.9% and occipital white matter: 45.9%).
When solving executive functioning tasks, patients with schizophrenia demonstrate decreased activity in the middle occipital gyrus.
There is no doubt that the occipital lobe is associated with schizophrenia, and abnormalities of the occipital lobe may be important in schizophrenia and related disorders. Structural brain abnormalities in the parietal lobe have been found in imaging studies of childhood onset schizophrenia, suggesting that gray matter abnormalities begin in the parietal and occipital lobes and continue their pathological dynamic “wave” to the frontal cortex.
There are no significant metabolic changes in the brains of patients with schizophrenia. The nature and timing of the pathological processes underlying the structural, functional and metabolic changes in schizophrenia remain unclear. Thus, structural changes in the occipital lobe may occur early in the disease and indicate genetic influences that remain to be determined. Disturbances in neural connections in the circuits of neurons and fiber tracts leading to the occipital lobe are associated with schizophrenia and may indicate a genetic predisposition to this mental disorder. In a post-mortem study of patients with schizophrenia, Selemon et al. (1995) showed an abnormally high density of neurons in the prefrontal and occipital cortex. Previously, the death of neuronal cells was attributed to a decrease in the volume of the gray matter cortex. However, Selemon L, Goldman-Rakic P. (1997) associate the increase in cell density, in the context of reduced volume, with loss of neutrophils or connections between neurons, which may result from “over-pruning” of their processes (excessive pruning).
The importance of proper formation and movement of cerebrospinal fluid for brain function
In a healthy person, the circulation of cerebrospinal fluid (CSF) occurs continuously. It is located not only in the cisterns of the brain, but also in its central cavities. These sections are called the cerebral ventricles. There are several varieties:
- lateral;
- third and fourth (connected by the Sylvian aqueduct).
It is important to note that it is the fourth ventricle that is directly connected to the human spinal cord. Cerebrospinal fluid performs the following functions:
- washes the outer surface of the cortex;
- circulates in the cerebral ventricles;
- penetrates deep into the brain tissue through the cavities around the vessels.
These areas are not only the main area of cerebrospinal fluid circulation, but also its storage. The cerebrospinal fluid itself begins its formation at the junction of the blood vessels of the ventricles. These are small processes that have a velvety surface and are located directly on the walls of the ventricles. There is an inextricable connection between the tank and the cavity around it. When special slits are used, the main tank interacts with the fourth ventricle of the brain. Thus, cerebrospinal fluid is synthesized, which is transported through these gaps to the subarachnoid region.
Among the features of the movement of cerebrospinal fluid are:
- movement in different directions;
- circulation occurs slowly;
- it is influenced by cerebral pulsation and respiratory movements;
- the main amount of cerebrospinal fluid enters the venous bed, the remainder into the lymphatic system;
- directly takes part in metabolic processes between brain tissues and organs.
Assigned functions
The functions of the occipital lobe of the brain are associated with the analysis, perception and containment (storage) of visual information. The visual tract consists of several points:
- An eye with its retina. This paired organ is only a mechanical component of vision, performing an optical function.
- Optic nerves, through which electrical impulses directly travel at a certain frequency and carry certain information.
- The primary centers are represented by the visual thalamus and quadrigeminal.
- Subcortical and cortical centers. All of the above structures act as points of elementary perception and delivery of information. The visual cortex, in contrast, plays the role of a higher analyzer, that is, it processes the received nerve impulses into mental visual images.
It is noteworthy that the retina of the eye perceives a set of light waves, each of which has a length and consists of quanta of electromagnetic radiation. But the cortex, evolving over millions of years, “ learned ” to work with such signals and turn them into something more than a set of energy and impulses. Thanks to this, people have a picture of the environment and the world. Thanks to this crust, we see the elements of the universe as they appear.
The visual cortex, located on both hemispheres of the occipital lobe, provides binocular vision - the world appears three-dimensional to the human eye.
The human brain is a multifunctional structure, like each area of its cortex - therefore, the occipital lobe of the brain in a standard functional state takes little part in processing auditory and tactile signals. Under conditions of damage to neighboring areas, the degree of participation in signal analysis increases.
The visual cortex, called the association area, constantly interacts with other brain structures, forming a complete picture of the world. The occipital lobe has strong connections with the limbic system (especially the hippocampus), parietal and temporal lobes. Thus, a particular visual image may be accompanied by negative emotions, or vice versa: a long-standing visual memory evokes positive feelings.
The occipital lobe, in addition to simultaneous analysis of signals, also plays the role of an information container. However, the amount of such information is small, and most environmental data is stored in the hippocampus.
The occipital cortex is strongly associated with theories of feature integration, the essence of which is that the cortical analytical centers process individual properties of an object (color) both separately, in isolation, and in parallel.
To summarize, we can answer the question of what the occipital lobe is responsible for:
- processing visual information and integrating it into a general attitude towards the world;
- storage of visual information;
- interaction with other areas of the telencephalon and partial succession of their functions;
- binocular perception of the environment.
Symptoms of deformation
The main signs of changes in the size of the tanks are: headache, nausea, blurred vision. As symptoms progress, serious complications develop.
When a large volume of fluid accumulates, the patient is diagnosed with hydrocephalus. It comes in two types:
- internal (cerebrospinal fluid accumulates in the cerebral ventricles);
- external (accumulation is observed in the subarachnoid region).
The main symptoms include morning swelling under the eyes. In this case, an urgent examination by a doctor is required to make an accurate diagnosis. During pregnancy, to exclude disorders of brain development in the child, a mandatory ultrasound examination is performed in the first trimester.
Treatment of diseases associated with deformities
If deformation processes are detected early, drug therapy is carried out. If the amount of accumulated fluid is very large, the patient may require urgent surgery. To do this, a small hole is made in the patient's skull into which a tube is placed. With its help, excess liquid is pumped out. Today, neuroendoscopy is becoming an increasingly popular method, which is performed without the use of additional excretory tubes and does not cause harm to the patient.
Consequences of the disease
In case of chronic hydrocephalus, the patient is registered with a neurologist and regularly undergoes the necessary tests. If treatment is not started on time, hydrocephalus leads to disability in the child. His development is inhibited, he speaks poorly, and his vision functions may be impaired. With timely treatment, doctors note a high recovery rate. If deformations in the cisterns of the brain are diagnosed during intrauterine development, then most likely such a child will be born defective.
Prevention of violations
Most brain development disorders occur during fetal development. You must adhere to the following recommendations:
- try to avoid infectious diseases, especially in the first trimester of pregnancy;
- Take medications with caution.
To prevent the development of hydrocephalus in children, it is necessary to avoid traumatic brain injuries and infectious diseases of the nervous system, since these factors are considered to provoke the development of hydrocephalus.
To maintain the viability of a patient with cistern deformities, doctors prescribe medications and regular examinations. If a deterioration of the condition is suspected, urgent surgical intervention is performed.
Location
The occipital lobe is the region of the telencephalon that is located behind the temporal and parietal lobes. In the occipital lobe of the cerebral cortex there is a central part of the analyzer, namely the visual one. This region of the brain includes the non-constant lateral occipital sulcus, which separates the superior and inferior occipital gyri. Inside this area is the calcarine groove.